You might also like
- Heal Yourself NaturallyDocument204 pagesHeal Yourself NaturallyKanjaFit100% (8)
- Drugs Acting On Respiratory SystemDocument52 pagesDrugs Acting On Respiratory SystemIrwan M. Iskober100% (4)
- Respiratory Agents: Dextromethorphan, Diphenhydramine, Guaifenesin, Albuterol, and BudesonideDocument30 pagesRespiratory Agents: Dextromethorphan, Diphenhydramine, Guaifenesin, Albuterol, and BudesonideLindy JaneNo ratings yet
- RH IncompatibilityDocument33 pagesRH IncompatibilityChristine Denise Venus Valentino0% (1)
- Virology MCQsDocument7 pagesVirology MCQsHabib Ullah100% (1)
- Paramedic Soft Tissue InjuryDocument60 pagesParamedic Soft Tissue InjuryPaulhotvw67100% (5)
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (2)
- Montelukast Levoceterizine (ZYKAST)Document2 pagesMontelukast Levoceterizine (ZYKAST)Kristine Young100% (2)
- Sel&Ass&Pae&Lis&Car&1 STDocument198 pagesSel&Ass&Pae&Lis&Car&1 STali tida100% (1)
- NeurotransmittersDocument5 pagesNeurotransmittersJoezerk Jhon Biel100% (1)
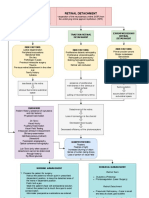
- Retinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentDocument3 pagesRetinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentJordz Placi100% (1)
- Fdar TorioDocument3 pagesFdar TorioJordz PlaciNo ratings yet
- Pediatric Nursing Care PlanDocument18 pagesPediatric Nursing Care PlanRo Vin100% (2)
- NCP Dengue Fever Hyperthermia and Acute PainDocument4 pagesNCP Dengue Fever Hyperthermia and Acute PainJordz PlaciNo ratings yet
- DementiaDocument40 pagesDementiakhusnulNo ratings yet
- Nursing Care Plan: Name of Patient: Attending Physician: Age: Impression/DiagnosisDocument3 pagesNursing Care Plan: Name of Patient: Attending Physician: Age: Impression/DiagnosisMelody B. Miguel0% (1)
- Craniotomy Nursing Care PlanDocument5 pagesCraniotomy Nursing Care PlanJordz Placi100% (2)
- PNLEDocument34 pagesPNLEnjNo ratings yet
- AcetylcysteineDocument2 pagesAcetylcysteineGwyn RosalesNo ratings yet
- Communicable Disease Nursing Ca1 July 2018 5Document461 pagesCommunicable Disease Nursing Ca1 July 2018 5Jordz PlaciNo ratings yet
- Case Study Opd UfcDocument13 pagesCase Study Opd UfcShan DyNo ratings yet
- Ineffective Breathing Pattern Related To Bronchospasm, Decreased Lung ExpansionDocument2 pagesIneffective Breathing Pattern Related To Bronchospasm, Decreased Lung ExpansionReylan Garcia43% (7)
- Copd Drug StudyDocument9 pagesCopd Drug StudyJoegie Ario100% (1)
- The Nurse's Guide to Communicable DiseasesDocument461 pagesThe Nurse's Guide to Communicable DiseasesJordz Placi100% (1)
- Ipratropium Salbutamol (DUAVENT)Document2 pagesIpratropium Salbutamol (DUAVENT)Kristine Young100% (2)
- Sas 17Document3 pagesSas 17Sistine Rose LabajoNo ratings yet
- Stroke: Dr. Fidha Rahmayani, M.SC, SP.S Fakultas Kedokteran Universitas Lampung RS Abdul MulukDocument45 pagesStroke: Dr. Fidha Rahmayani, M.SC, SP.S Fakultas Kedokteran Universitas Lampung RS Abdul Mulukdhea nadhiaNo ratings yet
- Ipratropium Bromide Plus SalbutamolDocument3 pagesIpratropium Bromide Plus SalbutamolA sison100% (1)
- Meconium Aspiration Syndrome Case PresentationDocument26 pagesMeconium Aspiration Syndrome Case Presentationkis100% (2)
