You might also like
- Causes of Domestic ViolenceDocument14 pagesCauses of Domestic ViolenceIan AbraganNo ratings yet
- Healing From Infidelity Book: A Comprehensive Guide to Coping with Betrayal, Rebuilding Trust, and Moving ForwardFrom EverandHealing From Infidelity Book: A Comprehensive Guide to Coping with Betrayal, Rebuilding Trust, and Moving ForwardNo ratings yet
- Overcoming Emotional Unavailability in Marriage: Practical Strategies for Recognizing, Dealing and Healing Emotionally Unavailable SpouseFrom EverandOvercoming Emotional Unavailability in Marriage: Practical Strategies for Recognizing, Dealing and Healing Emotionally Unavailable SpouseNo ratings yet
- Jealousy - How to Understand and Trust Your Partner and Deal with Insecurity in Your RelationshipFrom EverandJealousy - How to Understand and Trust Your Partner and Deal with Insecurity in Your RelationshipRating: 5 out of 5 stars5/5 (2)
- Coping With Family Stress After Chronic Illness or DeathFrom EverandCoping With Family Stress After Chronic Illness or DeathNo ratings yet
- A New Tried And Tested Routine For Getting Over Breakup Fast: Turning your pain to gainFrom EverandA New Tried And Tested Routine For Getting Over Breakup Fast: Turning your pain to gainNo ratings yet
- Overcoming Overthinking In Relationships: The Art of Setting Boundaries, Understanding Attachment, Effective Communication & Moving Beyond Anxiety, Jealousy & Insecurity: Develop Effective Communication Abilities, Overcome Awkwardness, Talk To Anyone, Make Friends & Create Deeper ConnectionsFrom EverandOvercoming Overthinking In Relationships: The Art of Setting Boundaries, Understanding Attachment, Effective Communication & Moving Beyond Anxiety, Jealousy & Insecurity: Develop Effective Communication Abilities, Overcome Awkwardness, Talk To Anyone, Make Friends & Create Deeper ConnectionsNo ratings yet
- Emotion and Copin1Document24 pagesEmotion and Copin1Anneliese FernandesNo ratings yet
- Dysfunctional FamilyDocument4 pagesDysfunctional FamilymahvishkhNo ratings yet
- Exploring the Roots of Your Marriage: Understanding the Influence of the Family of OriginFrom EverandExploring the Roots of Your Marriage: Understanding the Influence of the Family of OriginNo ratings yet
- Healing from Infidelity: How to Let Go, Recover, Rebuild trust and ThriveFrom EverandHealing from Infidelity: How to Let Go, Recover, Rebuild trust and ThriveRating: 4 out of 5 stars4/5 (2)
- How to Deal With Emotionally Immature Parents: Healing from Narcissistic, Authoritarian, Permissive, Enmeshed, or Absent Parents: Generational Healing, #2From EverandHow to Deal With Emotionally Immature Parents: Healing from Narcissistic, Authoritarian, Permissive, Enmeshed, or Absent Parents: Generational Healing, #2No ratings yet
- Change Your Mind: Co-Parenting in High Conflict Custody CasesFrom EverandChange Your Mind: Co-Parenting in High Conflict Custody CasesNo ratings yet
- Personality DisordersDocument8 pagesPersonality Disordersapi-211671182No ratings yet
- Empath Mastery: Understanding the Emotions of Highly Sensitive PeopleFrom EverandEmpath Mastery: Understanding the Emotions of Highly Sensitive PeopleNo ratings yet
- Natalie Wilson Big Essay 2Document10 pagesNatalie Wilson Big Essay 2api-582873643No ratings yet
- Coping With Family Stress After Reye's SyndromeFrom EverandCoping With Family Stress After Reye's SyndromeNo ratings yet
- Overcoming Overthinking In Relationships: Develop Mindful Loving Habits, Effective Communication, Overcome Overthinking, Jealousy, Insecurity, Negative Thinking & Deepen Your ConnectionFrom EverandOvercoming Overthinking In Relationships: Develop Mindful Loving Habits, Effective Communication, Overcome Overthinking, Jealousy, Insecurity, Negative Thinking & Deepen Your ConnectionNo ratings yet
- Unburdened: Liberating Your True Self from Emotionally Immature ParentsFrom EverandUnburdened: Liberating Your True Self from Emotionally Immature ParentsNo ratings yet
