You might also like
- Streptococcus Infection, On TheDocument3 pagesStreptococcus Infection, On TheMonica DomingoNo ratings yet
- 7 Renal Disease Student CopyDocument34 pages7 Renal Disease Student Copyrbm121415chyNo ratings yet
- Analysis of Urine and Body Fluids w8Document3 pagesAnalysis of Urine and Body Fluids w8Cheska ReyesNo ratings yet
- Disorder Etiology: Acute GlomerulonephritisDocument1 pageDisorder Etiology: Acute GlomerulonephritisChynna Izzabelle Alcantara AbellanaNo ratings yet
- Activity On Renal DiseasesDocument6 pagesActivity On Renal DiseasesRicca Christyl SumalpongNo ratings yet
- Chapter 7Document2 pagesChapter 7Mychelle MenesNo ratings yet
- Renal DiseaseDocument6 pagesRenal DiseaseyeonjiNo ratings yet
- Renal and Metabolic DiseasesDocument5 pagesRenal and Metabolic DiseasesAry OuiNo ratings yet
- Renal Failure en 2Document103 pagesRenal Failure en 2ezz sharabyNo ratings yet
- Renal Diseases NotesDocument4 pagesRenal Diseases NotesJanine CabreraNo ratings yet
- Stras Renal DiseaseDocument3 pagesStras Renal Diseaseacer14appleNo ratings yet
- Glomerular Disorders - GlomerulonephrtisDocument56 pagesGlomerular Disorders - GlomerulonephrtisValerie Suge-MichiekaNo ratings yet
- Aubf RenaallllllllDocument7 pagesAubf RenaallllllllMarienel PingolNo ratings yet
- 7 AUBF Lec 7Document6 pages7 AUBF Lec 7Marlyn BorilloNo ratings yet
- Renal DiseaseDocument5 pagesRenal DiseasefeajhanineladagaNo ratings yet
- Chapter 8 - Renal DiseaseDocument7 pagesChapter 8 - Renal DiseaseCha GuingabNo ratings yet
- AUBF-UT-DISORDER-TRANSES-FINALSDocument2 pagesAUBF-UT-DISORDER-TRANSES-FINALSElijah Mae MundocNo ratings yet
- Clinical Microscopy ReviewerDocument31 pagesClinical Microscopy ReviewerbokbokbokNo ratings yet
- glomerulonephritisDocument28 pagesglomerulonephritisqayyum consultantfpscNo ratings yet
- AUB - Renal DiseasesDocument2 pagesAUB - Renal DiseasesJeanne RodiñoNo ratings yet
- AUBF Lec Week#8 Renal DiseasesDocument10 pagesAUBF Lec Week#8 Renal DiseasesLexaNatalieConcepcionJuntadoNo ratings yet
- Glomer Ds TadDocument190 pagesGlomer Ds TadHaileprince MekonnenNo ratings yet
- AUBF FinalsDocument62 pagesAUBF FinalsAlthea Jam Grezshyl GaloNo ratings yet
- Glomerulonephritis: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK Tim Ginjal Hipertensi Unhas 2019Document68 pagesGlomerulonephritis: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK Tim Ginjal Hipertensi Unhas 2019uzan100% (1)
- L20 - Glomerular DiseasesDocument34 pagesL20 - Glomerular Diseasesabdideba6No ratings yet
- Acute Glomerulonephritis: Best PracticeDocument8 pagesAcute Glomerulonephritis: Best PracticeMichael HusainNo ratings yet
- AUBF Lec - Renal DiseasesDocument6 pagesAUBF Lec - Renal Diseasescdsteenkamp18No ratings yet
- Renal DiseasesDocument7 pagesRenal DiseasesXyleene Jency Bien IINo ratings yet
- Renal DisordersDocument28 pagesRenal DisordersChristine CalumaNo ratings yet
- Renal DiseaseDocument4 pagesRenal DiseaseApril Lady Faith P. PaundogNo ratings yet
- Lecture 4. Pathology Anatomy of Urinary SystemDocument53 pagesLecture 4. Pathology Anatomy of Urinary SystemkrisnadewirahadiNo ratings yet