- Acute Bronchitis Alcantara Manuscript 2Document10 pagesAcute Bronchitis Alcantara Manuscript 2Ma. Isabel A. EnriquezNo ratings yet
- Restoring Fluid Balance Through RehydrationDocument11 pagesRestoring Fluid Balance Through RehydrationMicah MagallanoNo ratings yet
- Silbert, Sara May L. (BSN 2-H) DRUG STUDYDocument4 pagesSilbert, Sara May L. (BSN 2-H) DRUG STUDYSara May SilbertNo ratings yet
- Drug StudyDocument5 pagesDrug Studyboxed juiceNo ratings yet
- The Appropriate Amount of Oxygen Is Continuously Delivered So That The Patient Does Not DesiderateDocument4 pagesThe Appropriate Amount of Oxygen Is Continuously Delivered So That The Patient Does Not DesideratezheeraNo ratings yet
- Drug NameDocument5 pagesDrug NameSushiBaLNo ratings yet
- SalbutamolDocument1 pageSalbutamolRheza AltimoNo ratings yet
- Drug StudyDocument2 pagesDrug StudyMec AmilasanNo ratings yet
- Drug classification, mechanism of action, indications and nursing responsibilitiesDocument5 pagesDrug classification, mechanism of action, indications and nursing responsibilitiesMcNover Catlin OsamNo ratings yet
- BPN - FinalDocument14 pagesBPN - FinalAngel Alexa Del MundoNo ratings yet
- Pharmacology PDFDocument20 pagesPharmacology PDFMichelle SatairapanNo ratings yet
- Drug Action and Nursing ResponsibilitiesDocument38 pagesDrug Action and Nursing ResponsibilitiesSnehal SharmaNo ratings yet
- Lhea's Case StudyDocument14 pagesLhea's Case StudyMelody B. MiguelNo ratings yet
- ASTHMADocument22 pagesASTHMAKyle VargasNo ratings yet
- Drug Study #3Document8 pagesDrug Study #3James Emman ClementeNo ratings yet
- Drug Study 2Document2 pagesDrug Study 2Joshua Selwyn SalazarNo ratings yet
- Silbert, Sara May L. (BSN 2-h) Drug StudyDocument4 pagesSilbert, Sara May L. (BSN 2-h) Drug StudySara May SilbertNo ratings yet
- Ledesma - DRUG STUDYDocument8 pagesLedesma - DRUG STUDYAnnika Ysabelle S. LedesmaNo ratings yet
- Opd) Ba) CSDocument7 pagesOpd) Ba) CSFerreze AnnNo ratings yet
- Drug StudyDocument5 pagesDrug Studymarie100% (27)
- Dipolog Medical Center College Foundation Inc.: A Case Study OF AppendicitisDocument11 pagesDipolog Medical Center College Foundation Inc.: A Case Study OF AppendicitisTiffany AdriasNo ratings yet
- Dacanay Jungco Omeprazole DsDocument2 pagesDacanay Jungco Omeprazole DsTRISHA JUNGCONo ratings yet
- Gr.4 NCP Health AssessmentDocument3 pagesGr.4 NCP Health AssessmentAlessandro MadrigalNo ratings yet
- Drug Study UtiDocument4 pagesDrug Study UtiClaire MachicaNo ratings yet
- Drug StudyDocument2 pagesDrug StudyZek Comidoy100% (1)
- Republic of the Philippines College of Nursing Drug StudyDocument5 pagesRepublic of the Philippines College of Nursing Drug StudyChelsea WuNo ratings yet
- PNEUMONIADocument14 pagesPNEUMONIArogggNo ratings yet
- Pharma Reviewer (Midterm)Document7 pagesPharma Reviewer (Midterm)SaidinaNo ratings yet
- 2nd Drug Study and NCPDocument8 pages2nd Drug Study and NCPDara Sophia EncarguezNo ratings yet
- Drug study on bronchodilators and corticosteroidsDocument17 pagesDrug study on bronchodilators and corticosteroidsJhucyl Mae GalvezNo ratings yet