- Anger Management: How to Manage Your Anger, Control Your Emotions and Handle Behavioral Issues in Adults or Children.From EverandAnger Management: How to Manage Your Anger, Control Your Emotions and Handle Behavioral Issues in Adults or Children.Rating: 5 out of 5 stars5/5 (1)
- 50 Ways to Love Your Stepparent: Approaching the Heart With a Rational MindFrom Everand50 Ways to Love Your Stepparent: Approaching the Heart With a Rational MindNo ratings yet
- Psychoanalytic Family TherapyDocument34 pagesPsychoanalytic Family Therapyiragirl100% (2)
- Summary of It Didn’t Start With You by Mark Wolynn :How Inherited Family Trauma Shapes Who We Are and How to End the Cycle: FRANCIS Books, #1From EverandSummary of It Didn’t Start With You by Mark Wolynn :How Inherited Family Trauma Shapes Who We Are and How to End the Cycle: FRANCIS Books, #1No ratings yet
- Inferiority ComplexDocument5 pagesInferiority Complexb.tareNo ratings yet
- DISORGANIZED ATTACHMENT: How Early Trauma Affects Attachment Style and What You Can Do About It (2023 Guide for Beginners)From EverandDISORGANIZED ATTACHMENT: How Early Trauma Affects Attachment Style and What You Can Do About It (2023 Guide for Beginners)No ratings yet
- What Does Research Tell Us About Healthy RelationshipsDocument4 pagesWhat Does Research Tell Us About Healthy RelationshipsyagnapalrajuNo ratings yet
- Family-Dynamics 095321Document32 pagesFamily-Dynamics 095321hibebe143No ratings yet
- Happy Children A Complete Guide to Smart Parenting through DivorceFrom EverandHappy Children A Complete Guide to Smart Parenting through DivorceNo ratings yet
- Salas Bowen TheoryDocument32 pagesSalas Bowen TheoryJade Harris ColorjeNo ratings yet
- 50 Ways to Love Your Parents: Approaching the Heart With a Rational MindFrom Everand50 Ways to Love Your Parents: Approaching the Heart With a Rational MindNo ratings yet
- How to Deal with a Narcissist: A 4-in-1 Book Bundle: Exposing Covert Narcissism, Surviving Co-Parenting Challenges, Harnessing Empath Abilities, and Triumphing Over Narcissistic Abuse.: NarcissismFrom EverandHow to Deal with a Narcissist: A 4-in-1 Book Bundle: Exposing Covert Narcissism, Surviving Co-Parenting Challenges, Harnessing Empath Abilities, and Triumphing Over Narcissistic Abuse.: NarcissismNo ratings yet
- Heitler (2018) Parental Alienation Syndrome What Is It Who Does ItDocument3 pagesHeitler (2018) Parental Alienation Syndrome What Is It Who Does ItShawn A. WygantNo ratings yet
- Set Healthy Boundaries & Overthinking In Relationships Cure (2 in 1): Develop Effective Communication, Overcome Anxiety, Prevent Co-Dependency & Your Love: Develop Effective Communication, Overcome Anxiety, Prevent Co-dependency & Your Love: Develop Effective Communication, Overcome Anxiety, Prevent Codependency & Your LoveFrom EverandSet Healthy Boundaries & Overthinking In Relationships Cure (2 in 1): Develop Effective Communication, Overcome Anxiety, Prevent Co-Dependency & Your Love: Develop Effective Communication, Overcome Anxiety, Prevent Co-dependency & Your Love: Develop Effective Communication, Overcome Anxiety, Prevent Codependency & Your LoveNo ratings yet
- Counseling Troubled Couple and Conflicting Family RelationshipDocument4 pagesCounseling Troubled Couple and Conflicting Family Relationshipmiji_ggNo ratings yet
- Bowenian Family TherapyDocument7 pagesBowenian Family TherapyCybill BlakeNo ratings yet
- 10 1023@a@1005167926689Document15 pages10 1023@a@1005167926689M. MikeNo ratings yet
- Emotional Abuse: How to Stop Emotional Abuse From Ruining Your Life and A Powerful Program to Help You Recover From Emotional AbuseFrom EverandEmotional Abuse: How to Stop Emotional Abuse From Ruining Your Life and A Powerful Program to Help You Recover From Emotional AbuseRating: 4 out of 5 stars4/5 (1)
