You might also like
- Lab Act 2 SensoryDocument5 pagesLab Act 2 SensoryZgama AbdulrahmanNo ratings yet
- Annual Report (Latest)Document105 pagesAnnual Report (Latest)Lester Anonuevo100% (1)
- Philippine Nursing Seminars and Training January 2011Document2 pagesPhilippine Nursing Seminars and Training January 2011PhilippineNursingDirectory.com100% (1)
- COPAR Stray DogsDocument3 pagesCOPAR Stray DogsMicaela Andrea CieloNo ratings yet
- Program PlanDocument6 pagesProgram Planapi-271124825No ratings yet
- Effects of AnxietyDocument4 pagesEffects of AnxietyEdelrose LapitanNo ratings yet
- Maed101 Research ProposalDocument40 pagesMaed101 Research ProposalCRestine Joy Elmido MonteroNo ratings yet
- 5.psychosocial Aspects of Health and DiseaseDocument30 pages5.psychosocial Aspects of Health and DiseaseFaisal MehboobNo ratings yet
- 2011-0021 22 Research MethodologyDocument18 pages2011-0021 22 Research Methodologyahmedbalo100% (1)
- Health Fitness in Motion: A Community Engagement Proposal For Locality of Gasak Foster Health AwarenessDocument3 pagesHealth Fitness in Motion: A Community Engagement Proposal For Locality of Gasak Foster Health AwarenessJanna MangaliliNo ratings yet
- Physician Letter - Heart FailureDocument2 pagesPhysician Letter - Heart FailurepatweavaNo ratings yet
- Proposing A Solution Teenage PregnancyDocument5 pagesProposing A Solution Teenage PregnancyJacques OwokelNo ratings yet
- Research Paper About EpilepsyDocument4 pagesResearch Paper About EpilepsyHazel Anne Joyce Antonio100% (1)
- ResearchDocument8 pagesResearchKiana RamosaNo ratings yet
- Discuss Surgical Management of Cerebral Palsy - 000Document72 pagesDiscuss Surgical Management of Cerebral Palsy - 000SamNo ratings yet
- Community Based Rehabilitation in Vietnam PDFDocument13 pagesCommunity Based Rehabilitation in Vietnam PDFsaycrNo ratings yet
- Case Study, Chapter 9, Assessing Pain: The Fifth Vital SignDocument1 pageCase Study, Chapter 9, Assessing Pain: The Fifth Vital Signclyde i amNo ratings yet
- Paper Battery SeminarDocument27 pagesPaper Battery SeminarPritjot GillNo ratings yet
- Mental Health Is Defined As "A State of Well-Being in Which Every IndividualDocument7 pagesMental Health Is Defined As "A State of Well-Being in Which Every IndividualmejulNo ratings yet
- Reflection Paper Darren CarinoDocument2 pagesReflection Paper Darren CarinoDarren CariñoNo ratings yet
- Communicating With Adolescents Power PointDocument16 pagesCommunicating With Adolescents Power PointNuma WadhwaniaNo ratings yet
- THE LEVEL OF AWARENESS AMONG THE TEENAGE MOTHERS OF TUBIGON, BOHOL IN RENDERING NEWBORN CARE (Part 1)Document13 pagesTHE LEVEL OF AWARENESS AMONG THE TEENAGE MOTHERS OF TUBIGON, BOHOL IN RENDERING NEWBORN CARE (Part 1)Wuawie MemesNo ratings yet
- Assessment in The K To 12 BEP (National)Document44 pagesAssessment in The K To 12 BEP (National)Santa Dela Cruz NaluzNo ratings yet
- Medical & Surgical Management in Cerebral PalsyDocument13 pagesMedical & Surgical Management in Cerebral PalsySahil SahniNo ratings yet
- Narrative Report 1Document5 pagesNarrative Report 1geraldine amahidoNo ratings yet
- Sona Position PaperDocument5 pagesSona Position PaperFrancis BorromeoNo ratings yet
- Impairment, Disability and HandicapDocument9 pagesImpairment, Disability and HandicapSHIBU PRASAD SAHOONo ratings yet
- Nursing DiagnosisDocument5 pagesNursing DiagnosisGeovanni Rai HermanoNo ratings yet
- Social Problems in The Philippines I-Witness: "Black Manila", A Documentary by Howie SeverinoDocument1 pageSocial Problems in The Philippines I-Witness: "Black Manila", A Documentary by Howie SeverinoMhelai Dela CruzNo ratings yet
- Learn To PredictDocument1 pageLearn To PredictKelley WalkerNo ratings yet
- The ThesisDocument8 pagesThe ThesisTerraMonsta BlogspotNo ratings yet
- RRL - Mobile PhonesDocument3 pagesRRL - Mobile Phonesarvin jay sacilNo ratings yet
- EUTHENICS LECTURE Week 1 To 5Document5 pagesEUTHENICS LECTURE Week 1 To 5Cyra BanzonNo ratings yet
- Narrative ReportDocument1 pageNarrative Report14markianneNo ratings yet
