You might also like
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Winter Safety Toolbox TalkDocument18 pagesWinter Safety Toolbox TalkKristina100% (1)
- 1cambrigton Dave Ielts Reading 100 9 PointsDocument43 pages1cambrigton Dave Ielts Reading 100 9 PointsWit FksunNo ratings yet
- Enquiry Form Indian Overseas BankDocument3 pagesEnquiry Form Indian Overseas Bankthenambi100% (1)
- Death Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3Document3 pagesDeath Claim Form: CLAIMFORM DC-s Nov2016 v2 Page 1 of 3vertine belerNo ratings yet
- Annex UreDocument8 pagesAnnex Urevijayapathy reddyNo ratings yet
- Application For Survivors Benefits Pension/Provident FundDocument9 pagesApplication For Survivors Benefits Pension/Provident FundXANPHOXYL KIBETNo ratings yet
- Certificate of Identity and Burial or CremationDocument2 pagesCertificate of Identity and Burial or CremationAbhijit AminpurNo ratings yet
- Form 2 Death ReportDocument1 pageForm 2 Death ReportSunilNo ratings yet
- Proof of Death - Claimant StatementDocument2 pagesProof of Death - Claimant Statementlisa marieNo ratings yet
- Annexure III Additional Nomination DetailsDocument2 pagesAnnexure III Additional Nomination Detailsnaveed naahidNo ratings yet
- Claimant's Statement FormDocument2 pagesClaimant's Statement FormRiza Zausa CuarteroNo ratings yet
- Ecosure Death Form Claim: 1. Please Specify Claim TypeDocument1 pageEcosure Death Form Claim: 1. Please Specify Claim TypeMichael-lee MupesaNo ratings yet
- Death Claim Form PDFDocument4 pagesDeath Claim Form PDFSupdt. of Post offices Kanpur (M) Dn. KanpurNo ratings yet
- Attending Physicians Statement Death Claim - 041222Document2 pagesAttending Physicians Statement Death Claim - 041222Lhen TrinidadNo ratings yet
- Death Claim FormDocument4 pagesDeath Claim FormudufkhkfysfkgoNo ratings yet
- Pardon PetitionDocument11 pagesPardon Petitionwarriorsinrecoveryalex.rNo ratings yet
- A616d0fc152d4e - 1634537409 - Sample Compliance Forms-DelhiveryDocument8 pagesA616d0fc152d4e - 1634537409 - Sample Compliance Forms-Delhiverypriyanshi11090No ratings yet
- Death Claim Form RSA: For Death/Final Expenses/ Funeral ClaimsDocument4 pagesDeath Claim Form RSA: For Death/Final Expenses/ Funeral ClaimsMartha MtikaNo ratings yet
- PODO - HR Form No. 02 - Employment Application FormDocument3 pagesPODO - HR Form No. 02 - Employment Application FormAbseiling BMSNo ratings yet
- Form DA 1 Addition of NominationDocument1 pageForm DA 1 Addition of Nominationranji1979100% (2)
- St. Peter Life Plan, Inc: (State Relationship To Deceased)Document1 pageSt. Peter Life Plan, Inc: (State Relationship To Deceased)Janice SobejanoNo ratings yet
- Form 700Document4 pagesForm 700Abhishek ChattopadhyayNo ratings yet
- Forml1 1aDocument4 pagesForml1 1aEmily ChowNo ratings yet
- Colour Photo of The Life To Be AssuredDocument12 pagesColour Photo of The Life To Be AssuredshahnawazNo ratings yet
- 680 DGHDocument4 pages680 DGHjdchandrapal4980No ratings yet
- Form FDocument2 pagesForm FTeck EngineerNo ratings yet
- Great ThinkDocument2 pagesGreat ThinkjituNo ratings yet
- LIC Proposal Form - 340 - Revised - 01 02 2020Document11 pagesLIC Proposal Form - 340 - Revised - 01 02 2020Choudhary YTNo ratings yet
- Declaration by The Primary Resident: Permission To Register at An AddressDocument1 pageDeclaration by The Primary Resident: Permission To Register at An AddressPublinet Mentes CreativasNo ratings yet
- Form FDocument3 pagesForm FJaganath RaviNo ratings yet
- Form No. SH-14Document2 pagesForm No. SH-14Hilal KhanNo ratings yet
- Creditfile AppDocument1 pageCreditfile Appchunzhimoe233No ratings yet
- Form ADocument1 pageForm AAbhijit SarkarNo ratings yet
- Checklist of Req. For LA and Substitution of ADocument2 pagesChecklist of Req. For LA and Substitution of Athechieftain95No ratings yet