- Codependency: The Ultimate Guide to Breaking Free from Emotional Abuse. Stop Codependent and Toxic Relationships and Start Recovering Your Life.From EverandCodependency: The Ultimate Guide to Breaking Free from Emotional Abuse. Stop Codependent and Toxic Relationships and Start Recovering Your Life.No ratings yet
- Love Is Never Enough: How Couples Can Overcome MisunderstandingFrom EverandLove Is Never Enough: How Couples Can Overcome MisunderstandingRating: 4 out of 5 stars4/5 (21)
- Adolescents and Parental Divorce: Helping Teens Thrive When Families DivideFrom EverandAdolescents and Parental Divorce: Helping Teens Thrive When Families DivideNo ratings yet
- Dyfunctional Family Term PaperDocument28 pagesDyfunctional Family Term PaperKing Solomon100% (1)
- Jealousy Unraveled: A Guide To Overcoming Insecurity And Building Trust In LoveFrom EverandJealousy Unraveled: A Guide To Overcoming Insecurity And Building Trust In LoveNo ratings yet
- Fear of IntimacyDocument9 pagesFear of IntimacyHelsi MayaNo ratings yet
- Commitment PhobiaDocument2 pagesCommitment Phobiarajkumar_umakanthamNo ratings yet
- Understanding Dysfunctional Relationship Patterns in Your FamilyDocument3 pagesUnderstanding Dysfunctional Relationship Patterns in Your FamilykielmaticsNo ratings yet
- Narcissistic Mothers: The Ultimate Emotional Abuse Recovery Guide. Learn How to Overcome Anxiety and Stop Manipulation. Start Healing from Toxic Parents and Finally Take Control of Your Emotions.From EverandNarcissistic Mothers: The Ultimate Emotional Abuse Recovery Guide. Learn How to Overcome Anxiety and Stop Manipulation. Start Healing from Toxic Parents and Finally Take Control of Your Emotions.Rating: 3 out of 5 stars3/5 (2)
- Emotionally Abusive RelationshipsDocument4 pagesEmotionally Abusive RelationshipsJin Lyn100% (2)
- The Relationship Between Husband and WifeDocument46 pagesThe Relationship Between Husband and Wifejcf12930100% (1)
- The Perfect Family Storm: Tips to Restore Mental Health and Strengthen Family Relationships in Today's WorldFrom EverandThe Perfect Family Storm: Tips to Restore Mental Health and Strengthen Family Relationships in Today's WorldNo ratings yet
- Family and PsychopathologyDocument7 pagesFamily and Psychopathologyaastha jainNo ratings yet
- Emotional Abuse: How To Recognize Narcissistic Abuse in Relationship and Learn to Defend Yourself Against Dark Psychology by Reacting to Passive Codependency with Self-esteem and Self-confidence.From EverandEmotional Abuse: How To Recognize Narcissistic Abuse in Relationship and Learn to Defend Yourself Against Dark Psychology by Reacting to Passive Codependency with Self-esteem and Self-confidence.Rating: 5 out of 5 stars5/5 (3)
- Jerath (2016) Pranayamic BreathingDocument2 pagesJerath (2016) Pranayamic BreathingShawn A. WygantNo ratings yet
- Wang (2013) Effects of Qigong Anxiety Depression Psychological Well-BeingDocument17 pagesWang (2013) Effects of Qigong Anxiety Depression Psychological Well-BeingShawn A. WygantNo ratings yet
- Chow (2011) Qigong Wellness DissertationDocument353 pagesChow (2011) Qigong Wellness DissertationShawn A. WygantNo ratings yet
- Vasilyuk (1991) The Psychology of ExperiencingDocument259 pagesVasilyuk (1991) The Psychology of ExperiencingShawn A. WygantNo ratings yet
- Osborne (2008) CH 22 Testing The Assumptions of Analysis of VarianceDocument29 pagesOsborne (2008) CH 22 Testing The Assumptions of Analysis of VarianceShawn A. WygantNo ratings yet
- Interventive I - K. TommDocument11 pagesInterventive I - K. TommlocologoNo ratings yet
- Neil J. Salkind - Encyclopedia of Research Design (2010, SAGE Publications, Inc) PDFDocument1,644 pagesNeil J. Salkind - Encyclopedia of Research Design (2010, SAGE Publications, Inc) PDFMark Cervantes91% (11)
- Glossary 03 (Aron, 2013)Document14 pagesGlossary 03 (Aron, 2013)Shawn A. WygantNo ratings yet
- Kopetski (1998) Parental Alienation Syndrome Part II. 27-MAR - COLAW - 61Document8 pagesKopetski (1998) Parental Alienation Syndrome Part II. 27-MAR - COLAW - 61Shawn A. WygantNo ratings yet
