You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- HSE Bridging Document Template 2019Document50 pagesHSE Bridging Document Template 2019raj100% (4)
- RA Risk Window Cleaning by Using Rope AccessDocument11 pagesRA Risk Window Cleaning by Using Rope AccessADIL FAZALNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fadel Thariq Gifari - Assignment 1Document12 pagesFadel Thariq Gifari - Assignment 1Fadel GifariNo ratings yet
- Craniotomy Nursing Care PlanDocument5 pagesCraniotomy Nursing Care PlanJordz Placi100% (2)
- Communicable Disease Nursing Ca1 July 2018 5 PDFDocument461 pagesCommunicable Disease Nursing Ca1 July 2018 5 PDFJordz Placi100% (2)
- NCP Dengue Fever Hyperthermia and Acute PainDocument4 pagesNCP Dengue Fever Hyperthermia and Acute PainJordz PlaciNo ratings yet
- Risk Register - Movie NightDocument2 pagesRisk Register - Movie Nightapi-514548596No ratings yet
- Nursing Degree - EZEKULIE MALLAREDocument1 pageNursing Degree - EZEKULIE MALLAREJordz PlaciNo ratings yet
- NURSING and SURGICAL MANAGEMENTDocument3 pagesNURSING and SURGICAL MANAGEMENTJordz PlaciNo ratings yet
- LABS Part 2 Jagna SchistosomiasisDocument3 pagesLABS Part 2 Jagna SchistosomiasisJordz PlaciNo ratings yet
- Nures ApaDocument1 pageNures ApaJordz PlaciNo ratings yet
- Retinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentDocument3 pagesRetinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentJordz Placi100% (1)
- Anatomy and Physiology: Circulatory SystemDocument4 pagesAnatomy and Physiology: Circulatory SystemJordz PlaciNo ratings yet
- MS2 PPT Course Unit 13 - Review of The Anatomy and Physiology of The Eyes & AssessmentDocument5 pagesMS2 PPT Course Unit 13 - Review of The Anatomy and Physiology of The Eyes & AssessmentJordz PlaciNo ratings yet
- LABS Part 2Document3 pagesLABS Part 2Jordz PlaciNo ratings yet
- Muskulo Geria-1Document40 pagesMuskulo Geria-1Jordz PlaciNo ratings yet
- Gi NelecDocument52 pagesGi NelecJordz PlaciNo ratings yet
- Gi NelecDocument52 pagesGi NelecJordz PlaciNo ratings yet
- Health and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoDocument35 pagesHealth and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoJordz PlaciNo ratings yet
- Fdar TorioDocument3 pagesFdar TorioJordz PlaciNo ratings yet
- Communicable Disease Nursing Ca1 July 2018 5Document461 pagesCommunicable Disease Nursing Ca1 July 2018 5Jordz PlaciNo ratings yet
- NCM104 MS2 - Course Unit 13 - Review of The Anatomy and Physiology of The Eyes & AssessmentDocument5 pagesNCM104 MS2 - Course Unit 13 - Review of The Anatomy and Physiology of The Eyes & AssessmentJordz PlaciNo ratings yet
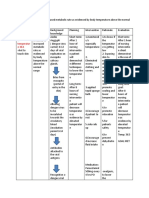
- Assessment Explanation of The Problem Goals and Objectives Interventions Rationale EvaluationDocument9 pagesAssessment Explanation of The Problem Goals and Objectives Interventions Rationale EvaluationJordz PlaciNo ratings yet
- Ody Temperature As Evidenced by Temperature of 38.5Document1 pageOdy Temperature As Evidenced by Temperature of 38.5Jordz PlaciNo ratings yet
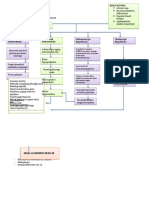
- There Are 3 Layers of Tissue Called MeningesDocument2 pagesThere Are 3 Layers of Tissue Called MeningesJordz PlaciNo ratings yet
- Short Term Goal: After 1 Hour of Short Term Goal: After 1Document2 pagesShort Term Goal: After 1 Hour of Short Term Goal: After 1Jordz PlaciNo ratings yet
- Drug Mechanis MOF Action Indicatio N and Rationale Contra Indication S Side Effects Nursing ConsiderationDocument1 pageDrug Mechanis MOF Action Indicatio N and Rationale Contra Indication S Side Effects Nursing ConsiderationJordz PlaciNo ratings yet
- Risk Factors:: Pathophysiology of Alzheimer'S DiseaseDocument2 pagesRisk Factors:: Pathophysiology of Alzheimer'S DiseaseJordz PlaciNo ratings yet