- Form-No-700 English 0 PDFDocument4 pagesForm-No-700 English 0 PDFMallappa.B MadihalliNo ratings yet
- Form-F-Nomination-Gratuity SampleDocument3 pagesForm-F-Nomination-Gratuity SampleVENKATESAN BNo ratings yet
- Application For Deceased Claim 4Document2 pagesApplication For Deceased Claim 4anishek guptaNo ratings yet
- Nsi VerificationDocument3 pagesNsi Verificationatotayi007No ratings yet
- Member Enrolment Form-GTL-without Addendum-19 Nov 2018Document2 pagesMember Enrolment Form-GTL-without Addendum-19 Nov 2018Rajesh MukkavilliNo ratings yet
- Nominee 1Document1 pageNominee 1ravimaiinNo ratings yet
- Sample Gratuity-Nomination-Form-FDocument2 pagesSample Gratuity-Nomination-Form-FAnkit0% (1)
- Manappuram Group of Companies, ValapadDocument6 pagesManappuram Group of Companies, Valapadpawakumar9043No ratings yet
- NominationsDocument4 pagesNominationsAngsuman SenguptaNo ratings yet
- YVOP Form FINALDocument3 pagesYVOP Form FINALJoshua O. ApuyaNo ratings yet
- Name of The Person Making Nomination 2. Father's/Husband's Name 3. Date of Birth 4. Sex 5. Marital Status 6. Address A) Permanent B) TemporaryDocument2 pagesName of The Person Making Nomination 2. Father's/Husband's Name 3. Date of Birth 4. Sex 5. Marital Status 6. Address A) Permanent B) TemporaryYash SellsNo ratings yet
- Transferee Information Sheet (Dar Requirements)Document2 pagesTransferee Information Sheet (Dar Requirements)my little wanderNo ratings yet
- Annexure I FORM NO. 3783 Claim Form A' Life Insurance Corporation of IndiaDocument3 pagesAnnexure I FORM NO. 3783 Claim Form A' Life Insurance Corporation of IndiaSharang Paruthi0% (1)
- Affidavit Blank TemplateDocument3 pagesAffidavit Blank TemplateCampbell McKenzieNo ratings yet
- Nomination Cancellation FormDocument1 pageNomination Cancellation FormAdv Ratnesh DubeNo ratings yet
- LIC Claim Form B 3784 Medical Attendant's CertificateDocument3 pagesLIC Claim Form B 3784 Medical Attendant's Certificategdbdgbd xc v xvNo ratings yet
- TALIC Part A EPF & Part B EPS Nomination FormDocument2 pagesTALIC Part A EPF & Part B EPS Nomination FormAvdhesh Singh RajpootNo ratings yet
- Form 340 - Feb 2021Document11 pagesForm 340 - Feb 2021PREM MURUGANNo ratings yet
- Advocate Data Sheet For Filing CasesDocument1 pageAdvocate Data Sheet For Filing CasesSundararajan Sathyamurthi100% (1)
- Form 2: Part A (Epf)Document3 pagesForm 2: Part A (Epf)Nikhil KulkarniNo ratings yet
- Form F - GratuityDocument2 pagesForm F - Gratuityriyanofficial513No ratings yet
- 5 Agreement of Adoption of Nonminor DependentDocument1 page5 Agreement of Adoption of Nonminor Dependentjaydourman2020No ratings yet
- Form SH 13 - NominationDocument3 pagesForm SH 13 - NominationKrunalNo ratings yet
- Joining Kit: First Name Middle NameDocument20 pagesJoining Kit: First Name Middle NameDNYANESHWAR PAWARNo ratings yet
- Legal Practitioners Examination 6-97 AnswersDocument4 pagesLegal Practitioners Examination 6-97 AnswersAndré Le RouxNo ratings yet
- Online Term Plan: Shriram LifeDocument10 pagesOnline Term Plan: Shriram LifeSivaramakrishna DavuluriNo ratings yet
- Shriram Life InsuranceDocument12 pagesShriram Life InsuranceSivaramakrishna DavuluriNo ratings yet
- Brochure Shriram Assured Income Plan OfflineDocument7 pagesBrochure Shriram Assured Income Plan OfflineSivaramakrishna DavuluriNo ratings yet
- A Study On Consumer Perception About Life InsuranceDocument63 pagesA Study On Consumer Perception About Life Insurancekundanky@live.in82% (44)
- A Comprehensive Project Report Factors Affecting Consumer Purchase Decision of Laptops"Document79 pagesA Comprehensive Project Report Factors Affecting Consumer Purchase Decision of Laptops"nithish patkarNo ratings yet
- Shriram Life Insurance Company Limited Claim Form "A": Divisional Office: Branch OfficeDocument3 pagesShriram Life Insurance Company Limited Claim Form "A": Divisional Office: Branch OfficeSivaramakrishna DavuluriNo ratings yet