- Black (1999) Doing Quantitative Research Social SciencesDocument541 pagesBlack (1999) Doing Quantitative Research Social SciencesShawn A. WygantNo ratings yet
- Kopetski (1998) Parental Alienation Syndrome Part II. 27-MAR - COLAW - 61Document8 pagesKopetski (1998) Parental Alienation Syndrome Part II. 27-MAR - COLAW - 61Shawn A. WygantNo ratings yet
- Shaw (2016) Commentary Examining The Use of Parental Alienation SyndromeDocument4 pagesShaw (2016) Commentary Examining The Use of Parental Alienation SyndromeShawn A. WygantNo ratings yet
- Kopetski (1998) Parental Alienation Syndrome Part II. 27-MAR - COLAW - 61Document8 pagesKopetski (1998) Parental Alienation Syndrome Part II. 27-MAR - COLAW - 61Shawn A. WygantNo ratings yet
- Engel (1977) Need New Medical Model Challenge BiomedicineDocument9 pagesEngel (1977) Need New Medical Model Challenge BiomedicineShawn A. WygantNo ratings yet
- Elzer (2014) Psychoanalytic Psychotherapy Handbook KARNACDocument345 pagesElzer (2014) Psychoanalytic Psychotherapy Handbook KARNACShawn A. Wygant100% (2)
- Hlista v. Altevogt Court Decision on Clean Hands DoctrineDocument8 pagesHlista v. Altevogt Court Decision on Clean Hands DoctrineShawn A. WygantNo ratings yet
- Walker (2006) Extreme Consequence Parental Alienation Syndrome Richard LohstrohDocument19 pagesWalker (2006) Extreme Consequence Parental Alienation Syndrome Richard LohstrohShawn A. WygantNo ratings yet
- Visser (2016) Interparental Violence Mother-Child Emotion Dialogues in Families Parental AlienationDocument22 pagesVisser (2016) Interparental Violence Mother-Child Emotion Dialogues in Families Parental AlienationShawn A. WygantNo ratings yet
- Fairy Tales and Script Drama AnalysisDocument5 pagesFairy Tales and Script Drama AnalysisAdriana Cristina SaraceanuNo ratings yet
- Script Drama AnalysisDocument17 pagesScript Drama Analysisanagard2593No ratings yet
- Dallam (2016) Recommended Treatments Parental Alienation Cause Psychological Harm To Children PDFDocument11 pagesDallam (2016) Recommended Treatments Parental Alienation Cause Psychological Harm To Children PDFShawn A. WygantNo ratings yet
- Saunders (2016) Battered Women Negative Consequences Child Custody Parental AlienationDocument25 pagesSaunders (2016) Battered Women Negative Consequences Child Custody Parental AlienationShawn A. Wygant100% (1)
- Summers (2006) Unadulterated Arrogance Autopsy of The Narcissistic Parental Alienator PDFDocument31 pagesSummers (2006) Unadulterated Arrogance Autopsy of The Narcissistic Parental Alienator PDFShawn A. WygantNo ratings yet
- Heitler (2018) Parental Alienation Syndrome What Is It Who Does ItDocument3 pagesHeitler (2018) Parental Alienation Syndrome What Is It Who Does ItShawn A. WygantNo ratings yet
- O'Donohue (2016) Examining The Validity of Parental Alienation SyndromeDocument14 pagesO'Donohue (2016) Examining The Validity of Parental Alienation SyndromeShawn A. WygantNo ratings yet
- Munchausen by Proxy: A Collaborative Approach to Investigation, Assessment and TreatmentDocument29 pagesMunchausen by Proxy: A Collaborative Approach to Investigation, Assessment and TreatmentShawn A. WygantNo ratings yet
- The Impact On An Abusive Family Context On ChildhoodDocument19 pagesThe Impact On An Abusive Family Context On ChildhoodRosolimou EviNo ratings yet
- Falshaw Et Al (1996) - Victim To Offender - A Review. Aggression and Violent Behavior, 1 (4), 389-404 PDFDocument16 pagesFalshaw Et Al (1996) - Victim To Offender - A Review. Aggression and Violent Behavior, 1 (4), 389-404 PDFShawn A. WygantNo ratings yet
- Clemente (2016) When Courts Accept What Science Rejects Parental Alienation SyndromeDocument9 pagesClemente (2016) When Courts Accept What Science Rejects Parental Alienation SyndromeShawn A. WygantNo ratings yet
- All India Institute of Medical SciencesDocument3 pagesAll India Institute of Medical SciencesNaresh BeatsNo ratings yet
