You might also like
- Combatting Pandemics Role of Global CooperationDocument5 pagesCombatting Pandemics Role of Global CooperationMikhailNo ratings yet
- Correspondence: Ebola: A Failure of International Collective ActionDocument1 pageCorrespondence: Ebola: A Failure of International Collective Actionudaysingh98No ratings yet
- Resrep24189 PDFDocument7 pagesResrep24189 PDFAINUR ROHMAH W.No ratings yet
- Resrep24189 PDFDocument7 pagesResrep24189 PDFAINUR ROHMAH W.No ratings yet
- Activity 3Document3 pagesActivity 3Tristan Jerald BechaydaNo ratings yet
- MB Confront Coronavirus Catastrophe Public Health Plan 300320 enDocument10 pagesMB Confront Coronavirus Catastrophe Public Health Plan 300320 enGeetika KhandelwalNo ratings yet
- Planning For The Next Global PandemicDocument6 pagesPlanning For The Next Global PandemicCOproduções Culturais e ArtísticasNo ratings yet
- COVID - 19 - Too Little, Too LateDocument1 pageCOVID - 19 - Too Little, Too LateIswan NggolituNo ratings yet
- WH 1988 Jul EngDocument32 pagesWH 1988 Jul EngSTANN KAZIPETNo ratings yet
- WHO - Creating A Framework Enabling - Healthcare Access For Migrants in Conflict Zones.Document9 pagesWHO - Creating A Framework Enabling - Healthcare Access For Migrants in Conflict Zones.Dhruv AgarwalNo ratings yet
- WHO BAR Topic 2Document8 pagesWHO BAR Topic 2Natasha FrancisNo ratings yet
- Final PaperDocument14 pagesFinal PaperMakky Drake BryleNo ratings yet
- Nejm 09-04-2015Document107 pagesNejm 09-04-2015Javier B GreenNo ratings yet
- Connoly Lancet Deadly 2002Document2 pagesConnoly Lancet Deadly 2002Adelina IuliaNo ratings yet
- Stephen Prior, M.D. - Preparing For A Pandemic Influenza, A Primer For Governors and Senior State OfficialsDocument32 pagesStephen Prior, M.D. - Preparing For A Pandemic Influenza, A Primer For Governors and Senior State OfficialsMiha ChiribucaNo ratings yet
- Global Health PursuitDocument5 pagesGlobal Health Pursuitujangketul62No ratings yet
- Khvi 11 11 1096457Document10 pagesKhvi 11 11 1096457The UmarNo ratings yet
- Tori Robbins Research Paper SubmissionDocument40 pagesTori Robbins Research Paper Submissionapi-529132931No ratings yet
- Global Health Security and The International Health RegulationsDocument7 pagesGlobal Health Security and The International Health RegulationssarsulthaNo ratings yet
- UGBS Working Paper Series 01-2021Document19 pagesUGBS Working Paper Series 01-2021maxiluuvNo ratings yet
- COVID-19 and Conflict: Seven Trends To Watch: Crisis Group Special Briefing N°4Document16 pagesCOVID-19 and Conflict: Seven Trends To Watch: Crisis Group Special Briefing N°4Olivier FranchiNo ratings yet
- 吕尧global times公共外交文章Document7 pages吕尧global times公共外交文章刘欣怡No ratings yet
- Decolonising Global Health in The Time of COVID 19Document13 pagesDecolonising Global Health in The Time of COVID 19Ayu RosyidaNo ratings yet
- Ckhxtyxsz0ff1o4quch43bvqb Fighting Communicable Diseases Subcommittee BriefingDocument4 pagesCkhxtyxsz0ff1o4quch43bvqb Fighting Communicable Diseases Subcommittee BriefingjakuraimanetayNo ratings yet
- Global Pandemics and Human Security - Docx Research Article 2Document14 pagesGlobal Pandemics and Human Security - Docx Research Article 2quratNo ratings yet
- Who CDS 2005.29 PDFDocument64 pagesWho CDS 2005.29 PDFrizky yuza ananDANo ratings yet
- Jamaophthalmology Sommer 2020 Ic 200013 PDFDocument2 pagesJamaophthalmology Sommer 2020 Ic 200013 PDFfaisaladeNo ratings yet
- The South African's Covid-19 Response RhetoricDocument7 pagesThe South African's Covid-19 Response RhetoricIlyka Jean SionzonNo ratings yet
