You might also like
- Psoriasis Lecture Notes 2015Document17 pagesPsoriasis Lecture Notes 2015SaulNo ratings yet
- Psoriasis - StatPearls - NCBI BookshelfDocument8 pagesPsoriasis - StatPearls - NCBI BookshelfMehmet TaşçıNo ratings yet
- White Scaly Papules and Plaques On His Elbows, Extensor Arms, Knees, and ShinsDocument54 pagesWhite Scaly Papules and Plaques On His Elbows, Extensor Arms, Knees, and ShinsJohn Christopher LucesNo ratings yet
- Kuliah 4 B - PSORIASISDocument30 pagesKuliah 4 B - PSORIASISTimothy TobiasNo ratings yet
- Pityriasis RoseaDocument20 pagesPityriasis RoseaMendy Herianto100% (1)
- PsoriasisDocument57 pagesPsoriasisapi-19916399100% (1)
- How To Cure PsoriasisDocument7 pagesHow To Cure Psoriasispallavsharma1987No ratings yet
- PSORIASISDocument27 pagesPSORIASISnurulzakinahnunu100% (1)
- Psoriasis: Psoriasis Is A Common, Chronic, Relapsing/remitting, Immune-Mediated Systemic DiseaseDocument16 pagesPsoriasis: Psoriasis Is A Common, Chronic, Relapsing/remitting, Immune-Mediated Systemic DiseaseSaitejaKachamNo ratings yet
- Case Report - PsoriasisDocument7 pagesCase Report - Psoriasisnathalia gabriellaNo ratings yet
- Kuliah 4 A - EritropapuloskuamousDocument46 pagesKuliah 4 A - EritropapuloskuamousTimothy TobiasNo ratings yet
- Psoriasis 1Document32 pagesPsoriasis 1SabaniaresmenNo ratings yet
- Referat Kulit KakayDocument26 pagesReferat Kulit KakayRezky Dwiputra FellanysNo ratings yet
- Mikimos,+09 +lisi 56 60Document5 pagesMikimos,+09 +lisi 56 60MaylafaizaNo ratings yet
- PsoriasisDocument30 pagesPsoriasisSaputra Tri NopiantoNo ratings yet
- Psoriasis: Psoriasis Type of PsoriasisDocument18 pagesPsoriasis: Psoriasis Type of PsoriasisDeepikaNo ratings yet
- Physical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsDocument12 pagesPhysical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsNaomi AnastacioNo ratings yet
- PsoriasisDocument7 pagesPsoriasisdhavalNo ratings yet
- Y3 Immunologic DsesDocument65 pagesY3 Immunologic DsesJess PeltraNo ratings yet
- PsoriasisDocument27 pagesPsoriasisMala PotterNo ratings yet
- PsoriasisDocument32 pagesPsoriasisChirag VijayvargiyaNo ratings yet
- Dermatology D. Azr Lec2 Mon 18.10.2010: Papulosquamous DiseasesDocument9 pagesDermatology D. Azr Lec2 Mon 18.10.2010: Papulosquamous DiseasesMohamed Al-zichrawyNo ratings yet
- PsoriasisDocument33 pagesPsoriasisPratzNo ratings yet
- Psoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsDocument21 pagesPsoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsMapsNo ratings yet
- Psoriasis: ClassificationDocument10 pagesPsoriasis: ClassificationRaluk OnytzaNo ratings yet
- Speaker NotesDocument21 pagesSpeaker Noteschinnupepsi4allNo ratings yet
- Papulosquamous Diseases PDFDocument15 pagesPapulosquamous Diseases PDFJames Ajak AgothNo ratings yet
- Plaque Psoriasis: Understanding Risk Factors of This Inflammatory Skin PathologyDocument14 pagesPlaque Psoriasis: Understanding Risk Factors of This Inflammatory Skin PathologyOktavianti Prisilia SoumokilNo ratings yet
- Pustular Psoriasis Sep 20Document8 pagesPustular Psoriasis Sep 20RemNo ratings yet
- 5 Psoriasis PDFDocument76 pages5 Psoriasis PDFWorku KifleNo ratings yet
- Faculty of Medicine: Kafr El-Sheikh UniversityDocument11 pagesFaculty of Medicine: Kafr El-Sheikh UniversityjayNo ratings yet
- Griffiths2007 PDFDocument9 pagesGriffiths2007 PDFFirah Triple'sNo ratings yet
- PsoriasisDocument27 pagesPsoriasisMASCULINE DEACONNo ratings yet
- Systemic and Localized Scleroderm11!05!08Document99 pagesSystemic and Localized Scleroderm11!05!08Linux LinuxNo ratings yet
- PsoriasisDocument61 pagesPsoriasisWilliam WongNo ratings yet
- Dermatology OSCE Pictures 1Document208 pagesDermatology OSCE Pictures 1medt80No ratings yet
- Psoriasis - FINALDocument33 pagesPsoriasis - FINALbrian mburuNo ratings yet
- Psoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsDocument21 pagesPsoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsOktavianti Prisilia SoumokilNo ratings yet