- Acute Glomerulonephritis: Best PracticeDocument8 pagesAcute Glomerulonephritis: Best PracticeWenny A. YuliantiNo ratings yet
- Renal Disease 2023Document9 pagesRenal Disease 2023MaeNo ratings yet
- Acute Glomerulonephritis: Best PracticeDocument9 pagesAcute Glomerulonephritis: Best PracticeAjeng DwiNo ratings yet
- Glomdis - GanlinDocument118 pagesGlomdis - GanlinMEDS easyNo ratings yet
- PATH - Nephritic SyndromeDocument14 pagesPATH - Nephritic SyndromeMuhamad Zul ImanNo ratings yet
- WSU Renal ReviewDocument100 pagesWSU Renal ReviewLeticia BornsteinNo ratings yet
- LEC AUBF Renal-Diseases MIDTERMS 02Document3 pagesLEC AUBF Renal-Diseases MIDTERMS 02Jashmine May TadinaNo ratings yet
- Renal Diseases: Pathology Department University Surakarta For Medical SciencesDocument43 pagesRenal Diseases: Pathology Department University Surakarta For Medical SciencesKatou Jeffrey ShigehitoNo ratings yet
- Pathology GlomerulonephritisDocument4 pagesPathology GlomerulonephritisGerardLum100% (2)
- Clin Path Lab 6 UrinalysisDocument5 pagesClin Path Lab 6 Urinalysisapi-3743217100% (6)
- Predisposing Factors Precipitating Factors: Streptococcal Pyrogenes and Superantigen ReleasedDocument9 pagesPredisposing Factors Precipitating Factors: Streptococcal Pyrogenes and Superantigen ReleasedDATO-ON JOANA PAULANo ratings yet
- Glomerulonephritis 2019Document31 pagesGlomerulonephritis 2019EsoklailNo ratings yet
- Proteinuria &Document38 pagesProteinuria &Agustinus BethaNo ratings yet
- Glomerular DiseasesDocument31 pagesGlomerular DiseasesLALITH SAI KNo ratings yet
- 05 - GinjalDocument119 pages05 - GinjalAna ambiyaNo ratings yet
- renal-diseasesDocument4 pagesrenal-diseasesJolan Fernando HerceNo ratings yet
- Renal and Cardiovascular Pathology 2Document8 pagesRenal and Cardiovascular Pathology 2Morgan PeggNo ratings yet
- AUBF Group 1 Chapter 8Document12 pagesAUBF Group 1 Chapter 8Gerald John PazNo ratings yet
- ExcreDocument3 pagesExcreKristin Charm MascareñasNo ratings yet
- Kidney (Part 1)Document13 pagesKidney (Part 1)Kathlene EmbodoNo ratings yet
- The Urinary System: Dr. Khan, MD, MCPS, DTCD PA 5402 T/W/RDocument35 pagesThe Urinary System: Dr. Khan, MD, MCPS, DTCD PA 5402 T/W/RCrystal Lynn Keener SciariniNo ratings yet
- NEPHROTIC SYNDROME - HamidDocument20 pagesNEPHROTIC SYNDROME - HamidAbdul Hamid OmarNo ratings yet
- Glomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesDocument6 pagesGlomerular Diseases: Pathogenesis of Glomerular Diseases Progression of Glomerular DiseasesSeff CausapinNo ratings yet
- Acute Glomerulonephritis: Postgraduate Medical Journal May 2003Document9 pagesAcute Glomerulonephritis: Postgraduate Medical Journal May 2003Sa7arNo ratings yet
- Screenshot 2022-12-05 at 15.41.06Document122 pagesScreenshot 2022-12-05 at 15.41.06Senuri ManthripalaNo ratings yet
- Acute Post Streptococcal GlomerulonephritisDocument14 pagesAcute Post Streptococcal GlomerulonephritisDanica Alyssa CruzNo ratings yet
- Test 4 OutlineDocument13 pagesTest 4 Outlinemara5140No ratings yet
- Fast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentFrom EverandFast Facts: Acute and Recurrent Pancreatitis: Using evidence to support treatmentNo ratings yet
