You might also like
- Risk RegisterDocument15 pagesRisk Registerdammy0% (1)
- MCQ PhysiotherapyDocument5 pagesMCQ PhysiotherapyAnonymous nXU3ahQEbf100% (2)
- Area Classification: (IEC/EN 60529)Document1 pageArea Classification: (IEC/EN 60529)nestkwt1No ratings yet
- 1mg 1573884813954 PDFDocument2 pages1mg 1573884813954 PDFpavan mantriNo ratings yet
- EMP - Environmental Risk RegisterDocument23 pagesEMP - Environmental Risk RegisterNaveen ChaudharyNo ratings yet
- Base de Données 11Document501 pagesBase de Données 11OsagonaNo ratings yet
- Crec Masterlist Format V7Document41 pagesCrec Masterlist Format V7John Dalton Marin VelascoNo ratings yet
- Pharma Co ListDocument7 pagesPharma Co ListRafeek ShaikhNo ratings yet
- Status and Order ChangeDocument1 pageStatus and Order ChangeSAUTOTNo ratings yet
- Omalizumab in DermatologyDocument35 pagesOmalizumab in DermatologyDeval MistryNo ratings yet
- Antimicrobial Susceptibility TestDocument4 pagesAntimicrobial Susceptibility TestMATTHEW EARL MALUMAY100% (1)
- Risk Assesmen LaboratDocument7 pagesRisk Assesmen LaboratAlfianck Premis IDNo ratings yet
- ILNAS-EN 17141:2020: Cleanrooms and Associated Controlled Environments - Biocontamination ControlDocument9 pagesILNAS-EN 17141:2020: Cleanrooms and Associated Controlled Environments - Biocontamination ControlBLUEPRINT Integrated Engineering Services0% (1)
- 4639 CB 5 B 2Document1 page4639 CB 5 B 2Moussa Ag Mohamed AlyNo ratings yet
- JV Agreement Block 488Document10 pagesJV Agreement Block 488abdulhaiahmadzaiNo ratings yet
- 1002 1257004427 Uganda-UnitsDocument1 page1002 1257004427 Uganda-UnitsAYUSHNo ratings yet
- AISI 1045 Medium Carbon SteelDocument9 pagesAISI 1045 Medium Carbon SteelFatih BahşiNo ratings yet
- Resina HojaDocument2 pagesResina HojaChristian Jesus Jacobo CornejoNo ratings yet
- Mineral Occurence Map of Uganda - A3Document1 pageMineral Occurence Map of Uganda - A3noreply.otimsNo ratings yet
- Pe PDFDocument2 pagesPe PDFPiyush kumarNo ratings yet
- Winter Seat Price Plan 201718 PDFDocument1 pageWinter Seat Price Plan 201718 PDFmeryNo ratings yet
- IPA Blackball RulesDocument1 pageIPA Blackball RulesTumalanoNo ratings yet
- PCTEL MYA93012 896-970 MHZ 11dB 12 Element Yagi Antenna - TESSCODocument1 pagePCTEL MYA93012 896-970 MHZ 11dB 12 Element Yagi Antenna - TESSCOGabriel Montoya CorreaNo ratings yet
- October AccomplishmentDocument17 pagesOctober AccomplishmentReyma GalingganaNo ratings yet
- Republic of The Philippines Department of Education Region VI-Western VisayasDocument1 pageRepublic of The Philippines Department of Education Region VI-Western VisayasMa. Rosadelle LontesNo ratings yet
- MERICON™ I, II, III - Caustic Treatments - Merichem - IDocument1 pageMERICON™ I, II, III - Caustic Treatments - Merichem - IOthman Mat YamanNo ratings yet
- FWCMS Equota - Document List - Ver1.3Document1 pageFWCMS Equota - Document List - Ver1.3Jayson TeeNo ratings yet
- LRK 15423097964-1Document45 pagesLRK 15423097964-1Shujat AbroNo ratings yet
- Result of Compaction Test: Lab Geoteknik (Formulir)Document1 pageResult of Compaction Test: Lab Geoteknik (Formulir)eka krisnantoNo ratings yet
- Report JaundiceDocument2 pagesReport JaundiceVishal KumarNo ratings yet
- Qatar: Persian GulfDocument1 pageQatar: Persian Gulfhassanzafar9090No ratings yet
- Format Table of Specification TemplateDocument2 pagesFormat Table of Specification Templategleen barrientosNo ratings yet
- MERICON™ I, II, III - Caustic Treatments - Merichem - IIDocument1 pageMERICON™ I, II, III - Caustic Treatments - Merichem - IIOthman Mat YamanNo ratings yet