- Covid-19-A Momentous ScandalDocument3 pagesCovid-19-A Momentous ScandalConstant HopeNo ratings yet
- Covid19 A Tale of Two Epidemics March 20 2020Document3 pagesCovid19 A Tale of Two Epidemics March 20 2020Tewfic SeidNo ratings yet
- Expository Essay About Corona Virus PandemicDocument6 pagesExpository Essay About Corona Virus PandemicRas JemohNo ratings yet
- Kentucky Bannister Trufanov Aff KY RR Round6Document46 pagesKentucky Bannister Trufanov Aff KY RR Round6aesopwNo ratings yet
- TB in AsiaDocument31 pagesTB in AsiaAlik Septian MubarrokNo ratings yet
- X Disease WHODocument3 pagesX Disease WHOEvangelina RivarolaNo ratings yet
- Governing Infectious Disease h5n1 Avian Influenza in Southeast AsiaDocument36 pagesGoverning Infectious Disease h5n1 Avian Influenza in Southeast AsiaFifit BimartanaNo ratings yet
- Governing Infectious Disease h5n1 Avian Influenza in Southeast AsiaDocument36 pagesGoverning Infectious Disease h5n1 Avian Influenza in Southeast AsiaFifit BimartanaNo ratings yet
- Case Study SMALLPOX ERADICATIONDocument3 pagesCase Study SMALLPOX ERADICATIONSimran WaghelaNo ratings yet
- Continuity of Supply Chain During PendamicDocument6 pagesContinuity of Supply Chain During PendamicMohsin IqbalNo ratings yet
- WHO Report On Neglected Tropical DiseasesDocument184 pagesWHO Report On Neglected Tropical DiseasesN Aright ForestNo ratings yet
- SG Policy Brief On Covid-19 Impact On Africa May 2020 PDFDocument28 pagesSG Policy Brief On Covid-19 Impact On Africa May 2020 PDFrajasekar venkatesanNo ratings yet
- Reaction PaperDocument6 pagesReaction PaperJezell De Torres-dela CruzNo ratings yet
- Global Surveillance of Communicable Diseases: Special IssueDocument4 pagesGlobal Surveillance of Communicable Diseases: Special IssueMuhammad Hafiidh MuizzNo ratings yet
- Covid 19Document9 pagesCovid 19Dagi AbebawNo ratings yet
- COVID-19: Too Little, Too Late? The Lancet Published: March 07,2020Document2 pagesCOVID-19: Too Little, Too Late? The Lancet Published: March 07,2020Jamica Anne CostinianoNo ratings yet
- HIV and Conflict ReportDocument39 pagesHIV and Conflict ReportTobi CrackNo ratings yet
- Tropical Med Int Health - 2009 - Mendis - From Malaria Control To Eradication The WHO PerspectiveDocument8 pagesTropical Med Int Health - 2009 - Mendis - From Malaria Control To Eradication The WHO PerspectiveDircia D'silvaNo ratings yet
- Complex Emergencies - Update and Policy RecommendationsDocument6 pagesComplex Emergencies - Update and Policy RecommendationsSBolgerNo ratings yet
- Climate MigrationDocument1 pageClimate MigrationNatalia García100% (1)
- Position Paper MUNDocument3 pagesPosition Paper MUNainaNo ratings yet
- Pandemic Pol ROBERTS - Adam Pandemics - Politics 2020Document35 pagesPandemic Pol ROBERTS - Adam Pandemics - Politics 2020Jorge MalcaNo ratings yet
- FMSC Research - TB and HivDocument11 pagesFMSC Research - TB and Hivapi-608287742No ratings yet
- Dyadic Work VENTE, PALMADocument2 pagesDyadic Work VENTE, PALMAAdrian Christopher Cuevas VenteNo ratings yet
- Lesson 1 - Who Global Health SituationDocument5 pagesLesson 1 - Who Global Health SituationA CNo ratings yet
- HIV/AIDS in The Last 10 Years: Abdalla Sidahmed OsmanDocument7 pagesHIV/AIDS in The Last 10 Years: Abdalla Sidahmed OsmanMichelle BritanicoNo ratings yet
- What Happens To Freedom of Movement Duri PDFDocument7 pagesWhat Happens To Freedom of Movement Duri PDFMaría MazzantiNo ratings yet
- France AL Position Paper 3 FinalDocument2 pagesFrance AL Position Paper 3 FinalPhil KazembeNo ratings yet
