You might also like
- Parasitology Table: ProtozoaDocument10 pagesParasitology Table: ProtozoaKate Alyssa CatonNo ratings yet
- Introduction To Nematodes: College of Medical Laboratory Science Our Lady of Fatima University-ValenzuelaDocument29 pagesIntroduction To Nematodes: College of Medical Laboratory Science Our Lady of Fatima University-ValenzuelaMich100% (1)
- Parasitology - MTAPDocument278 pagesParasitology - MTAPMarron MonsaludNo ratings yet
- Entamoeba Histolytica: Causes: Amoebiasis. Geog - Distribution: Habitat: Infective Stage: Mode of InfectionDocument46 pagesEntamoeba Histolytica: Causes: Amoebiasis. Geog - Distribution: Habitat: Infective Stage: Mode of InfectionAlfia Nikmah100% (3)
- Clinical Chemistry Notes - ABIDocument32 pagesClinical Chemistry Notes - ABIAnya Ignacio100% (1)
- Parasitology: Basic Terminologies Major Groups of Medically Important ParasitesDocument4 pagesParasitology: Basic Terminologies Major Groups of Medically Important ParasitesHannah Grace CorveraNo ratings yet
- An Ocean Without ShoreDocument199 pagesAn Ocean Without ShoreBogdan Scupra50% (2)
- Parasites of Medical ImportanceDocument9 pagesParasites of Medical ImportanceKimberly RampersadNo ratings yet
- At Sea (Return of The Woodland Warriors)Document23 pagesAt Sea (Return of The Woodland Warriors)Tess MercerNo ratings yet
- Parasitology-Lec 10 EntamoebaDocument7 pagesParasitology-Lec 10 Entamoebaapi-3743217100% (2)
- Enzymology Part 1-2Document12 pagesEnzymology Part 1-2Anya IgnacioNo ratings yet
- Lunar Code Final LayoutDocument208 pagesLunar Code Final LayoutPhillip LambertNo ratings yet
- Yog Mimnsha PDFDocument6 pagesYog Mimnsha PDFrahul guptaNo ratings yet
- Clinical Chemistry Notes (Blanked) - ABI PDFDocument34 pagesClinical Chemistry Notes (Blanked) - ABI PDFAnya IgnacioNo ratings yet
- 125.052 - Travel Wide v. CA (1991) - DigestDocument4 pages125.052 - Travel Wide v. CA (1991) - DigestJames LouNo ratings yet
- Parasitology Table ProtozoaDocument10 pagesParasitology Table ProtozoaMae Rose Charlene MendozaNo ratings yet
- PROTOZOA (Sarcodina) : ProtozoologyDocument7 pagesPROTOZOA (Sarcodina) : ProtozoologyReyven Niña DyNo ratings yet
- Parasitic AmoebaDocument23 pagesParasitic AmoebaJethrö MallariNo ratings yet
- Gear 1Document9 pagesGear 1Ariyant CreativeNo ratings yet
- Clinical Chemistry Notes - AbiDocument34 pagesClinical Chemistry Notes - AbiAnya Ignacio100% (1)
- (PROTOZOANS) Phylum ApicomplexaDocument8 pages(PROTOZOANS) Phylum ApicomplexaEunice AndradeNo ratings yet
- G.R. No. 159926 January 20, 2014 Pinausukan Seafood House, Roxas Bouley Ard, Inc.Document65 pagesG.R. No. 159926 January 20, 2014 Pinausukan Seafood House, Roxas Bouley Ard, Inc.johnkyleNo ratings yet
- Emerging & Remerging Parasitic DiseasesDocument27 pagesEmerging & Remerging Parasitic DiseasesNeha SamalNo ratings yet
- 3.b.coli, Crypt, Cyclo, Iso, Sarco, Microsp, Acnth, NaegDocument86 pages3.b.coli, Crypt, Cyclo, Iso, Sarco, Microsp, Acnth, NaegPallavi Uday NaikNo ratings yet