- Case: Pulmonary Tuberculosis Group D: NCM 104 Rle-Cd BSN 3Y2-1 SUBMITTED TO: Gerardo Nicolas, RN, MANDocument18 pagesCase: Pulmonary Tuberculosis Group D: NCM 104 Rle-Cd BSN 3Y2-1 SUBMITTED TO: Gerardo Nicolas, RN, MANJordz PlaciNo ratings yet
- Online Immigrant Visa and Alien Registration Application (DS-260)Document11 pagesOnline Immigrant Visa and Alien Registration Application (DS-260)Jordz PlaciNo ratings yet
- Eating Disoder PPT 3Document22 pagesEating Disoder PPT 3Jordz PlaciNo ratings yet
- Hsep-06 - Emergency Preparedness & ResponseDocument8 pagesHsep-06 - Emergency Preparedness & ResponseScha Affin100% (1)
- Disaster Readiness and Risk Reduction: Quarter 2 - Module 6Document24 pagesDisaster Readiness and Risk Reduction: Quarter 2 - Module 6garryNo ratings yet
- 53.1 - OSH Construction Management Plan v3.0 English-3Document30 pages53.1 - OSH Construction Management Plan v3.0 English-3Anthikkatte Reddots50% (4)
- Book13 - Roller Screen RR1439 - P0EBD72 (TR 1-59)Document59 pagesBook13 - Roller Screen RR1439 - P0EBD72 (TR 1-59)Cuộc Sống MàNo ratings yet
- SITXHRM007Document69 pagesSITXHRM007zhangandynewNo ratings yet
- Practice Teaching On "Disaster Nursing"Document10 pagesPractice Teaching On "Disaster Nursing"Rumela Ganguly ChakrabortyNo ratings yet
- Emergency Plan and Procedure in Industry Involving Norm/TenormDocument34 pagesEmergency Plan and Procedure in Industry Involving Norm/TenormMohd Isa HarunNo ratings yet
- Plan Operacional Ante DesastresDocument244 pagesPlan Operacional Ante DesastresXuaem Tirado RamosNo ratings yet
- Case Study 2 - ADocument7 pagesCase Study 2 - AIdaSafina AzizNo ratings yet
- Disaster Preparedness and Rehabilitation: Dr. K. Suresh KumarDocument45 pagesDisaster Preparedness and Rehabilitation: Dr. K. Suresh KumarAbdisa GonfaNo ratings yet
- Lone Working Risk AssessmentDocument3 pagesLone Working Risk AssessmentMuhammed yahiyaNo ratings yet
- Acer Transition Pres FinalDocument12 pagesAcer Transition Pres FinalDabe LoredlebNo ratings yet
- Awis Ti Langenlangen: An Understanding of The Awareness of Isnhs' Stem Students On Responses To EmergencyDocument12 pagesAwis Ti Langenlangen: An Understanding of The Awareness of Isnhs' Stem Students On Responses To EmergencyKristine AsuncionNo ratings yet
- Executive Order 41 Frequently Asked Questions v2020 2Document4 pagesExecutive Order 41 Frequently Asked Questions v2020 2Virginia Department of Emergency ManagementNo ratings yet
- Bill179 1 PDFDocument11 pagesBill179 1 PDFInes De CastroNo ratings yet
- Ekf Coaching Guide PDFDocument22 pagesEkf Coaching Guide PDFElaine PaulineNo ratings yet
- Disaster Management Project - 2016009Document15 pagesDisaster Management Project - 2016009Akshay LalNo ratings yet
- Steve F. Carlisle,: Professional SummaryDocument5 pagesSteve F. Carlisle,: Professional SummaryRickey StokesNo ratings yet
- Private NCS4 Report On Evolv ExpressDocument52 pagesPrivate NCS4 Report On Evolv ExpressLindsey BasyeNo ratings yet
- Planning and Responding To Workplace EmergenciesDocument3 pagesPlanning and Responding To Workplace EmergenciesIsabel del ValleNo ratings yet
- IFI Safety Statement August 2017Document527 pagesIFI Safety Statement August 2017BryanNo ratings yet
- START - Simple Triage and Rapid Treatment: MinorDocument7 pagesSTART - Simple Triage and Rapid Treatment: Minorlp2tk tenaga kesehatanNo ratings yet
- Inspection Test Plan, Inspection Checklist, Work Safety Procedure REFERENCEDocument174 pagesInspection Test Plan, Inspection Checklist, Work Safety Procedure REFERENCEJeff JiaNo ratings yet
- Introduction To Ingen: The StructureDocument4 pagesIntroduction To Ingen: The StructureMergus MerganserNo ratings yet
- Bureau of Fire Standards Guidance For Regulatory Compliance: NoticeDocument23 pagesBureau of Fire Standards Guidance For Regulatory Compliance: NoticeBenaoumeur FertasNo ratings yet
- Design of Door HandlesDocument7 pagesDesign of Door HandlesFelice ShareenNo ratings yet