- MUN PositionpaperDocument3 pagesMUN PositionpaperchingkuoyNo ratings yet
- Piis0140673615608583 PDFDocument18 pagesPiis0140673615608583 PDFCharles AugustusNo ratings yet
- Age of PandemicDocument12 pagesAge of PandemicDavide FalcioniNo ratings yet
- Out of The Bretton Woods How The AIIB Is DifferentDocument5 pagesOut of The Bretton Woods How The AIIB Is DifferentEl JuancezNo ratings yet
- Is Greece To Blame For The CrisisDocument8 pagesIs Greece To Blame For The CrisisEl JuancezNo ratings yet
- China's Soft-Power Push The Search For RespectDocument7 pagesChina's Soft-Power Push The Search For RespectEl JuancezNo ratings yet
- Frozen Conflicts in The Post-Soviet Space PDFDocument19 pagesFrozen Conflicts in The Post-Soviet Space PDFEl JuancezNo ratings yet
- Empire of The Geeks Silicon Valley Should Be Celebrated. But Its Insularity Risks A BacklashDocument3 pagesEmpire of The Geeks Silicon Valley Should Be Celebrated. But Its Insularity Risks A BacklashEl JuancezNo ratings yet
- Improving - Humanitarian Aid How To Make Relief More Efficient - and EffectiveDocument8 pagesImproving - Humanitarian Aid How To Make Relief More Efficient - and EffectiveEl JuancezNo ratings yet
- Bentham's Fallacies, Then and Now by Peter Singer - Project SyndicateDocument3 pagesBentham's Fallacies, Then and Now by Peter Singer - Project SyndicateEl JuancezNo ratings yet
- Israel's Questionable Quixote What Michael Oren Gets Wrong in - AllyDocument4 pagesIsrael's Questionable Quixote What Michael Oren Gets Wrong in - AllyEl JuancezNo ratings yet
- The Death and Life of The Two-State Solution How The Palestinians May Eventually Get Their StateDocument6 pagesThe Death and Life of The Two-State Solution How The Palestinians May Eventually Get Their StateEl JuancezNo ratings yet
- G (Reece) 2KHow To Contain Athens' Economic ProblemsDocument2 pagesG (Reece) 2KHow To Contain Athens' Economic ProblemsEl JuancezNo ratings yet
- More Data, More Problems Surveillance and The Information EconomyDocument4 pagesMore Data, More Problems Surveillance and The Information EconomyEl JuancezNo ratings yet
- Tehran's Power Lobby How Energy Concerns Drive The Nuclear DealDocument3 pagesTehran's Power Lobby How Energy Concerns Drive The Nuclear DealEl JuancezNo ratings yet
- India Flexes Its Muscle Behind New DElhi's Assertive Foreign PolicyDocument2 pagesIndia Flexes Its Muscle Behind New DElhi's Assertive Foreign PolicyEl JuancezNo ratings yet
- Pengaruh Prenatal Care Yoga Terhadap Pengurangan Keluhan Ketidaknyamanan Ibu Hamil Trimester Iii Di Puskesmas Putri Ayukota JambiDocument6 pagesPengaruh Prenatal Care Yoga Terhadap Pengurangan Keluhan Ketidaknyamanan Ibu Hamil Trimester Iii Di Puskesmas Putri Ayukota JambiWahyu ItuwsiTriNo ratings yet
- Pathophysiology of Acute CholecystitisDocument2 pagesPathophysiology of Acute CholecystitisKush KhannaNo ratings yet
- Copar-RU Maternal and Child HealthDocument16 pagesCopar-RU Maternal and Child HealthMichelle ThereseNo ratings yet
- Intrinsic and Extrinsic Incubation PeriodDocument5 pagesIntrinsic and Extrinsic Incubation PeriodCirimpei PaulNo ratings yet
- Rights and Obligations of PatientsDocument10 pagesRights and Obligations of PatientsRey BenítezNo ratings yet
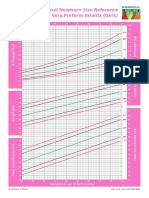
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- Records & Reports Maintained at Sub-Centre and PHCDocument32 pagesRecords & Reports Maintained at Sub-Centre and PHCLakshmi Seth87% (15)
- Hazard Identification and Risk AssessmentDocument4 pagesHazard Identification and Risk AssessmentsibusisoNo ratings yet