- Parasitology: Basic TerminologiesDocument4 pagesParasitology: Basic TerminologiesHannah Grace CorveraNo ratings yet
- Isospora BelliDocument16 pagesIsospora BelliMary Christelle100% (1)
- 4-Intestinal ProtozoaDocument21 pages4-Intestinal ProtozoaHumera JabeenNo ratings yet
- Parasitos Oportunistas: Catalina Tovar Acero Msc. Infecciones Y Salud en El TropicalDocument22 pagesParasitos Oportunistas: Catalina Tovar Acero Msc. Infecciones Y Salud en El TropicalAndrés ArrietaNo ratings yet
- Opportunistic InfectionDocument8 pagesOpportunistic InfectionlhoshinyNo ratings yet
- MBP Lab ReviewerDocument9 pagesMBP Lab ReviewerTrisha PaolaNo ratings yet
- Intestinal FlagellatesDocument5 pagesIntestinal Flagellatesdhainey100% (3)
- SPOROZOANS Excluding PlasmodiumDocument28 pagesSPOROZOANS Excluding PlasmodiumdiamantechennieNo ratings yet
- PARA CompilationDocument22 pagesPARA CompilationMica BernardoNo ratings yet
- E. Histolytica: Associated DiseasesDocument11 pagesE. Histolytica: Associated DiseasesCorinne MandrezaNo ratings yet
- 2021 Parasitology Lab CoccidiansDocument55 pages2021 Parasitology Lab CoccidiansPhilip Patrick LeeNo ratings yet
- 2021 - l4 Medical Bacteriology - Gram Negative Bacteria (I)Document52 pages2021 - l4 Medical Bacteriology - Gram Negative Bacteria (I)Tonny YuliantoNo ratings yet
- 2.14 - Trematodes and CestodesDocument5 pages2.14 - Trematodes and CestodesLunaNo ratings yet
- Lecture I 2022Document24 pagesLecture I 2022Adam DiabNo ratings yet
- Lecture I 2022Document24 pagesLecture I 2022Adam DiabNo ratings yet
- Screenshot 2024-02-28 at 9.47.36 AMDocument36 pagesScreenshot 2024-02-28 at 9.47.36 AMfftemmmNo ratings yet
- Int CoccidDocument43 pagesInt Coccidhanan.mahmoud272246No ratings yet
- ProtozoaDocument28 pagesProtozoaFRANCESCA ALEXANDRIA PAREDESNo ratings yet
- Summary of Cyclospora CayetanensisDocument2 pagesSummary of Cyclospora CayetanensisGearvell NapatNo ratings yet
- Coccidia SummaryDocument2 pagesCoccidia SummaryNibshian Dela RosaNo ratings yet
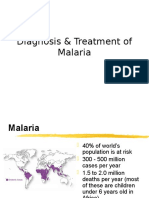
- Diagnosis & Treatment of MalariaDocument67 pagesDiagnosis & Treatment of MalariaINDRINo ratings yet
- Other ProtozoansDocument5 pagesOther ProtozoansChristine BuenNo ratings yet
- Giardia LambliaDocument28 pagesGiardia LambliaMegbaruNo ratings yet
- Parasites by Apple TanDocument16 pagesParasites by Apple TanOlivia LimNo ratings yet
- Parasitology: Victor Babes University of Medicine and Pharmacy Timisoara Discipline of ParasitologyDocument72 pagesParasitology: Victor Babes University of Medicine and Pharmacy Timisoara Discipline of ParasitologyanaNo ratings yet
- CoccidiaDocument42 pagesCoccidiawadige4668No ratings yet
- Miscellaneous Protozoa1Document5 pagesMiscellaneous Protozoa1Haki TozakiNo ratings yet
- Parasite InfectionsDocument45 pagesParasite InfectionsAbdullah AlkharsNo ratings yet
- Presentation 1Document57 pagesPresentation 1amrita goyalNo ratings yet
- Protozoa: DR Mohieddīn M Abdul FattahDocument95 pagesProtozoa: DR Mohieddīn M Abdul FattahMicroscopeGeekNo ratings yet
