You might also like
- IntegumentaryDocument8 pagesIntegumentaryRamon Carlo AlmiranezNo ratings yet
- Increased Intracranial Pressure (IICP)Document2 pagesIncreased Intracranial Pressure (IICP)Giselle Chloe Baluya icoNo ratings yet
- Muscle Strength TestingDocument3 pagesMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- Women's Running - February 2016Document84 pagesWomen's Running - February 2016Agache GigelNo ratings yet
- CV AliDocument8 pagesCV AliCryptic SufiNo ratings yet
- Pentagon CDDocument12 pagesPentagon CDJohnNo ratings yet
- Ncm107 Summarization of MCNDocument40 pagesNcm107 Summarization of MCNArlyn Faith AlvarezNo ratings yet
- Pediatric NursingDocument29 pagesPediatric NursingjeshemaNo ratings yet
- Children's Respiratory NursingFrom EverandChildren's Respiratory NursingJanice MightenNo ratings yet
- Nutrition 1Document6 pagesNutrition 1jeshemaNo ratings yet
- Common Board Question 2Document965 pagesCommon Board Question 2Angelie PantajoNo ratings yet
- Take One Nursing FC Psych 1 4Document7 pagesTake One Nursing FC Psych 1 4LiezelNo ratings yet
- Assessment of The Hematologic SystemDocument36 pagesAssessment of The Hematologic SystemUSC Upstate Nursing CoachesNo ratings yet
- A2.Fundamentals - 25item With Rationale (PNLE) IIDocument3 pagesA2.Fundamentals - 25item With Rationale (PNLE) IIBlardy Falking You Benchod BlardyNo ratings yet
- Set 3Document22 pagesSet 3Alyssa MontimorNo ratings yet
- 2 Introduction To Nursing Theory HandoutDocument4 pages2 Introduction To Nursing Theory HandoutPlacido Edgar MagaNo ratings yet
- Patrick Callaghan, Helen Waldock-Emergencies in Mental Health Nursing-Oxford University Press (2013)Document195 pagesPatrick Callaghan, Helen Waldock-Emergencies in Mental Health Nursing-Oxford University Press (2013)VidákZsigmond100% (2)
- December2012nletips Funda 121005040112 Phpapp02 PDFDocument6 pagesDecember2012nletips Funda 121005040112 Phpapp02 PDFJessamine Rochelle Reyes EsbertoNo ratings yet
- T 2 - Unit Test 2 - Psych & PediaDocument8 pagesT 2 - Unit Test 2 - Psych & PediaenzoNo ratings yet
- Nle Test Plan: Nursing Practice IDocument14 pagesNle Test Plan: Nursing Practice IericNo ratings yet
- Carillo vs. PeopleDocument1 pageCarillo vs. People123abc456defNo ratings yet
- NURSING PRACTICE IV - Care of Clients With Physiologic and Psychosocial Alterations (Part B)Document25 pagesNURSING PRACTICE IV - Care of Clients With Physiologic and Psychosocial Alterations (Part B)Rem Yriz100% (1)
- Physiological and Psychosocial Alterations: Nursing Practice 3A: Nursing Care of Client WithDocument9 pagesPhysiological and Psychosocial Alterations: Nursing Practice 3A: Nursing Care of Client WithSepjho M. Nojepse0% (1)
- Fundamentals of NursingDocument13 pagesFundamentals of NursingGiselle Chloe Baluya icoNo ratings yet
- Giger and DavidhizarDocument4 pagesGiger and DavidhizarHv EstokNo ratings yet
- PA and ResearchDocument36 pagesPA and ResearchjeshemaNo ratings yet
- No. of Workers Required Occupational Health Service Provider 101 201 301Document9 pagesNo. of Workers Required Occupational Health Service Provider 101 201 301JoshuaNo ratings yet
- Surgical DrainsDocument3 pagesSurgical DrainsJerome ValdellonNo ratings yet
- Margo Mccaffery, A Nurse and A Pioneer in Pain ManagementDocument7 pagesMargo Mccaffery, A Nurse and A Pioneer in Pain ManagementGiselle Chloe Baluya ico100% (1)
- NR1 Lecture Notes 1, IntroductionDocument11 pagesNR1 Lecture Notes 1, IntroductionHassen ZabalaNo ratings yet
- PSYCHE (Songs)Document4 pagesPSYCHE (Songs)Jo Hn VengzNo ratings yet
- NP1 BulletsDocument17 pagesNP1 BulletsJea VesagasNo ratings yet
- Fundamentals of NursingDocument332 pagesFundamentals of NursingQuia Benjch UayanNo ratings yet
