You might also like
- Physical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsDocument12 pagesPhysical Trauma (Koebner's Phenomenon) Is A Major Factor in Eliciting LesionsNaomi AnastacioNo ratings yet
- 5 Psoriasis PDFDocument76 pages5 Psoriasis PDFWorku KifleNo ratings yet
- Y3 Immunologic DsesDocument65 pagesY3 Immunologic DsesJess PeltraNo ratings yet
- PsoriasisDocument61 pagesPsoriasisWilliam WongNo ratings yet
- White Scaly Papules and Plaques On His Elbows, Extensor Arms, Knees, and ShinsDocument54 pagesWhite Scaly Papules and Plaques On His Elbows, Extensor Arms, Knees, and ShinsJohn Christopher LucesNo ratings yet
- Psoriasis: Psoriasis Type of PsoriasisDocument18 pagesPsoriasis: Psoriasis Type of PsoriasisDeepikaNo ratings yet
- A Brief Summary of Clinical Types of Psoriasis: Invited ReviewDocument4 pagesA Brief Summary of Clinical Types of Psoriasis: Invited ReviewRemigius RiyanNo ratings yet
- PsoriasisDocument33 pagesPsoriasisPratzNo ratings yet
- Psoriasis Case Report on 33-Year-Old MaleDocument7 pagesPsoriasis Case Report on 33-Year-Old Malenathalia gabriellaNo ratings yet
- Dermatology D. Azr Lec2 Mon 18.10.2010: Papulosquamous DiseasesDocument9 pagesDermatology D. Azr Lec2 Mon 18.10.2010: Papulosquamous DiseasesMohamed Al-zichrawyNo ratings yet
- Kuliah 4 A - EritropapuloskuamousDocument46 pagesKuliah 4 A - EritropapuloskuamousTimothy TobiasNo ratings yet
- PsoriasisDocument32 pagesPsoriasisChirag VijayvargiyaNo ratings yet
- Psoriasis: PathophysiologyDocument23 pagesPsoriasis: PathophysiologyImran KhanNo ratings yet
- Papulosquamous Diseases (Andrew's Dermatology)Document10 pagesPapulosquamous Diseases (Andrew's Dermatology)Xanthia CristobalNo ratings yet
- PSORIASIS: AN IMMUNE-MEDIATED SKIN DISEASEDocument10 pagesPSORIASIS: AN IMMUNE-MEDIATED SKIN DISEASERaluk OnytzaNo ratings yet
- Kafr El-Sheikh University: PsoriasisDocument11 pagesKafr El-Sheikh University: PsoriasisjayNo ratings yet
- Kuliah 4 B - PSORIASISDocument30 pagesKuliah 4 B - PSORIASISTimothy TobiasNo ratings yet
- PSORIASISDocument27 pagesPSORIASISnurulzakinahnunu100% (1)
- Psoriasis: For Health Officer Students Solomon H (MD, DVR)Document38 pagesPsoriasis: For Health Officer Students Solomon H (MD, DVR)Theo Grazila RuvaNo ratings yet
- Psoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsDocument21 pagesPsoriasis: Epidemiology, Clinical and Histological Features, Triggering Factors, Assessment of Severity and Psychosocial AspectsMapsNo ratings yet
- 2.papulosquamous DiseasesDocument65 pages2.papulosquamous DiseasesThesa TagalogNo ratings yet
- PsoriasisDocument27 pagesPsoriasisMASCULINE DEACONNo ratings yet
- Psoriasis 1Document32 pagesPsoriasis 1SabaniaresmenNo ratings yet
- Pityriasis RoseaDocument20 pagesPityriasis RoseaMendy Herianto100% (1)
- Psoriasis - FINALDocument33 pagesPsoriasis - FINALbrian mburuNo ratings yet
- Psoriasis: Risk FactorsDocument9 pagesPsoriasis: Risk FactorsJohn Michael TaylanNo ratings yet
- Therapeutics 4th YrDocument26 pagesTherapeutics 4th YrpragnaNo ratings yet
- Diagnosis and Management of Psoriasis: Clinical ReviewDocument9 pagesDiagnosis and Management of Psoriasis: Clinical Reviewirvan halimNo ratings yet
- PSORIASIS: AN IMMUNE MEDIATED SKIN DISEASEDocument15 pagesPSORIASIS: AN IMMUNE MEDIATED SKIN DISEASEphp_czarina04421No ratings yet
- Presentation 1Document57 pagesPresentation 1Brian BeeNo ratings yet
- Psoriasis - StatPearls - NCBI BookshelfDocument8 pagesPsoriasis - StatPearls - NCBI BookshelfMehmet TaşçıNo ratings yet