- 2020 PIDSR WeeklDocument1 page2020 PIDSR WeeklErrol LlanesNo ratings yet
- Moderna Eua-Fact-Sheet-ProvidersDocument38 pagesModerna Eua-Fact-Sheet-ProvidersJuan PaoloNo ratings yet
- What Causes Teenage Pregnancy?Document2 pagesWhat Causes Teenage Pregnancy?Girlie Faith Morales BrozasNo ratings yet
- Coronavirus Transmission - How COVID-19 Spreads - WorldometerDocument3 pagesCoronavirus Transmission - How COVID-19 Spreads - WorldometerRondeep BoraNo ratings yet
- Adigrat Inception Report Draft PDFDocument126 pagesAdigrat Inception Report Draft PDFAnonymous TvOpvX100% (3)
- COVID Handbook and Outbreak Management Plan (4974)Document32 pagesCOVID Handbook and Outbreak Management Plan (4974)Rachit SharmaNo ratings yet
- SCI 241 Course SyllabusDocument13 pagesSCI 241 Course SyllabusuopfinancestudentNo ratings yet
- The Epidemic Diseases Act, 1897Document8 pagesThe Epidemic Diseases Act, 1897SinghNo ratings yet
- Schemes (Part 4) - HealthDocument17 pagesSchemes (Part 4) - HealthbwerNo ratings yet
- Health Quarter 3 - Module Health Trends, Issues and Concerns (Global Level)Document22 pagesHealth Quarter 3 - Module Health Trends, Issues and Concerns (Global Level)Mary Cris GoNo ratings yet
- Biological Incident Annex To The Response and Recovery Federal Interagency Operational PlansDocument143 pagesBiological Incident Annex To The Response and Recovery Federal Interagency Operational Planssnausages100% (1)
- Joint Effort For Elimination of Tuberculosis (Jeet)Document2 pagesJoint Effort For Elimination of Tuberculosis (Jeet)Arindam MoitraNo ratings yet
- Immunization Safety SurveillanceDocument14 pagesImmunization Safety SurveillanceHIRA DASNo ratings yet
- Vaccination List: Belyaletdinov, Ravil AbdulverovichDocument5 pagesVaccination List: Belyaletdinov, Ravil AbdulverovichCarlos MoriNo ratings yet
- Roles and Responsibilities of Bhws in The AreaDocument13 pagesRoles and Responsibilities of Bhws in The AreaFret Ramirez Coronia RN71% (7)
- (August 24, 2021) Framework For Maternal and Child Nursing - NCM 33 LectureDocument4 pages(August 24, 2021) Framework For Maternal and Child Nursing - NCM 33 LectureMa. Ferimi Gleam BajadoNo ratings yet
- Journal of Equine Veterinary Science - IEIDC 2016Document112 pagesJournal of Equine Veterinary Science - IEIDC 2016Micaela SantangeloNo ratings yet
- Coronavirus (Covid-19) Hub - Latest News & ResearchDocument9 pagesCoronavirus (Covid-19) Hub - Latest News & ResearchrichardonNo ratings yet
- Service Delivery in Rural Areas: by Dennis PoppDocument13 pagesService Delivery in Rural Areas: by Dennis PoppnathanrengaNo ratings yet
- Clinical Presentation On Child With Neonatal SepsisDocument37 pagesClinical Presentation On Child With Neonatal SepsisSREEDEVI T SURESHNo ratings yet
- Dylan CharlesDocument2 pagesDylan CharlesHafni KumarNo ratings yet
- Melliene Semblante's AbstractDocument2 pagesMelliene Semblante's AbstractCMU - College of Forestry and Environmental ScienceNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (39)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (84)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (3)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- The Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeFrom EverandThe Fun Habit: How the Pursuit of Joy and Wonder Can Change Your LifeRating: 4.5 out of 5 stars4.5/5 (19)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- The Story of Philosophy: The Lives and Opinions of the Greater PhilosophersFrom EverandThe Story of Philosophy: The Lives and Opinions of the Greater PhilosophersNo ratings yet