- 1 Azad Nagar, Kanpur 2 Kidwai Nagar, Kanpur: Dr. Ajay Kumar Verma (Ms-Pipri - Up@esic - Nic.in)Document1 page1 Azad Nagar, Kanpur 2 Kidwai Nagar, Kanpur: Dr. Ajay Kumar Verma (Ms-Pipri - Up@esic - Nic.in)Ajay Kumar VermaNo ratings yet
- Tagged SelfDocument2 pagesTagged Selfmohsin shaikhNo ratings yet
- Buy Titan Media Culture, Microbiological Media, Biological ProductsDocument4 pagesBuy Titan Media Culture, Microbiological Media, Biological ProductsMymicrolabNo ratings yet
- Akola Vasai Girgaon Dadar Borivali Andheri: 7:00 - 9:00 AM VE-4Document1 pageAkola Vasai Girgaon Dadar Borivali Andheri: 7:00 - 9:00 AM VE-4Pratham AbadNo ratings yet
- Mumbai Two PDFDocument1 pageMumbai Two PDFshreyaan SharmaNo ratings yet
- Semiconductor Sector Update: Kick Starting The NKEA-15/10/2010Document2 pagesSemiconductor Sector Update: Kick Starting The NKEA-15/10/2010Rhb InvestNo ratings yet
- Azeem LedDocument5 pagesAzeem LedMuzammil AhmadNo ratings yet
- Jefferson County Vaccination Report Feb. 8, 2021Document1 pageJefferson County Vaccination Report Feb. 8, 2021NewzjunkyNo ratings yet
- Multan District Reference Map September 2014Document1 pageMultan District Reference Map September 2014Sadia SamiNo ratings yet
- 2n Trim IngDocument3 pages2n Trim IngMireia MontolioNo ratings yet
- HBW-BirdLife Checklist Version 3-1 PDFDocument1,648 pagesHBW-BirdLife Checklist Version 3-1 PDFArieloOrDieNo ratings yet
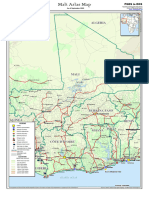
- The Middle East Atlas Map 2007Document1 pageThe Middle East Atlas Map 2007correasherwin007No ratings yet
- Mandate ChartDocument1 pageMandate Chartflyer fighterNo ratings yet
- Tetric EvoFlow Bulk FillDocument48 pagesTetric EvoFlow Bulk FillJuanTabarésNo ratings yet
- BirdLife Checklist Version 9.1PDF PDFDocument535 pagesBirdLife Checklist Version 9.1PDF PDFSanjeev ChoudharyNo ratings yet
- Bildschirmfoto 2022-05-08 Um 11.39.35Document1 pageBildschirmfoto 2022-05-08 Um 11.39.35Giorgi AlimbarashviliNo ratings yet
- Nazara Technologies: A Perspective Unlisted FinancialsDocument4 pagesNazara Technologies: A Perspective Unlisted FinancialsTushar GargNo ratings yet
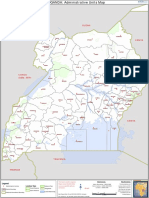
- United Republic of Tanzania Atlas Map: UgandaDocument1 pageUnited Republic of Tanzania Atlas Map: UgandaVincent Deodath Bang'araNo ratings yet
- Digital Marketing Question PaperDocument1 pageDigital Marketing Question PaperVeeram KarnawatNo ratings yet
- Afar Geophy Survey 2005 FINALDocument28 pagesAfar Geophy Survey 2005 FINALVaishnavi BherdeNo ratings yet
- Bangladesh S Intended Nationally Determined Contributions 'Document2 pagesBangladesh S Intended Nationally Determined Contributions 'Tahmina SultanaNo ratings yet
- Energy Efficient Airconditioners - Carrier PhilippinesDocument3 pagesEnergy Efficient Airconditioners - Carrier PhilippinespogisimpatikoNo ratings yet
- Area Classification: (IEC/EN 60529)Document1 pageArea Classification: (IEC/EN 60529)Ku BonNo ratings yet
- 1KD Ecu PDF Manufactured Goods Vehicle PartsDocument1 page1KD Ecu PDF Manufactured Goods Vehicle Partsset paing minNo ratings yet
- Tos TemplateDocument2 pagesTos TemplatekristelNo ratings yet
- Sample TC 256Document2 pagesSample TC 256santanushee8No ratings yet
- Screenshot 2023-03-13 at 07.36.55 PDFDocument1 pageScreenshot 2023-03-13 at 07.36.55 PDFGondeR ???No ratings yet
- Gassing of Insulating Liquid Under Electric Stress AND - I. Ionization IDocument6 pagesGassing of Insulating Liquid Under Electric Stress AND - I. Ionization IShyam K PatelNo ratings yet