- Psoriasis: Key PointsDocument11 pagesPsoriasis: Key Pointsazucena rocio de la roca gonzalezNo ratings yet
- Cutaneous Manifestation of Systemic DisordersDocument31 pagesCutaneous Manifestation of Systemic DisordersPratzNo ratings yet
- Biological Treatment in PsoriasisDocument10 pagesBiological Treatment in PsoriasisHassanNo ratings yet
- Papulosquamous DisordersDocument51 pagesPapulosquamous DisordersleenaloveuNo ratings yet
- How To Cure PsoriasisDocument7 pagesHow To Cure Psoriasispallavsharma1987No ratings yet
- Skin Patterns and Clinical Presentations of PsoriasisDocument30 pagesSkin Patterns and Clinical Presentations of PsoriasisSaputra Tri NopiantoNo ratings yet
- PsoriasisDocument27 pagesPsoriasisMala PotterNo ratings yet
- PsoriasisDocument32 pagesPsoriasisEffah FestusNo ratings yet
- Huangshi Center Hospital - Zheng Qi: Erythema Scaly DermatosisDocument139 pagesHuangshi Center Hospital - Zheng Qi: Erythema Scaly DermatosisAmeliaNo ratings yet
- Papulosquamous Ds.Document70 pagesPapulosquamous Ds.CHALIE MEQUNo ratings yet
- Acute and Chronic Dermatosis ..Document28 pagesAcute and Chronic Dermatosis ..mohammed alrubaiaanNo ratings yet
- PsoriasisDocument23 pagesPsoriasisvasavavipul38022No ratings yet
- Eritro Papulo Skuamosa 2021Document47 pagesEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- Eritropapuloskuamosa Kuliah NewDocument52 pagesEritropapuloskuamosa Kuliah NewpipitNo ratings yet
- Dermatitis Numularis and NeurodermatitisDocument22 pagesDermatitis Numularis and NeurodermatitisNura ReefaNo ratings yet
- Skin Block: - Introduction To Diseases of The Skin - Acneiform, Alopecias, and Pigmentary DisordersDocument60 pagesSkin Block: - Introduction To Diseases of The Skin - Acneiform, Alopecias, and Pigmentary DisordershemihemaNo ratings yet
- Rash BookDocument12 pagesRash BookPhoebe UsmleNo ratings yet
- Reactive Inflammatory ErythemasDocument71 pagesReactive Inflammatory ErythemasYasir Saleem KhanNo ratings yet
- Askep Psoriasis: Bab I PendahuluanDocument64 pagesAskep Psoriasis: Bab I PendahuluanMoh Syukrin LamukeNo ratings yet
- Psoriasis: Psoriasis Is A Common, Chronic, Relapsing/remitting, Immune-Mediated Systemic DiseaseDocument16 pagesPsoriasis: Psoriasis Is A Common, Chronic, Relapsing/remitting, Immune-Mediated Systemic DiseaseSaitejaKachamNo ratings yet
- Psoriasis: A Systematic Review of Autoimmune DisorderDocument8 pagesPsoriasis: A Systematic Review of Autoimmune DisorderInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- NEURODERMATITIS: Understanding Lichen Simplex ChronicusDocument3 pagesNEURODERMATITIS: Understanding Lichen Simplex ChronicusAdeliaNo ratings yet
- PsoriasisDocument7 pagesPsoriasisdhavalNo ratings yet
- Referat Kulit KakayDocument26 pagesReferat Kulit KakayRezky Dwiputra FellanysNo ratings yet
- PsoriasisDocument29 pagesPsoriasisProtantagonist100% (1)
- Fitzpatrick Lecture: Katrina D. Olitoquit, MDDocument94 pagesFitzpatrick Lecture: Katrina D. Olitoquit, MDJonnie Rose Louise WeeNo ratings yet
- Psoriasis: Common DermatosesDocument7 pagesPsoriasis: Common DermatoseslaluneNo ratings yet
- Antiarrhythmic Drugs: Mechanisms, Effects & UsesDocument6 pagesAntiarrhythmic Drugs: Mechanisms, Effects & UsesSaulNo ratings yet
- IV. Antiarrhythmic Drugs: PHRM 537 Summer 2020Document19 pagesIV. Antiarrhythmic Drugs: PHRM 537 Summer 2020SaulNo ratings yet
- Case16 Part2Document1 pageCase16 Part2SaulNo ratings yet
- Pediatric Pinworm: Treatment & Education"TITLE"Adult Pinworm: Assessment & ManagementDocument3 pagesPediatric Pinworm: Treatment & Education"TITLE"Adult Pinworm: Assessment & ManagementSaul0% (1)