- Final Examinations Leadership and Management Name: - QUIJANO - Year/ Level: - Date/ TimeDocument4 pagesFinal Examinations Leadership and Management Name: - QUIJANO - Year/ Level: - Date/ TimeARISNo ratings yet
- Expanded Program On ImmunizationDocument15 pagesExpanded Program On ImmunizationReygie MarsadaNo ratings yet
- PALMRDocument9 pagesPALMRCai SolanoNo ratings yet
- Hema Q&aDocument126 pagesHema Q&aHoney Lyn AlebioNo ratings yet
- JomsDocument168 pagesJomsElaiza DumlaoNo ratings yet
- Bioethics in Nursing Practice Practice TestDocument9 pagesBioethics in Nursing Practice Practice TestjeshemaNo ratings yet
- By: Catherine M. Souribio, R.NDocument40 pagesBy: Catherine M. Souribio, R.NIsrael AgrisNo ratings yet
- Funda DXDocument8 pagesFunda DXdhodejun lizhaldeNo ratings yet
- Foundation of PROFESSIONAL Nursing Practice: Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDocument19 pagesFoundation of PROFESSIONAL Nursing Practice: Practice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralNo ratings yet
- TFN Quiz IntroDocument1 pageTFN Quiz IntroKaye CorNo ratings yet
- GFSDGSDGFSDGDocument2 pagesGFSDGSDGFSDGMA IZNo ratings yet
- Ears Lecture GuideDocument56 pagesEars Lecture GuidemajNo ratings yet
- Final ReviewDocument9 pagesFinal ReviewAlbert jonesNo ratings yet
- Wound Care: Section I: Assessing Your UnderstandingDocument12 pagesWound Care: Section I: Assessing Your UnderstandingkeyonaNo ratings yet
- Therapeutic CommunicationDocument7 pagesTherapeutic CommunicationRemedios BandongNo ratings yet
- The Nclex-Rn Test Plan Adult Physiologal IntegrityDocument25 pagesThe Nclex-Rn Test Plan Adult Physiologal IntegrityalfreddahbiNo ratings yet
- Med Surg Lessons # 1 QuestionsDocument4 pagesMed Surg Lessons # 1 Questionsccapps25No ratings yet
- Examination Male Genitalia855090520Document4 pagesExamination Male Genitalia855090520HardiTariqHammaNo ratings yet
- Metabolism: Marcus Cueno, RNDocument15 pagesMetabolism: Marcus Cueno, RNMarcus, RN100% (2)
- Group QuestionsDocument7 pagesGroup QuestionsSheana TmplNo ratings yet
- Ob Review QuestionsDocument31 pagesOb Review QuestionsRandyNo ratings yet
- Cardiovascular Physical Examination - LectureDocument20 pagesCardiovascular Physical Examination - LectureDENNIS N. MUÑOZNo ratings yet
- Medical Surgical Nursing Review 1Document31 pagesMedical Surgical Nursing Review 1jeshemaNo ratings yet
- R.A. No. 11509 Doktor para Sa Bayan ActDocument14 pagesR.A. No. 11509 Doktor para Sa Bayan ActAngel BacaniNo ratings yet
- Funda 15Document3 pagesFunda 15Nur SetsuNo ratings yet
- Fundamentals of NursingDocument31 pagesFundamentals of NursingCherrie Dianne SeriñaNo ratings yet
- Chapter 19Document16 pagesChapter 19missy23pap100% (1)
- Doctrine of Double Effect Stanford Encyclopedia of PhilosophyDocument9 pagesDoctrine of Double Effect Stanford Encyclopedia of PhilosophyCarlos TrNo ratings yet
- Name: Glenda S, Casundo Date: Nov. 3, 2020 Course/Yr: BSN Iv Comp - Appraisal Quiz No.2Document4 pagesName: Glenda S, Casundo Date: Nov. 3, 2020 Course/Yr: BSN Iv Comp - Appraisal Quiz No.2Joanne Bernadette AguilarNo ratings yet
- Kozier Chapter 17 Health Wellness Well BeingDocument10 pagesKozier Chapter 17 Health Wellness Well BeingpauchanmnlNo ratings yet
- Sas 2 Cabahug, Victoria Mae IDocument4 pagesSas 2 Cabahug, Victoria Mae Ibekbekk cabahugNo ratings yet
- Lecture 4 - Intraoperative & Postoperative Nursing Management 2021-2022Document46 pagesLecture 4 - Intraoperative & Postoperative Nursing Management 2021-2022عمار عاشورNo ratings yet
- Peran - Fungsi Perawat Safe SurgeryDocument69 pagesPeran - Fungsi Perawat Safe Surgeryerwin salehNo ratings yet
- Intraoperative PhaseDocument173 pagesIntraoperative PhaseEbi100% (1)