- Cues Nursing Diagnosis Inference Planning Nursing Intervention Rationale EvaluationDocument3 pagesCues Nursing Diagnosis Inference Planning Nursing Intervention Rationale EvaluationNichol John MalabananNo ratings yet
- Case Study 4Document22 pagesCase Study 4Angel MayNo ratings yet
- Drug-Tabulation (2) For CHN IndiDocument5 pagesDrug-Tabulation (2) For CHN IndiKANT JAMES D. MAHANNo ratings yet
- Drug Study Lab, NCP - Bronchial AsthmaDocument6 pagesDrug Study Lab, NCP - Bronchial AsthmaRichelle Sandriel C. de CastroNo ratings yet
- Paracetamol Nursing CareDocument5 pagesParacetamol Nursing CareAlyssa Moutrie Dulay ArabeNo ratings yet
- Asma 2019Document64 pagesAsma 2019ajeng putriNo ratings yet
- Generic Name: Brand Name: Zurenix Classification: Doctor's Order: 750 Date Started: Nursing ConsiderationsDocument3 pagesGeneric Name: Brand Name: Zurenix Classification: Doctor's Order: 750 Date Started: Nursing ConsiderationsAlvin RamirezNo ratings yet
- Drug TabulationDocument6 pagesDrug TabulationKANT JAMES D. MAHANNo ratings yet
- Drug Study: 75 Yrs. OldDocument3 pagesDrug Study: 75 Yrs. OldAngie MandeoyaNo ratings yet
- Acute MI DMII Medical ManagementDocument52 pagesAcute MI DMII Medical ManagementsherwincruzNo ratings yet
- KlindexDocument2 pagesKlindexPatricia MaglasangNo ratings yet
- Anaphylactic Shock Guide for NursesDocument3 pagesAnaphylactic Shock Guide for NurseszipheleleNo ratings yet
- FF0089 01 Free Healthcare Presentation Template 16x9Document22 pagesFF0089 01 Free Healthcare Presentation Template 16x9Sartini Roma Dame NainggolanNo ratings yet
- Drug Study SummariesDocument6 pagesDrug Study SummariesGabriel Delos SantosNo ratings yet
- HospiceDocument10 pagesHospiceJasmineNo ratings yet
- Nursing Student Stress & ResilienceDocument1 pageNursing Student Stress & ResilienceJordz PlaciNo ratings yet
- Use of Electroconvulsive Therapy To Patient With Schizophrenia and Other Mental IllnessDocument1 pageUse of Electroconvulsive Therapy To Patient With Schizophrenia and Other Mental IllnessJordz PlaciNo ratings yet
- Nursing Student Stress & ResilienceDocument1 pageNursing Student Stress & ResilienceJordz PlaciNo ratings yet
- Nures ApaDocument1 pageNures ApaJordz PlaciNo ratings yet
- Nursing Student Stress & ResilienceDocument1 pageNursing Student Stress & ResilienceJordz PlaciNo ratings yet
- LABS Part 2 Jagna SchistosomiasisDocument3 pagesLABS Part 2 Jagna SchistosomiasisJordz PlaciNo ratings yet
- Nursing Care for Ear Pain ReliefDocument3 pagesNursing Care for Ear Pain ReliefJordz PlaciNo ratings yet
- Otitis Media DialogueDocument1 pageOtitis Media DialogueJordz PlaciNo ratings yet
- WEEK 14 Ear Ana Dxtic TestsDocument35 pagesWEEK 14 Ear Ana Dxtic TestsJordz PlaciNo ratings yet
- Otitis Media DialogueDocument1 pageOtitis Media DialogueJordz PlaciNo ratings yet
- RECOMMENDATIONS Dengue FeverDocument1 pageRECOMMENDATIONS Dengue FeverJordz PlaciNo ratings yet
- Recomm Schisto MajanDocument3 pagesRecomm Schisto MajanJordz PlaciNo ratings yet
- Nursing Student Stress & ResilienceDocument1 pageNursing Student Stress & ResilienceJordz PlaciNo ratings yet
- LABS Part 2Document3 pagesLABS Part 2Jordz PlaciNo ratings yet
- Muskulo Geria-1Document40 pagesMuskulo Geria-1Jordz PlaciNo ratings yet