- Presented By:Cherry Ann Del Pilar Iviu Staff NurseDocument15 pagesPresented By:Cherry Ann Del Pilar Iviu Staff Nursephp_czarina04421No ratings yet
- Scleroderma PDFDocument9 pagesScleroderma PDFAustine OsaweNo ratings yet
- Papulosquamous Diseases (Andrew's Dermatology)Document10 pagesPapulosquamous Diseases (Andrew's Dermatology)Xanthia CristobalNo ratings yet
- Fever and Rash: Alvin Germo PasuquinDocument70 pagesFever and Rash: Alvin Germo PasuquinAlvin Germo PasuquinNo ratings yet
- Psoriasis: Risk FactorsDocument9 pagesPsoriasis: Risk FactorsJohn Michael TaylanNo ratings yet
- Eritro Papulo Skuamosa 2021Document47 pagesEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- PENDAHULUAN - EfloresensiDocument50 pagesPENDAHULUAN - EfloresensiSucitri NyomanNo ratings yet
- PsoriasisDocument27 pagesPsoriasisMishaNo ratings yet
- Psoriasis (: /SƏ Raɪ - Əsɨs/ Autoimmune DiseaseDocument23 pagesPsoriasis (: /SƏ Raɪ - Əsɨs/ Autoimmune DiseaseMichael CoronadoNo ratings yet
- CarbuncleDocument28 pagesCarbunclemimie23No ratings yet
- ErythrodermaDocument48 pagesErythrodermaShwan OmarNo ratings yet
- Presentation 1Document57 pagesPresentation 1Brian BeeNo ratings yet
- PATHOPHYS - DermatologyDocument19 pagesPATHOPHYS - Dermatologyaagioaa100% (1)
- PsoriasisDocument5 pagesPsoriasismuhammadridhwanNo ratings yet
- Psoriasis: PathophysiologyDocument23 pagesPsoriasis: PathophysiologyImran KhanNo ratings yet
- Therapeutics 4th YrDocument26 pagesTherapeutics 4th YrpragnaNo ratings yet
- Ayurvedic Management of Psoriasis (Ek Kustha) - A Case StudyDocument8 pagesAyurvedic Management of Psoriasis (Ek Kustha) - A Case Studybhavana NandakumarNo ratings yet
- Rash BookDocument12 pagesRash BookPhoebe UsmleNo ratings yet
- 2.papulosquamous DiseasesDocument65 pages2.papulosquamous DiseasesThesa TagalogNo ratings yet
- Psoriasis: For Health Officer Students Solomon H (MD, DVR)Document38 pagesPsoriasis: For Health Officer Students Solomon H (MD, DVR)Theo Grazila RuvaNo ratings yet
- Bacterial Genetics: DR - Tetty Aman Nasution M Med SCDocument54 pagesBacterial Genetics: DR - Tetty Aman Nasution M Med SCRemigius RiyanNo ratings yet
- SFT Lhfa Girls Z 0 2 PDFDocument1 pageSFT Lhfa Girls Z 0 2 PDFVictor BaezaNo ratings yet
- Pertussis in Children Problems in Indonesia 2165 7548 1000377 PDFDocument6 pagesPertussis in Children Problems in Indonesia 2165 7548 1000377 PDFRemigius RiyanNo ratings yet
- Fungi: Therapy of Skin, Hair and Nail Fungal InfectionsDocument13 pagesFungi: Therapy of Skin, Hair and Nail Fungal InfectionsAghnia NafilaNo ratings yet
- BBS2 MB-K11-tambahan-FDA Investigated Listeria Monocytogenes Illnesses Linked To Caramel ApplesDocument7 pagesBBS2 MB-K11-tambahan-FDA Investigated Listeria Monocytogenes Illnesses Linked To Caramel ApplesRemigius RiyanNo ratings yet
- IKD2-K11 - Mikosis Superfisialis, Mikosis Sistemik Dan Mikosis OportunistikDocument64 pagesIKD2-K11 - Mikosis Superfisialis, Mikosis Sistemik Dan Mikosis OportunistikHalseyNo ratings yet
- AHA Hypertension Guidelines 2017Document22 pagesAHA Hypertension Guidelines 2017Anonymous elSqPhzKNo ratings yet
- Nutrition 2 1046 PDFDocument5 pagesNutrition 2 1046 PDFRemigius RiyanNo ratings yet
- Radiology - Letter Warning of CT False Negative Rate in COVID-YangDocument3 pagesRadiology - Letter Warning of CT False Negative Rate in COVID-YangRemigius RiyanNo ratings yet
- Epilepsy q2Document23 pagesEpilepsy q2lugosor20No ratings yet
- Bone AgeDocument13 pagesBone Ageadrian revoNo ratings yet
- SFT Lhfa Girls Z 0 2 PDFDocument1 pageSFT Lhfa Girls Z 0 2 PDFVictor BaezaNo ratings yet
- The Effects of Betahistine and Dimenhydrinate On Caloric Test Parameters Slow-Phase Velocity of NystagmusDocument4 pagesThe Effects of Betahistine and Dimenhydrinate On Caloric Test Parameters Slow-Phase Velocity of NystagmusRemigius RiyanNo ratings yet