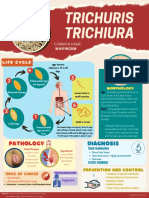
- Trichuris whipworm life cycle and pathologyDocument1 pageTrichuris whipworm life cycle and pathologyAnya IgnacioNo ratings yet
- Enzyme: Specific Proteins That Catalyze Biochemical: Constituents of Enzyme MoleculeDocument6 pagesEnzyme: Specific Proteins That Catalyze Biochemical: Constituents of Enzyme MoleculeAnya IgnacioNo ratings yet
- Enzymology 3Document4 pagesEnzymology 3Anya IgnacioNo ratings yet
- Purine Disorder PDFDocument1 pagePurine Disorder PDFAnya IgnacioNo ratings yet
- Fixation NotesDocument35 pagesFixation NotesAnya IgnacioNo ratings yet
- Lesson 6 - Coccidian PDFDocument11 pagesLesson 6 - Coccidian PDFAnya IgnacioNo ratings yet
- Carbohydrate Disorder PDFDocument1 pageCarbohydrate Disorder PDFAnya IgnacioNo ratings yet
- Quality Assessment, Renal Disease & Urine Screening. (BOOK)Document19 pagesQuality Assessment, Renal Disease & Urine Screening. (BOOK)Anya IgnacioNo ratings yet
- Lesson 6 - Coccidian PDFDocument11 pagesLesson 6 - Coccidian PDFAnya IgnacioNo ratings yet
- Quality Assessment, Renal Disease & Urine ScreeningDocument15 pagesQuality Assessment, Renal Disease & Urine ScreeningAnya IgnacioNo ratings yet
- Lesson 5 Plasmodium SPPDocument8 pagesLesson 5 Plasmodium SPPAnya IgnacioNo ratings yet
- Lesson 5 - PlasmodiumDocument9 pagesLesson 5 - PlasmodiumAnya IgnacioNo ratings yet
- Lesson 6 - Coccidian PDFDocument11 pagesLesson 6 - Coccidian PDFAnya IgnacioNo ratings yet
- Lesson 7 PDFDocument6 pagesLesson 7 PDFAnya IgnacioNo ratings yet
- Lesson 8: Nematodes Part 1 OverviewDocument7 pagesLesson 8: Nematodes Part 1 OverviewAnya IgnacioNo ratings yet
- Enzymology Part 1-2Document12 pagesEnzymology Part 1-2Anya IgnacioNo ratings yet
- Endocrine System: EndocrinologyDocument10 pagesEndocrine System: EndocrinologyAnya IgnacioNo ratings yet
- Coccidians and Filarial WormsDocument11 pagesCoccidians and Filarial WormsAnya IgnacioNo ratings yet
- Myxoviruses: MIDTERM LESSON 2: Respiratory VirusesDocument8 pagesMyxoviruses: MIDTERM LESSON 2: Respiratory VirusesAnya IgnacioNo ratings yet
- Fixation NotesDocument35 pagesFixation NotesAnya IgnacioNo ratings yet
- Clinical Chemistry Notes - AbiDocument34 pagesClinical Chemistry Notes - AbiAnya Ignacio100% (1)
- Clinical Chemistry Quality Control GuideDocument32 pagesClinical Chemistry Quality Control GuideAnya Ignacio100% (1)
- AUBF Microscopic Exam Part 2&3Document13 pagesAUBF Microscopic Exam Part 2&3Anya IgnacioNo ratings yet
- Characteristics of Virus: Characteristic of Cellular LifeDocument6 pagesCharacteristics of Virus: Characteristic of Cellular LifeAnya IgnacioNo ratings yet
- Clinical Chemistry Notes (Blanked) - ABI PDFDocument34 pagesClinical Chemistry Notes (Blanked) - ABI PDFAnya IgnacioNo ratings yet
- The Devil Wears Prada Movie ReviewDocument1 pageThe Devil Wears Prada Movie ReviewAnya IgnacioNo ratings yet
- First Aid Essentials GuideDocument33 pagesFirst Aid Essentials GuidejltarleyNo ratings yet
- OphthalmologyDocument12 pagesOphthalmologyAmy StampNo ratings yet
- Avishek Roy Class12 Bio Project On ThalassemiaDocument20 pagesAvishek Roy Class12 Bio Project On ThalassemiaDazzling DilNo ratings yet