- UntitledDocument2 pagesUntitledKhan ShahrukhNo ratings yet
- Aspect-Impact For LabDocument1 pageAspect-Impact For Labvipulsharma655No ratings yet
- GF Arsh PDFDocument1 pageGF Arsh PDFAKASH DAYALNo ratings yet
- Market Data Update January 2017Document11 pagesMarket Data Update January 2017Saadaq AbdirahmanNo ratings yet
- Summer07 Design ProjectsDocument8 pagesSummer07 Design ProjectsvinuvenuNo ratings yet
- 2033 Rheumatoid Arthritis 14-1 PDFDocument48 pages2033 Rheumatoid Arthritis 14-1 PDFAfif Al FatihNo ratings yet
- HTN Topic DiscussionDocument7 pagesHTN Topic Discussionapi-668844754No ratings yet
- Globapharm: Start Case StudyDocument5 pagesGlobapharm: Start Case Studyeh07No ratings yet
- Introduction To Gliclazide TabletsDocument6 pagesIntroduction To Gliclazide TabletsSucharitaNo ratings yet
- Conquering Methicillin Resistant Staphylococcus Aureus: Perspectives and Treatment OptionsDocument7 pagesConquering Methicillin Resistant Staphylococcus Aureus: Perspectives and Treatment OptionsInternational Medical PublisherNo ratings yet
- Rosalie Ragotero Alindogan: # 49 Sitio Dalig LLL Brgy. Dalig Antipolo City 099-75064623Document2 pagesRosalie Ragotero Alindogan: # 49 Sitio Dalig LLL Brgy. Dalig Antipolo City 099-75064623Jamrhose Ragotero AlindoganNo ratings yet
- Pharmacology Assignment: Student's NameDocument6 pagesPharmacology Assignment: Student's NameMosesNo ratings yet
- Michael Chuka OkosaDocument5 pagesMichael Chuka OkosaKaisun TeoNo ratings yet
- A Tutorial For Developing A Topical Cream Formulation Based On The Quality by Design ApproachDocument11 pagesA Tutorial For Developing A Topical Cream Formulation Based On The Quality by Design ApproachMuhamad HilkaNo ratings yet
- PCQI BrouchureDocument6 pagesPCQI BrouchuresuchivapgmailcomNo ratings yet
- LBS Item List 23.01.2020Document30 pagesLBS Item List 23.01.2020Suresh ThanneruNo ratings yet
- FM 11.14.18 - ANGELINA County - State Court Complaint - FINALDocument221 pagesFM 11.14.18 - ANGELINA County - State Court Complaint - FINALAshley SlaytonNo ratings yet
- Cultivation of Medicinal PlantsDocument7 pagesCultivation of Medicinal PlantsgishaqNo ratings yet
- Uniformity of Dosage Units BP 2011 & USP 34Document26 pagesUniformity of Dosage Units BP 2011 & USP 34Anonymous SDUIPeqXNo ratings yet
- Auspar Valdoxan PDFDocument87 pagesAuspar Valdoxan PDFPandroshaNo ratings yet
- Interactive and Comprehensive Database For Environmental Effect Data For PharmaceuticalsDocument5 pagesInteractive and Comprehensive Database For Environmental Effect Data For PharmaceuticalsRaluca RatiuNo ratings yet
- Site Master File (SMF) For Pharmaceuticals - Pharmaceutical GuidelinesDocument2 pagesSite Master File (SMF) For Pharmaceuticals - Pharmaceutical GuidelinesPalak Agarwal0% (1)
- Pqri Draft Guidance On Blend Uniformity and Content UniformityyDocument13 pagesPqri Draft Guidance On Blend Uniformity and Content UniformityyPhill BrettNo ratings yet
- Evaluation of The Physicochemical Properties and Stability of SLNDocument276 pagesEvaluation of The Physicochemical Properties and Stability of SLNvkguptajssNo ratings yet
- FDC ListDocument43 pagesFDC ListHari Ram100% (2)
- Importance of Senaka Bibile Drug Policy at The Economic Turmoil of Sri LankaDocument10 pagesImportance of Senaka Bibile Drug Policy at The Economic Turmoil of Sri Lankaajith kumaraNo ratings yet
- Korea GMO and DMFDocument33 pagesKorea GMO and DMFAlok Kumar sharmaNo ratings yet