- Myasthenia Gravis: MG-epidemiologyDocument3 pagesMyasthenia Gravis: MG-epidemiologyRemigius RiyanNo ratings yet
- CHT Lfa Boys Z 0 2Document1 pageCHT Lfa Boys Z 0 2Indra NasutionNo ratings yet
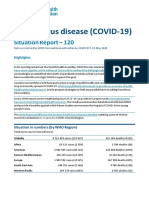
- Coronavirus Disease (COVID-19) : Situation Report - 120Document16 pagesCoronavirus Disease (COVID-19) : Situation Report - 120CityNewsTorontoNo ratings yet
- Management of Oral Leukoplakia - Analysis of The Literature: Material and MethodsDocument10 pagesManagement of Oral Leukoplakia - Analysis of The Literature: Material and MethodsyunisaNo ratings yet
- 40 5 643 PDFDocument12 pages40 5 643 PDFRemigius RiyanNo ratings yet
- JJM 08 03 21760Document5 pagesJJM 08 03 21760Remigius RiyanNo ratings yet
- ILAE Clasiffication and Teminology 2017Document10 pagesILAE Clasiffication and Teminology 2017Prabaningrum DwidjoasmoroNo ratings yet
- Microtronics Technologies: GSM Based Vehicle Theft Detection SystemDocument3 pagesMicrotronics Technologies: GSM Based Vehicle Theft Detection Systemابراهيم الثوبريNo ratings yet
- Kompilasi Soal Paket BDocument10 pagesKompilasi Soal Paket Babdul wahidNo ratings yet
- PLC Anupam Samanta 2010JE0976Document64 pagesPLC Anupam Samanta 2010JE0976Anupam SamantaNo ratings yet
- 46GA On Designers For CEED, UCEED and NID - Stuff You LookDocument3 pages46GA On Designers For CEED, UCEED and NID - Stuff You LookReshmi Varma100% (1)
- 02 RgebDocument1,168 pages02 Rgebprožnik100% (3)
- INST240 Sec4Document127 pagesINST240 Sec4bhanu6212No ratings yet
- 66 Essential Phrasal Verbs EnglishDocument6 pages66 Essential Phrasal Verbs EnglishNarcisVega100% (15)
- CV KM Roy Supit 01 April 2019Document3 pagesCV KM Roy Supit 01 April 2019Ephanama TehnikNo ratings yet
- Abu Quir Iii Start Up PDFDocument18 pagesAbu Quir Iii Start Up PDFAnonymous 1XHScfCI100% (1)
- Quintin Kynaston School Wikipedia.Document3 pagesQuintin Kynaston School Wikipedia.John_Adam_St_Gang_QKNo ratings yet
- CRC Ace Far 1ST PBDocument9 pagesCRC Ace Far 1ST PBJohn Philip Castro100% (1)
- EtamolDocument5 pagesEtamolthonyyanmuNo ratings yet
- Levers of Control Analysis of Management Control SDocument17 pagesLevers of Control Analysis of Management Control SApriana RahmawatiNo ratings yet
- DLP1Document6 pagesDLP1Ben Joseph CapistranoNo ratings yet
- z01 PDFDocument12 pagesz01 PDFZdravko RusevNo ratings yet
- Inter 10 - Third ClassDocument96 pagesInter 10 - Third ClassRicardo Jackichan Barzola LopezNo ratings yet
- Last Voyage of Somebody The Sailor The SailorDocument581 pagesLast Voyage of Somebody The Sailor The SailorDelia Ungureanu50% (2)
- Yogesh Kadam (ABC)Document5 pagesYogesh Kadam (ABC)vipin HNo ratings yet
- Cyber CXDocument2 pagesCyber CXhplzNo ratings yet
- Vat Reg. CertificateDocument1 pageVat Reg. CertificateMaaz AzadNo ratings yet
- Giki Students Hand Book 08Document75 pagesGiki Students Hand Book 08Jawad Rasheed Sheikh100% (1)
- Rexroth 4we10 Data Sheet PDFDocument10 pagesRexroth 4we10 Data Sheet PDFSIVARAMANJAGANATHANNo ratings yet
- AP Physics 1 Practice Test 2 Answer ExplanationsDocument14 pagesAP Physics 1 Practice Test 2 Answer Explanations장준오No ratings yet
- A New Approach To Air Quality in Hospitals: Www.p3italy - ItDocument19 pagesA New Approach To Air Quality in Hospitals: Www.p3italy - ItMuneer Ahmed ShaikNo ratings yet
- Cutlist Cistern TankDocument10 pagesCutlist Cistern TankAilyn O. DungogNo ratings yet
- Business Studies Project 1Document16 pagesBusiness Studies Project 1MANOJ CHAVANNo ratings yet
- Turkey GO (896-22)Document1 pageTurkey GO (896-22)shrabon001No ratings yet
- RCB Dealers PHDocument3 pagesRCB Dealers PHJing AbionNo ratings yet
- Test Method of Flammability of Interior Materials For AutomobilesDocument17 pagesTest Method of Flammability of Interior Materials For AutomobilesKarthic BhrabuNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (79)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (21)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)