- Worktext (TCW) Chapter 3 Global InterstateDocument9 pagesWorktext (TCW) Chapter 3 Global InterstateAlthea Faye RabanalNo ratings yet
- PMLS Narrative Report PDFDocument14 pagesPMLS Narrative Report PDFGilmar ManzanoNo ratings yet
- Drug EducationDocument10 pagesDrug Educationไลมทด ระดมNo ratings yet
- Visual ImpairmentDocument7 pagesVisual ImpairmentROSE MARIE REVILLA100% (1)
- NSTP 200 - Edited But Not Yet FinalDocument20 pagesNSTP 200 - Edited But Not Yet FinalmjNo ratings yet
- Developing A Teaching PlanDocument6 pagesDeveloping A Teaching PlanAntonette Africa MercadoNo ratings yet
- Research ProposalDocument79 pagesResearch ProposalMARVIN BALLENASNo ratings yet
- Thesis Sample Chapter 1Document5 pagesThesis Sample Chapter 1Romie SolacitoNo ratings yet
- Physical Fitness NotesDocument11 pagesPhysical Fitness NotesAlbirk Vonz AgudoNo ratings yet
- MessagesDocument4 pagesMessagesBradTimwell DizonNo ratings yet
- Synthesis PaperDocument4 pagesSynthesis PaperEthan FreemanNo ratings yet
- ThesisDocument11 pagesThesismae santosNo ratings yet
- 1-Opening and Welcome SpeechDocument2 pages1-Opening and Welcome SpeechNavneet K. PatilNo ratings yet
- Sample of A Community Activity ProposalDocument4 pagesSample of A Community Activity ProposalChristian Keruel Yuson Laurente100% (1)
- Availability of Laboratory Facilities For Effective Teaching-Learning of Social Studies in Atbcoe KangereDocument25 pagesAvailability of Laboratory Facilities For Effective Teaching-Learning of Social Studies in Atbcoe KangereShuaibu YunusaNo ratings yet
- Iv Therapy With Edited RationaleDocument5 pagesIv Therapy With Edited RationaleKysha HuangNo ratings yet
- Acute Respiratory InfectionDocument68 pagesAcute Respiratory InfectionArun GeorgeNo ratings yet
- CHAPTER 1 Thesis HiSTORICALDocument8 pagesCHAPTER 1 Thesis HiSTORICALRomae AlimaniaNo ratings yet
- Assessment in Special EdDocument27 pagesAssessment in Special EdAlfred IntongNo ratings yet
- Lesson 5Document16 pagesLesson 5Vũ Hồng NgọcNo ratings yet
- Technology Good or BadDocument3 pagesTechnology Good or BadRohit Gupta100% (1)
- The Developmental Stages of The LearnerDocument56 pagesThe Developmental Stages of The LearnerJianne CaloNo ratings yet
- Questionnaire Survey Bases Awareness and Knowledge of Glaucoma Among Adult Patient in Rural and Urban Area in RaipurDocument3 pagesQuestionnaire Survey Bases Awareness and Knowledge of Glaucoma Among Adult Patient in Rural and Urban Area in RaipurInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Collaborative Paper On Issues and Concerns in Philippine Deaf EducationDocument35 pagesA Collaborative Paper On Issues and Concerns in Philippine Deaf EducationSeresa LegaspiNo ratings yet
- NCM 101 Midterm NotessDocument294 pagesNCM 101 Midterm NotessJude Marie Claire DequiñaNo ratings yet
- Handout I - Pathophysiology and Types of Burns PDFDocument5 pagesHandout I - Pathophysiology and Types of Burns PDFdivinaNo ratings yet
- I.W. Crandon Section of Surgery Division of Neurosurgery University of The West IndiesDocument38 pagesI.W. Crandon Section of Surgery Division of Neurosurgery University of The West IndiesdivinaNo ratings yet
- Congenital Lesions. PhysiotherapistsDocument9 pagesCongenital Lesions. PhysiotherapistsdivinaNo ratings yet
- Lecture. Physiotherapists. TumoursDocument34 pagesLecture. Physiotherapists. TumoursdivinaNo ratings yet
- Abscesses Lecture - Physiotherapists. 2012Document24 pagesAbscesses Lecture - Physiotherapists. 2012divinaNo ratings yet
- What Is Physical Therapy?: For The Orthopedic SurgeonDocument6 pagesWhat Is Physical Therapy?: For The Orthopedic SurgeondivinaNo ratings yet
- Below Elbow AmputationDocument11 pagesBelow Elbow AmputationdivinaNo ratings yet
- Sclerodactyly, and Telangiectasis) Syndrome Accompany-: Cor PulmonaleDocument2 pagesSclerodactyly, and Telangiectasis) Syndrome Accompany-: Cor PulmonaledivinaNo ratings yet
- 2017 Rehab ShoulderDocument11 pages2017 Rehab ShoulderRizka ApNo ratings yet
- Applied Anatomy: Head and NeckDocument9 pagesApplied Anatomy: Head and NeckdivinaNo ratings yet