- Antiarrhythmic Drugs: Mechanisms, Effects & UsesDocument6 pagesAntiarrhythmic Drugs: Mechanisms, Effects & UsesSaulNo ratings yet
- Segment Anafranil MedGuide PDFDocument2 pagesSegment Anafranil MedGuide PDFSaulNo ratings yet
- Ninja - Antiarrhythmic Drugs PDFDocument7 pagesNinja - Antiarrhythmic Drugs PDFErica Hyeyeon Lee100% (1)
- Lange Smart Charts: Pharmacology, 2e Medications Affecting Cardiac and Renal FunctionDocument2 pagesLange Smart Charts: Pharmacology, 2e Medications Affecting Cardiac and Renal FunctionSaulNo ratings yet
- Anti Arrythmic and Antianginal Drugs PDFDocument24 pagesAnti Arrythmic and Antianginal Drugs PDFSaulNo ratings yet
- Drug Facts For Your Personal Formulary - I Xmlns - Xlink - HTTPDocument3 pagesDrug Facts For Your Personal Formulary - I Xmlns - Xlink - HTTPSaulNo ratings yet
- Antiarrhythmic Drugs: 1A: Prolong AP & Increase Refractory Period Moderate Effects On Conduction in Normal CellsDocument3 pagesAntiarrhythmic Drugs: 1A: Prolong AP & Increase Refractory Period Moderate Effects On Conduction in Normal CellsSaulNo ratings yet
- Nauli Arrhythmia PollEveQs PDFDocument1 pageNauli Arrhythmia PollEveQs PDFSaulNo ratings yet
- Assignment 1Document3 pagesAssignment 1SaulNo ratings yet
- Antiarrhythmic AgentsDocument11 pagesAntiarrhythmic AgentsanaeshklNo ratings yet
- Antiarrhythmic Drugs: 1A: Prolong AP & Increase Refractory Period Moderate Effects On Conduction in Normal CellsDocument4 pagesAntiarrhythmic Drugs: 1A: Prolong AP & Increase Refractory Period Moderate Effects On Conduction in Normal CellsSaulNo ratings yet
- iRAT Week 2 Quiz Instructions: Started: May 12 at 2:04pmDocument4 pagesiRAT Week 2 Quiz Instructions: Started: May 12 at 2:04pmSaulNo ratings yet
- Measurement and Descriptive Analysis Application ExercisesDocument3 pagesMeasurement and Descriptive Analysis Application ExercisesSaulNo ratings yet
- 20antiarrhythmic Agent PDFDocument4 pages20antiarrhythmic Agent PDFSaulNo ratings yet
- AntiHTN ChartDocument5 pagesAntiHTN ChartSaulNo ratings yet
- How To Set Up Your CVS AccountDocument1 pageHow To Set Up Your CVS AccountSaulNo ratings yet
- CDS/Order Set Questions for Dr. Dao’s LectureDocument4 pagesCDS/Order Set Questions for Dr. Dao’s LectureSaulNo ratings yet
- How To Set Up Your CVS AccountDocument1 pageHow To Set Up Your CVS AccountSaulNo ratings yet
- Attachment For Itemid 53438 PDFDocument1 pageAttachment For Itemid 53438 PDFSaulNo ratings yet
- Attachment For Itemid 53436-1Document1 pageAttachment For Itemid 53436-1SaulNo ratings yet
- PICO Preclass ExercisesDocument2 pagesPICO Preclass ExercisesSaulNo ratings yet
- Measurement and Descriptive Analysis Application ExercisesDocument3 pagesMeasurement and Descriptive Analysis Application ExercisesSaulNo ratings yet
- I Am Concerned About Furnishing Hormonal Contraception To Patients Under 18Document2 pagesI Am Concerned About Furnishing Hormonal Contraception To Patients Under 18SaulNo ratings yet
- Hair Loss Cases FACILITATORDocument3 pagesHair Loss Cases FACILITATORSaulNo ratings yet
- Rheumatoid Arthritis Pre-Reading - Summer 2020Document16 pagesRheumatoid Arthritis Pre-Reading - Summer 2020SaulNo ratings yet
- Clinical Aspect of MalariaDocument68 pagesClinical Aspect of MalariaselviaNo ratings yet
- HypospadiaDocument21 pagesHypospadiaShi YunNo ratings yet
- Fatty Tumors of The Thorax by CT: DemonstratedDocument6 pagesFatty Tumors of The Thorax by CT: DemonstratedAulia Rahman Prabowo UllikNo ratings yet
- BupivacaineDocument6 pagesBupivacaineKrystel Joy Auro100% (1)