- Isospora Belli Summary OutlineDocument3 pagesIsospora Belli Summary OutlineGearvell NapatNo ratings yet
- COCCIDIANSDocument10 pagesCOCCIDIANSirishgopez24No ratings yet
- 4.1 Pathogenic FlagellatesDocument63 pages4.1 Pathogenic Flagellateskaartikey dubeNo ratings yet
- AmoebaDocument4 pagesAmoebaRichell VillacarlosNo ratings yet
- BACTERIOLOGYDocument9 pagesBACTERIOLOGYJe GregorioNo ratings yet
- Lecture 06Document35 pagesLecture 06Lib PalmaresNo ratings yet
- Lec 12 Apicomplexa 2Document30 pagesLec 12 Apicomplexa 2Ram RamNo ratings yet
- L3 - Enterobactericiae SPPDocument23 pagesL3 - Enterobactericiae SPPbujalkanNo ratings yet
- Other Human Sporozoal InfectionsDocument44 pagesOther Human Sporozoal Infectionsaditya.3757No ratings yet
- Amoeba Notes 2015Document6 pagesAmoeba Notes 2015Ivy FlorentinoNo ratings yet
- ProtistaDocument4 pagesProtistaBounce AtomNo ratings yet
- Paralec M1Document8 pagesParalec M1VE NI CENo ratings yet
- Protista (Subdivision Protozoa) : Bütschlii), or Pathogenic (E. Histolytica)Document6 pagesProtista (Subdivision Protozoa) : Bütschlii), or Pathogenic (E. Histolytica)Primo GeorgeNo ratings yet
- Ascaris Lumbricoides (Linneaus. 1758) : NEMATODES: IntestinalDocument21 pagesAscaris Lumbricoides (Linneaus. 1758) : NEMATODES: IntestinalPatricia CabisonNo ratings yet
- Deteksi Infeksi Penyakit Menular - Parasit - SalinDocument73 pagesDeteksi Infeksi Penyakit Menular - Parasit - SalinnurlailiNo ratings yet
- A Complete Note On Parasitology For 2nd PDFDocument105 pagesA Complete Note On Parasitology For 2nd PDFMahi SinghNo ratings yet
- Enzyme: Specific Proteins That Catalyze Biochemical: Constituents of Enzyme MoleculeDocument6 pagesEnzyme: Specific Proteins That Catalyze Biochemical: Constituents of Enzyme MoleculeAnya IgnacioNo ratings yet
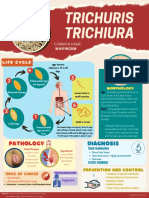
- Trichuris TrichiuraDocument1 pageTrichuris TrichiuraAnya IgnacioNo ratings yet
- Purine Disorder PDFDocument1 pagePurine Disorder PDFAnya IgnacioNo ratings yet
- Lesson 5 Plasmodium SPPDocument8 pagesLesson 5 Plasmodium SPPAnya IgnacioNo ratings yet
- Lesson 8 - Nematodes IDocument7 pagesLesson 8 - Nematodes IAnya IgnacioNo ratings yet
- Quality Assessment, Renal Disease & Urine ScreeningDocument15 pagesQuality Assessment, Renal Disease & Urine ScreeningAnya IgnacioNo ratings yet
- Endocrine System: EndocrinologyDocument10 pagesEndocrine System: EndocrinologyAnya IgnacioNo ratings yet
- Fixation NotesDocument35 pagesFixation NotesAnya IgnacioNo ratings yet
- Characteristics of Virus: Characteristic of Cellular LifeDocument6 pagesCharacteristics of Virus: Characteristic of Cellular LifeAnya IgnacioNo ratings yet
- Lesson 5 - PlasmodiumDocument9 pagesLesson 5 - PlasmodiumAnya IgnacioNo ratings yet
- Myxoviruses: MIDTERM LESSON 2: Respiratory VirusesDocument8 pagesMyxoviruses: MIDTERM LESSON 2: Respiratory VirusesAnya IgnacioNo ratings yet
- AUBF Microscopic Exam Part 2&3Document13 pagesAUBF Microscopic Exam Part 2&3Anya IgnacioNo ratings yet