- Gi NelecDocument52 pagesGi NelecJordz PlaciNo ratings yet
- Anatomy and Physiology: Circulatory SystemDocument4 pagesAnatomy and Physiology: Circulatory SystemJordz PlaciNo ratings yet
- Health and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoDocument35 pagesHealth and Safety Protocols: Dr. Michael Bautista Dr. Ethyl Salvador-CayetanoJordz PlaciNo ratings yet
- Gi NelecDocument52 pagesGi NelecJordz PlaciNo ratings yet
- Muskulo Geria-1Document40 pagesMuskulo Geria-1Jordz PlaciNo ratings yet
- Monitoring blood glucose levels and kidney functionDocument9 pagesMonitoring blood glucose levels and kidney functionJordz PlaciNo ratings yet
- Ncenl07 Activity 1Document1 pageNcenl07 Activity 1Jordz PlaciNo ratings yet
- (884 KB) Eyeball Anatomy Sagittal View - EBM Consult HandoutDocument3 pages(884 KB) Eyeball Anatomy Sagittal View - EBM Consult HandoutJordz PlaciNo ratings yet
- Chapter 21 - Aids2Document31 pagesChapter 21 - Aids2Sanjeevan Aravindan (JEEV)No ratings yet
- GpatDocument21 pagesGpatDeepak Kumar100% (1)
- Chronic Kidney DiseaseDocument18 pagesChronic Kidney DiseaseAde Cahyo IslamiNo ratings yet
- ph7x6t376 - Week 35 - Health 7 Approved APG 1Document11 pagesph7x6t376 - Week 35 - Health 7 Approved APG 1G- 6 ODL Trisha Mae ClementeNo ratings yet
- Skin PigmentatDocument110 pagesSkin Pigmentatsteven saputra0% (1)
- COPD NotesDocument4 pagesCOPD NotesjisooNo ratings yet
- Gram Pozitive CocciDocument47 pagesGram Pozitive CocciJedjdjdjdjdhjdNo ratings yet
- Case HT 5Document4 pagesCase HT 5farhah ayunizar ramadhaniNo ratings yet
- Serrapeptase EBook 3rd Edition-1Document362 pagesSerrapeptase EBook 3rd Edition-1shaknote5No ratings yet
- Spondylosis: Vertebral ColumnDocument12 pagesSpondylosis: Vertebral ColumnVdct MglNo ratings yet
- Virology Compilation For Final Exam GuideDocument51 pagesVirology Compilation For Final Exam GuideJenny Rose PangdaoNo ratings yet
- TriziaLoreto DocsDocument20 pagesTriziaLoreto DocsNenia Balictar100% (1)
- Gingival Tissue Management Methods for Dental RestorationsDocument20 pagesGingival Tissue Management Methods for Dental RestorationsSriram PugalenthiNo ratings yet
- Cell Comparison ChartDocument3 pagesCell Comparison ChartJake BryantNo ratings yet
- Molly's Case StudyDocument10 pagesMolly's Case StudyYounas BhattiNo ratings yet
- Contusion Pulmonum: Clinical Features and ManagementDocument10 pagesContusion Pulmonum: Clinical Features and ManagementSyamsuriWahyuNo ratings yet
- FMGE Paeds Sprint by Dr. Sarath Balaji (PW Med Ed)Document106 pagesFMGE Paeds Sprint by Dr. Sarath Balaji (PW Med Ed)Stella ParkerNo ratings yet
- ENT EEE by Dr. Manisha Budhiraja 5th Edition - UnlockedDocument448 pagesENT EEE by Dr. Manisha Budhiraja 5th Edition - UnlockedArbin PanjaNo ratings yet
- Nursing Exam Questions 2023 Part 3Document6 pagesNursing Exam Questions 2023 Part 3Lejo SunnyNo ratings yet
- Hypervitaminosis D Review: Causes, Symptoms and TreatmentDocument2 pagesHypervitaminosis D Review: Causes, Symptoms and Treatmentsmartjohnsmith10No ratings yet
- Sample Pages of MBBS Decode (MGR University)Document20 pagesSample Pages of MBBS Decode (MGR University)vkNo ratings yet