- Shriram Life InsuranceDocument12 pagesShriram Life InsuranceSivaramakrishna DavuluriNo ratings yet
- Shriram Life InsuranceDocument12 pagesShriram Life InsuranceSivaramakrishna DavuluriNo ratings yet
- Shriram Life InsuranceDocument12 pagesShriram Life InsuranceSivaramakrishna DavuluriNo ratings yet
- Brochure Shriram Assured Income Plus OnlineDocument12 pagesBrochure Shriram Assured Income Plus OnlineSivaramakrishna Davuluri100% (1)
- Myocardial Protection - An UpdateDocument67 pagesMyocardial Protection - An UpdateRezwanul Hoque Bulbul100% (5)
- Nuevas Patologias Cie 10Document281 pagesNuevas Patologias Cie 10Ana guely santivañez mitmaNo ratings yet
- YMCA Program Guide - 2016Document44 pagesYMCA Program Guide - 2016Pickens County YMCANo ratings yet
- Approach To The Patient in Shock: by James Holencik, DODocument52 pagesApproach To The Patient in Shock: by James Holencik, DOLydia MamurNo ratings yet
- Job Safety Analysis: Abqaiq Plants OperationDocument5 pagesJob Safety Analysis: Abqaiq Plants OperationZia ur RehmanNo ratings yet
- Impaired Posture and MovementDocument40 pagesImpaired Posture and MovementMohamed Magdy ElMeligieNo ratings yet
- Jhs Learner DataDocument3 pagesJhs Learner Dataapi-377500541No ratings yet
- Ion Breeding Policy - 2006 & 2010Document42 pagesIon Breeding Policy - 2006 & 2010Ulhas GaikwadNo ratings yet
- Bahasa Inggris Swot Madam Gie Sweet Cheek BlushedDocument8 pagesBahasa Inggris Swot Madam Gie Sweet Cheek Blushedanon_681594518No ratings yet
- Levels of PreventionDocument23 pagesLevels of Preventionkuruvagadda sagar100% (1)
- Alice in Michigan: A Financial Hardship StudyDocument58 pagesAlice in Michigan: A Financial Hardship StudydaneNo ratings yet
- A Handbook of Dementia Care: Edited byDocument15 pagesA Handbook of Dementia Care: Edited byJovana Ognenovska Bakalovska100% (1)
- Indian Research Funding AgenciesDocument6 pagesIndian Research Funding AgencieskcchtphdNo ratings yet
- Policy That Implemented in Kota SamarahanDocument9 pagesPolicy That Implemented in Kota SamarahanIskandar IskandarNo ratings yet
- Suplemento 1Document56 pagesSuplemento 1Dessirhe LaraNo ratings yet
- Primary Eye Care-A Manual For Health WorkersDocument76 pagesPrimary Eye Care-A Manual For Health WorkersRHU LOOCNo ratings yet
- Rajasthan Hospitals LISTDocument19 pagesRajasthan Hospitals LISTOrigin Over100% (1)
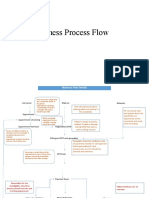
- Business Process FlowDocument12 pagesBusiness Process FlowKumar BalramNo ratings yet
- 48069B - Ferrofos 5260 (GB-ENG)Document6 pages48069B - Ferrofos 5260 (GB-ENG)danielNo ratings yet
- Tienchi Ginseng Panax Notoginseng San Qircljo PDFDocument4 pagesTienchi Ginseng Panax Notoginseng San Qircljo PDFTobiasenHolgersen89No ratings yet
- Muhanga District Development Plan 2013-2018-1 01Document116 pagesMuhanga District Development Plan 2013-2018-1 01Joseph Tuseku Officiel100% (1)
- Fundamentalism Vaccine FunVaxDocument35 pagesFundamentalism Vaccine FunVaxCathy Ann100% (1)
- Persuasive Speech OutlineDocument5 pagesPersuasive Speech Outlineapi-256458286No ratings yet
- Responsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFDocument64 pagesResponsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFPyae PyaeNo ratings yet
- The Emergence of India's Pharmaceutical IndustryDocument41 pagesThe Emergence of India's Pharmaceutical Industryvivekgupta2jNo ratings yet
- Persona Partial Knee Brochure PDFDocument12 pagesPersona Partial Knee Brochure PDF洪侊增No ratings yet
- UJA-Federation of New York Donor Recognition List 2022Document17 pagesUJA-Federation of New York Donor Recognition List 2022ericlkaplanNo ratings yet
- Rickets - A Brief View With Homoeopathic ApproachDocument32 pagesRickets - A Brief View With Homoeopathic ApproachDr. Sandeep Anwane100% (1)