- Case Study of Bronchial Asthma in Acute ExacerbationDocument16 pagesCase Study of Bronchial Asthma in Acute Exacerbationdextroid1290% (29)
- Weeks 3 & 4 - Oral CommunicationDocument7 pagesWeeks 3 & 4 - Oral CommunicationClaire CaraigNo ratings yet
- Research Proposal 4Document3 pagesResearch Proposal 4api-385647692No ratings yet
- Principles of Monitoring & Evaluation - NotesDocument113 pagesPrinciples of Monitoring & Evaluation - NotesKeith100% (2)
- f3 Home-Sci Simplified Notes SPDocument20 pagesf3 Home-Sci Simplified Notes SPmicah isabokeNo ratings yet
- Being in The World Selected Pa Ludwig BinswangerDocument388 pagesBeing in The World Selected Pa Ludwig BinswangerRamazan ÇarkıNo ratings yet
- Alternative Feed for ChickensDocument28 pagesAlternative Feed for ChickensClaudens Printing ServicesNo ratings yet
- Anxiety NeurosisDocument34 pagesAnxiety Neurosisilakkiya ilakkiyaNo ratings yet
- Combined Science: Trilogy: 8464/B/1F - Biology Paper 1 Foundation Tier Mark SchemeDocument22 pagesCombined Science: Trilogy: 8464/B/1F - Biology Paper 1 Foundation Tier Mark SchemeLabeenaNo ratings yet
- Stress ManagementDocument20 pagesStress ManagementSagar Bhoite100% (1)
- Risk ManagementDocument15 pagesRisk ManagementABEGAIL MADLAONo ratings yet
- [Journal of Autism and Childhood Schizophrenia vol. 49 iss. 6] Ng, Rowena_ Heinrich, Kimberley_ Hodges, Elise K. - Brief Report_ Neuropsychological Testing and Informant-Ratings of Children with Autism Spectrum Disorder, Atten - libgen.liDocument8 pages[Journal of Autism and Childhood Schizophrenia vol. 49 iss. 6] Ng, Rowena_ Heinrich, Kimberley_ Hodges, Elise K. - Brief Report_ Neuropsychological Testing and Informant-Ratings of Children with Autism Spectrum Disorder, Atten - libgen.ligustavNo ratings yet
- ExampleDocument12 pagesExampleEmma May De MesaNo ratings yet
- Coronavirus:: Separating The Facts From The FearDocument4 pagesCoronavirus:: Separating The Facts From The FearKhairur RijjalNo ratings yet
- How To Stop Loving Someone Who Doesn't Love You: Part 1 of 4: Giving Yourself SpaceDocument17 pagesHow To Stop Loving Someone Who Doesn't Love You: Part 1 of 4: Giving Yourself SpaceDariz MillerNo ratings yet
- CSP Chintu Anna - 1Document12 pagesCSP Chintu Anna - 1sujithNo ratings yet
- Prof Prac 2 EssayDocument3 pagesProf Prac 2 EssayEryka DyenghongNo ratings yet
- Cdmgens00160 PDFDocument111 pagesCdmgens00160 PDFMohammadMasoomParwezNo ratings yet
- Roth - From Free WombDocument19 pagesRoth - From Free WombNubss SSNo ratings yet
- Digital Citizenship vs. Global CitizenshipDocument20 pagesDigital Citizenship vs. Global CitizenshipMacasinag Jamie Anne M.No ratings yet
- FMU 101 - Chap 4 - Test Taking Strategies Part IIDocument11 pagesFMU 101 - Chap 4 - Test Taking Strategies Part IIMario LaraNo ratings yet
- Chemical Management PolicyDocument9 pagesChemical Management PolicySaifullah SherajiNo ratings yet
- Haidh, Istihadah and WiladahDocument14 pagesHaidh, Istihadah and WiladahHeartNo ratings yet
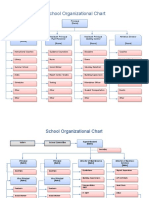
- School Organizational ChartDocument4 pagesSchool Organizational ChartislahNo ratings yet
- EKG Study GuideDocument45 pagesEKG Study GuideBrawner100% (6)
- S7 ManualDocument308 pagesS7 ManualBenjamin MurphyNo ratings yet
- Continuous Monitoring of Erns: Set of Ern Core IndicatorsDocument23 pagesContinuous Monitoring of Erns: Set of Ern Core IndicatorsElenaNo ratings yet
- 1393un 2023-03Document94 pages1393un 2023-03Marcela Martínez100% (1)
- Graded RecitationDocument22 pagesGraded RecitationClara MaeNo ratings yet
























































































![[Journal of Autism and Childhood Schizophrenia vol. 49 iss. 6] Ng, Rowena_ Heinrich, Kimberley_ Hodges, Elise K. - Brief Report_ Neuropsychological Testing and Informant-Ratings of Children with Autism Spectrum Disorder, Atten - libgen.li](https://imgv2-1-f.scribdassets.com/img/document/596448205/149x198/c66e65b0ff/1710588633?v=1)