- Delivery DrugsDocument2 pagesDelivery DrugsBernardNo ratings yet
- Pain DiaryDocument4 pagesPain DiaryFrancisco RuizNo ratings yet
- Platelets and Hemostasis ReviewDocument10 pagesPlatelets and Hemostasis Review西矢椛No ratings yet
- Cover LetterDocument2 pagesCover LettersamudraandiNo ratings yet
- GERD Guide: Causes, Symptoms and Treatment for Gastroesophageal Reflux DiseaseDocument7 pagesGERD Guide: Causes, Symptoms and Treatment for Gastroesophageal Reflux DiseaseAlan JacobNo ratings yet
- Drug CefuroximeDocument2 pagesDrug CefuroximeDhan LopezNo ratings yet
- Antihistamines: Author: Kimberly Mulcahy, Pharmd, Bcps Editor: Claudia Lee, RPH, MDDocument16 pagesAntihistamines: Author: Kimberly Mulcahy, Pharmd, Bcps Editor: Claudia Lee, RPH, MDHassan Ait YachouNo ratings yet
- Ophtha Quiz - INI CET High Yield TopicsDocument3 pagesOphtha Quiz - INI CET High Yield TopicsAsif MohammedNo ratings yet
- Genetics and Pathophysiology of Mental Retardation: ReviewDocument13 pagesGenetics and Pathophysiology of Mental Retardation: ReviewAndre OktavianNo ratings yet
- PoliomyelitisDocument13 pagesPoliomyelitisCea Mikee Mitch BartolomeNo ratings yet
- Drugs Used in PregnancyDocument39 pagesDrugs Used in PregnancySneha BencyNo ratings yet
- Grey Flathead Mullet (Mugil Cephalus)Document22 pagesGrey Flathead Mullet (Mugil Cephalus)Karl KiwisNo ratings yet
- DR Tans Balance Method PDFDocument18 pagesDR Tans Balance Method PDFJoy Arguelles GoolNo ratings yet
- Gestational Hypertension and Preeclampsia ACOG.46Document24 pagesGestational Hypertension and Preeclampsia ACOG.46UWIMANA Jean ClaudeNo ratings yet
- Hematologic DiseasesDocument13 pagesHematologic DiseaseshithNo ratings yet
- Mango LeavesDocument5 pagesMango LeavesMuthuswamy JayaramNo ratings yet
- Fever Proforma and Assignment - 1Document48 pagesFever Proforma and Assignment - 1SivaNo ratings yet
- Medical Surgical Nursing 50 ItemsDocument34 pagesMedical Surgical Nursing 50 ItemsNiceniadas CaraballeNo ratings yet
- Guidelines For Preventive Activities in General PracticeDocument382 pagesGuidelines For Preventive Activities in General PracticeDr. Serin KuriakoseNo ratings yet
- Inherited Heart Ano.Document49 pagesInherited Heart Ano.Alec Palcon JovenNo ratings yet
- Methamphetamine Research ReportDocument24 pagesMethamphetamine Research ReportFarhan MasoodNo ratings yet
- Review of Neonatal Calve Diarrhea (Rotavirus)Document12 pagesReview of Neonatal Calve Diarrhea (Rotavirus)Central Asian StudiesNo ratings yet
- Gene PPT RoughDocument18 pagesGene PPT RoughKrish DedhaNo ratings yet
- Neurotherapy JournalDocument14 pagesNeurotherapy JournalNivetha RajendhranNo ratings yet
- Cystic Kidney Disease Guide to Autosomal Dominant and Recessive TypesDocument2 pagesCystic Kidney Disease Guide to Autosomal Dominant and Recessive TypesShams JailaniNo ratings yet
- Differential Diagnosis of Back PainDocument26 pagesDifferential Diagnosis of Back PainKristy Besarab100% (1)
- TCM Case Studies Eye Ear Nose and Throat DisordersDocument61 pagesTCM Case Studies Eye Ear Nose and Throat Disordersmelissa.barlowe30698% (41)