- Nef Upper Filetest 02 Answerkey PDFDocument6 pagesNef Upper Filetest 02 Answerkey PDFCoralza SacNo ratings yet
- Lecture Notes Legal Ethics Part 2Document4 pagesLecture Notes Legal Ethics Part 2Ric TanNo ratings yet
- Students Innovation Festival Space HackathonDocument6 pagesStudents Innovation Festival Space HackathonAsad ShadNo ratings yet
- Earthquake-Induced Settlement: The Following Notation Is Used in This ChapterDocument27 pagesEarthquake-Induced Settlement: The Following Notation Is Used in This ChapternktanakaNo ratings yet
- NPI2Document4 pagesNPI2Jerome AsuncionNo ratings yet
- MURLIDocument4 pagesMURLIrabinpadhanNo ratings yet
- Immersion I Lesson Plan Anti Bias Revised With EvaluationDocument14 pagesImmersion I Lesson Plan Anti Bias Revised With Evaluationapi-334310370No ratings yet
- Undercurrent Worlds 100 Largest Seafood Companies 2014Document293 pagesUndercurrent Worlds 100 Largest Seafood Companies 2014Nelson ArmasNo ratings yet
- Employee Motivation and PerformanceDocument6 pagesEmployee Motivation and PerformanceOradea ToastmastersNo ratings yet
- Quotation 2Document1 pageQuotation 2rahulsoodplpNo ratings yet
- PDF To WordDocument43 pagesPDF To WordKamrul HasanNo ratings yet
- Ca Celin Carretela Arrived Bringing Inside My Brother and Her WifeDocument2 pagesCa Celin Carretela Arrived Bringing Inside My Brother and Her WifeYjasmin AnneNo ratings yet
- The Earth in The Solar System: Globe: Latitudes and LongitudesDocument10 pagesThe Earth in The Solar System: Globe: Latitudes and LongitudesPranit PrasoonNo ratings yet
- Inverter Outdoor Unit: For Air Source Split Heat Pump Air To Water and Air To Air 2 To 16 KW Output Heating and CoolingDocument3 pagesInverter Outdoor Unit: For Air Source Split Heat Pump Air To Water and Air To Air 2 To 16 KW Output Heating and CoolingVlad PandichiNo ratings yet
- Tariff Booklet: October 2021Document16 pagesTariff Booklet: October 2021Anonymous ameerNo ratings yet
- DCMMMNHS - Work Immersion Proper and Post ImmersionDocument3 pagesDCMMMNHS - Work Immersion Proper and Post ImmersionTresita B. RiosNo ratings yet
- Dolphin Station - Pre App Letter of IntentDocument3 pagesDolphin Station - Pre App Letter of Intentthe next miamiNo ratings yet
- Moraga, Cherrie La GueraDocument5 pagesMoraga, Cherrie La GueranizaiaNo ratings yet
- DocuCentre S2520 S2320Document4 pagesDocuCentre S2520 S2320nuwari fadliNo ratings yet
- Zoya Parasher - 2152916 - Big DataDocument6 pagesZoya Parasher - 2152916 - Big DataZoya ParasherNo ratings yet
- Workshop Unit 3 1 LevelsDocument6 pagesWorkshop Unit 3 1 LevelsFrancisco Camilo Hernandez MurgaNo ratings yet
- Qulalys Sample ReportDocument6 pagesQulalys Sample Reporteagleboy007No ratings yet
- Introduction To Earthquake Resistant Design..Earthquake and Urbanization - History of Major International and Philippine Earthquake. The Ring of FireDocument19 pagesIntroduction To Earthquake Resistant Design..Earthquake and Urbanization - History of Major International and Philippine Earthquake. The Ring of FireJeffry VargasNo ratings yet