- (NEJM, May 2023) - Medication-Related Osteonecrosis of The Jaw (Images in Clinical Medicine)Document1 page(NEJM, May 2023) - Medication-Related Osteonecrosis of The Jaw (Images in Clinical Medicine)NigelyulNo ratings yet
- OpisthorchisDocument17 pagesOpisthorchisIqraAzizNo ratings yet
- Paediatrica Indonesiana: Sri Yanti Harahap, Selvi Nafianti, Sri Sofyani, Supriatmo, Atan Baas SinuhajiDocument5 pagesPaediatrica Indonesiana: Sri Yanti Harahap, Selvi Nafianti, Sri Sofyani, Supriatmo, Atan Baas SinuhajiNadira Juanti PratiwiNo ratings yet
- Immunity and Vaccines As Biology Answers AQA OCR EdexcelDocument3 pagesImmunity and Vaccines As Biology Answers AQA OCR EdexcelShela HuangNo ratings yet
- NCM 116 - GIT (MODULE 5 Part II)Document6 pagesNCM 116 - GIT (MODULE 5 Part II)Meryville JacildoNo ratings yet
- Hydranencephaly: Cerebral Spinal Fluid Instead of Cerebral MantlesDocument8 pagesHydranencephaly: Cerebral Spinal Fluid Instead of Cerebral MantlesAmel LagiNo ratings yet
- Surgery 4 - Answers v1 (Wide)Document55 pagesSurgery 4 - Answers v1 (Wide)Humzala BashamNo ratings yet
- Gineco Eu An 2016 NR 3Document60 pagesGineco Eu An 2016 NR 3GîrbovanCristinaNo ratings yet
- Care Plan For Septic ArthritisDocument5 pagesCare Plan For Septic ArthritisokaciaNo ratings yet
- Valsartan 80 MG & 160 MG Tablets - Taj Pharma Leaflet Patient Medication InformationDocument3 pagesValsartan 80 MG & 160 MG Tablets - Taj Pharma Leaflet Patient Medication InformationTAJ PHARMA — A Health Care ProviderNo ratings yet
- Multiple Cranial Nerve PalsiesDocument11 pagesMultiple Cranial Nerve PalsiesVijay BabuNo ratings yet
- 3rd Mid CaseDocument32 pages3rd Mid CaseHarshini MakkenaNo ratings yet
- PEER - Stage2 - 10.1007/s00787 008 0701 0Document11 pagesPEER - Stage2 - 10.1007/s00787 008 0701 0Claire ClariceNo ratings yet
- CKD With Uremic GastropathyDocument4 pagesCKD With Uremic GastropathyMaretha Laksmi MahananiNo ratings yet
- NCP AirwayDocument2 pagesNCP AirwayjlucandoNo ratings yet
- Hand Hygiene Knowledge Assessment Questionnaire (IHI)Document2 pagesHand Hygiene Knowledge Assessment Questionnaire (IHI)Suseno Aji50% (2)
- Pediatrics CLINICAL QUESTIONDocument14 pagesPediatrics CLINICAL QUESTIONAyesha KhatunNo ratings yet
- Case 1: Group 4Document26 pagesCase 1: Group 4John Joshua Lacson MedicineNo ratings yet
- Open Letter To North Dakota Superintendents, School Board Members and ParentsDocument3 pagesOpen Letter To North Dakota Superintendents, School Board Members and Parentsinforumdocs100% (1)
- Commissioning Guide - Emergency General Surgery Acute Abdominal PainDocument32 pagesCommissioning Guide - Emergency General Surgery Acute Abdominal PainAnisNabillahMohdAzliNo ratings yet
- Atsp Book 2011Document24 pagesAtsp Book 2011Chengyuan ZhangNo ratings yet
- Congenital Scoliosis Case Study: Ashley (6-7 YearsDocument20 pagesCongenital Scoliosis Case Study: Ashley (6-7 YearsIulia Dulgheru100% (1)
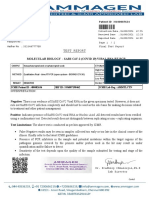
- Test Report: Patient ID 0100007634 Sid NoDocument2 pagesTest Report: Patient ID 0100007634 Sid NoBalamurugan ArumugamNo ratings yet
- Current Topics in Microbiology and ImunologyDocument203 pagesCurrent Topics in Microbiology and ImunologyAndreea StanescuNo ratings yet
- 3i HIRURGIJA - ŽELUCA I CRIJEVA Nejra Kikanović, Naida Kikanović I Indir Kulanić1275776300763Document20 pages3i HIRURGIJA - ŽELUCA I CRIJEVA Nejra Kikanović, Naida Kikanović I Indir Kulanić1275776300763Basketball is my loveNo ratings yet
- Rodaks Chapter Quizzes Chapter 35 43Document8 pagesRodaks Chapter Quizzes Chapter 35 43Maria MikaelaNo ratings yet