- Interferential Therapy Electrode Placement Techni-3 PDFDocument9 pagesInterferential Therapy Electrode Placement Techni-3 PDFdivinaNo ratings yet
- 10 5923 J Sports 20190903 02 PDFDocument7 pages10 5923 J Sports 20190903 02 PDFdivinaNo ratings yet
- Neurology Course OutlineDocument1 pageNeurology Course OutlinedivinaNo ratings yet
- 2 8 33 124 PDFDocument4 pages2 8 33 124 PDFdivinaNo ratings yet
- Cervical Myelopathy - StatPearls - NCBI BookshelfDocument5 pagesCervical Myelopathy - StatPearls - NCBI BookshelfdivinaNo ratings yet
- Agur, A. M. R. - Dalley, Arthur F. - Moore, Keith L. - Clinically Oriented Anatomy-Wolters Kluwer Health - Lippincott Williams & Wilkins (2014) (Dragged) PDFDocument3 pagesAgur, A. M. R. - Dalley, Arthur F. - Moore, Keith L. - Clinically Oriented Anatomy-Wolters Kluwer Health - Lippincott Williams & Wilkins (2014) (Dragged) PDFdivinaNo ratings yet
- Direct Black 22Document4 pagesDirect Black 22DHRUVNo ratings yet
- Family Systems Therapy and AddictionDocument30 pagesFamily Systems Therapy and AddictionthegavmanNo ratings yet
- EMP Procedure in MalaysiaDocument24 pagesEMP Procedure in Malaysialamkinpark3373No ratings yet
- Assignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Document3 pagesAssignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Hafshah AgustinaNo ratings yet
- Prevalence of High Risk Pregnancy in Rural DharwadDocument4 pagesPrevalence of High Risk Pregnancy in Rural DharwadIOSRjournalNo ratings yet
- Responsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFDocument64 pagesResponsible Tourism in Myanmar Current Situation and Challenges Red - 2 PDFPyae PyaeNo ratings yet
- Flux Cored Arc Welding NC IIDocument73 pagesFlux Cored Arc Welding NC IIAJ AcuñaNo ratings yet
- Ergonomic Factors in Construction Industry: A Literature ReviewDocument14 pagesErgonomic Factors in Construction Industry: A Literature ReviewdhanarajNo ratings yet
- Bus Man Unit 3 SAC 3Document13 pagesBus Man Unit 3 SAC 3Mohamad ZackuanNo ratings yet
- ARC 360 NGP InstructionManualDocument24 pagesARC 360 NGP InstructionManualLMTNo ratings yet
- Rickets - A Brief View With Homoeopathic ApproachDocument32 pagesRickets - A Brief View With Homoeopathic ApproachDr. Sandeep Anwane100% (1)
- UJA-Federation of New York Donor Recognition List 2022Document17 pagesUJA-Federation of New York Donor Recognition List 2022ericlkaplanNo ratings yet
- PMDC Community Medicine Mcqs PDFDocument280 pagesPMDC Community Medicine Mcqs PDFJay KNo ratings yet
- Complete Guide To Communication Problems After StrokeDocument22 pagesComplete Guide To Communication Problems After Strokeapi-215453798100% (1)
- Valid RRR Application 2013 - 2017 PDFDocument22,467 pagesValid RRR Application 2013 - 2017 PDFAyub NaveedNo ratings yet
- Sattvika Dite-YakubDocument6 pagesSattvika Dite-Yakubyakubjacob100% (1)
- Circadian RhythmsDocument2 pagesCircadian RhythmsOmar Saleh100% (1)
- Notes On Critical Areas in Labor Law Part IiDocument66 pagesNotes On Critical Areas in Labor Law Part IipaulNo ratings yet
- Internal Audit Ratings GuideDocument19 pagesInternal Audit Ratings Guidesanranist2100% (3)
- The Daily Tar Heel For April 12, 2016Document8 pagesThe Daily Tar Heel For April 12, 2016The Daily Tar HeelNo ratings yet
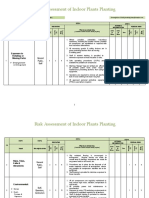
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Respaper 1Document48 pagesRespaper 1Xayezi AblenNo ratings yet
- Chapter 01Document22 pagesChapter 01kita5437100% (1)
- House Bill 15-1043Document19 pagesHouse Bill 15-1043Michael_Lee_RobertsNo ratings yet
- List of CosmeticsDocument9 pagesList of Cosmeticsasit_m0% (1)
- Xcelera Brochure Updated (English)Document24 pagesXcelera Brochure Updated (English)Pablo Rosas100% (1)
- Position Paper TopicsDocument2 pagesPosition Paper TopicskinodecuirNo ratings yet
- TermDocument3 pagesTermapi-308717184No ratings yet
- Sagar SinghDocument4 pagesSagar SinghzombieNo ratings yet
- Research Proposal-1Document28 pagesResearch Proposal-1sowsthikaNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)