- MedsurDocument116 pagesMedsurMacy MarquezNo ratings yet
- Heart Failure2Document39 pagesHeart Failure2Giselle Chloe Baluya icoNo ratings yet
- NUR-086-Act-2 4Document2 pagesNUR-086-Act-2 4Giselle Chloe Baluya icoNo ratings yet
- 37420046-Ncp-Head-Injury 2Document3 pages37420046-Ncp-Head-Injury 2Giselle Chloe Baluya icoNo ratings yet
- Homeostasis, Stress and Adaptation: Types of Stressors: Physiologic Emotional/PsychologicDocument5 pagesHomeostasis, Stress and Adaptation: Types of Stressors: Physiologic Emotional/PsychologicGiselle Chloe Baluya ico100% (1)
- Nursing Classifications and LanguagesDocument12 pagesNursing Classifications and LanguagesGiselle Chloe Baluya ico0% (1)
- Case 4 - Short of Breath With Expiratory and Inspiratory Wheezing Updated 2 Nov 2015 - StudentDocument7 pagesCase 4 - Short of Breath With Expiratory and Inspiratory Wheezing Updated 2 Nov 2015 - StudentSami Obaid Fallaj Alanazi 0261No ratings yet
- Disease Deep Dive Kathryn CrimDocument7 pagesDisease Deep Dive Kathryn Crimapi-579320483No ratings yet
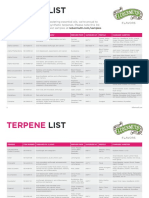
- Lebermuth Terpenes List 2019Document4 pagesLebermuth Terpenes List 2019EdoardoNo ratings yet
- Vinmec Services Marketing ReportDocument32 pagesVinmec Services Marketing ReportNgô Hồng Giang 2M-20ACN100% (1)
- The Use of Hyaluronidase in Cosmetic DermatologyDocument7 pagesThe Use of Hyaluronidase in Cosmetic DermatologyDr. Hilder HernandezNo ratings yet
- Medical Sociology 13th Edition Cockerham Test BankDocument10 pagesMedical Sociology 13th Edition Cockerham Test BankMarlys Culver100% (37)
- Arrhythmias: Domina Petric, MDDocument22 pagesArrhythmias: Domina Petric, MDMwaba PeterNo ratings yet
- DismenoreDocument14 pagesDismenoreRudyanto_NGPNo ratings yet
- Peh 4 Module 3Document134 pagesPeh 4 Module 3burner accNo ratings yet
- MD Development PaediatrcsDocument102 pagesMD Development PaediatrcsMuhammad Farooq SaeedNo ratings yet
- Ajeph Id45Document6 pagesAjeph Id45noneofyabiznasNo ratings yet
- CSIR Life Sciences Paper 2 Model QuestionsDocument12 pagesCSIR Life Sciences Paper 2 Model QuestionsImmanuel VinothNo ratings yet
- Dr. Abdelhakam Aldigeal Enterobacter CitrobacterDocument22 pagesDr. Abdelhakam Aldigeal Enterobacter CitrobacterAbdelhakam AliNo ratings yet
- Philippine Pediatric Society, IncDocument41 pagesPhilippine Pediatric Society, IncMark Cristopher JoaquinNo ratings yet
- 29 IM Raw Beef Prod SamplingDocument71 pages29 IM Raw Beef Prod SamplingNader Sedighi100% (1)
- E-Book Seminar PAPDI Kota Bekasi skp8Document5 pagesE-Book Seminar PAPDI Kota Bekasi skp8Miftah Nur AndamsariNo ratings yet
- Structure of Chemical Componds ImpuritiesDocument6 pagesStructure of Chemical Componds ImpuritiesJorge Oswaldo Toro Jaimes100% (1)
- Kaur 2018Document5 pagesKaur 2018Bima RizkiNo ratings yet
- Danger of LonelinessDocument12 pagesDanger of LonelinessLonzell WinnNo ratings yet
- Fissural CystsDocument17 pagesFissural CystssailalithaNo ratings yet
- 3D Objects - Shortcut - LNKDocument2 pages3D Objects - Shortcut - LNKromyNo ratings yet
- م اراد Darul Uloom Austin (DUA) : Student/Parent HandbookDocument12 pagesم اراد Darul Uloom Austin (DUA) : Student/Parent HandbookDrFaryal AbbassiNo ratings yet
- Breastfeeding With Thrush: Signs and Symptoms For The MotherDocument2 pagesBreastfeeding With Thrush: Signs and Symptoms For The MotherFaraz HussainNo ratings yet
- Form 1.1 Sample Data Gathering Instrument For TraineeDocument3 pagesForm 1.1 Sample Data Gathering Instrument For TraineeDanilo CumpioNo ratings yet
- Dermatology Chap6. Bacterial Infections of Skin 2020-3-23Document368 pagesDermatology Chap6. Bacterial Infections of Skin 2020-3-23Mohsin Tanmoy100% (1)