You might also like
- Spondyloarthropathies - Ankylosing Spondylitis, Psoriatic Arthritis, Reactive-Enteropathic Arthritis and HLA-B27 2020 PDFDocument125 pagesSpondyloarthropathies - Ankylosing Spondylitis, Psoriatic Arthritis, Reactive-Enteropathic Arthritis and HLA-B27 2020 PDFFazal Dalal100% (1)
- Otorhinolaryngology PDFDocument19 pagesOtorhinolaryngology PDFالطالب الطبيبNo ratings yet
- Preauricular Sinus and Its ManagmentDocument12 pagesPreauricular Sinus and Its ManagmentDr. T. Balasubramanian100% (7)
- Dr. Sana Bashir DPT, MS-CPPTDocument46 pagesDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- Common Throat Infections: A ReviewDocument5 pagesCommon Throat Infections: A ReviewharryNo ratings yet
- Otologic Manifestation of Systemic DiseaseDocument57 pagesOtologic Manifestation of Systemic DiseaseHERIZALNo ratings yet
- Uworld ENT NotesDocument4 pagesUworld ENT Notes808kailuaNo ratings yet
- OPP 3 Study Guide Exam 3Document158 pagesOPP 3 Study Guide Exam 3Fazal DalalNo ratings yet
- BronchiectasisDocument60 pagesBronchiectasisArulNo ratings yet
- Bimbingan UKMPPD (UKDI) - THTDocument152 pagesBimbingan UKMPPD (UKDI) - THTAvicenna_MSC100% (7)
- (Optima) Sopem Optima THT-KL Sep'19Document333 pages(Optima) Sopem Optima THT-KL Sep'19Ory LarasNo ratings yet
- Veterinary Aspects of Pigeon Breeding 2010Document78 pagesVeterinary Aspects of Pigeon Breeding 2010Iancu SebastianNo ratings yet
- LMU DCOM SecondaryDocument1 pageLMU DCOM SecondaryFazal Dalal50% (2)
- EennttDocument13 pagesEennttSuresh Kumar BansalNo ratings yet
- 5+6. Nasal Polyp & DNS PDFDocument43 pages5+6. Nasal Polyp & DNS PDFJames StiltonNo ratings yet
- LabyrinthitisDocument7 pagesLabyrinthitisChristie ZamoraNo ratings yet
- Fungal InfectionsDocument23 pagesFungal Infections180045No ratings yet
- Cavernous Sinus Thrombosis: Clinical FeaturesDocument4 pagesCavernous Sinus Thrombosis: Clinical FeaturesStefanus ChristianNo ratings yet
- Bacterial Uveitis - DR ArnavDocument59 pagesBacterial Uveitis - DR ArnavDr Arnav SaroyaNo ratings yet
- Presented By:-Dr. Saqib Majeed Salik Resident Maxillofacial Supervised By: - Dr. Suad A Ahmad Consultant Maxillofacial King Abdullah Hospital BishaDocument53 pagesPresented By:-Dr. Saqib Majeed Salik Resident Maxillofacial Supervised By: - Dr. Suad A Ahmad Consultant Maxillofacial King Abdullah Hospital BishaSaqib Majeed SalikNo ratings yet
- Anat Med & Surg March 7Document24 pagesAnat Med & Surg March 7sb medexNo ratings yet
- Diseases of AdenoidsDocument19 pagesDiseases of AdenoidsMacktevin FraterinNo ratings yet
- Behcet's DiseaseDocument21 pagesBehcet's DiseaseFazal DalalNo ratings yet
- BronchiectasisDocument17 pagesBronchiectasisShannon RamsumairNo ratings yet
- Orbital CellulitisDocument42 pagesOrbital CellulitisDita HannaNo ratings yet
- Echinococcosis 1Document38 pagesEchinococcosis 1Nadine SellersNo ratings yet
- ASOMDocument41 pagesASOMArunkumar S KumarNo ratings yet
- Respiratory Module Pathology Lecture 1, Upper Respiratory Tract, Atelectasis, ARDSDocument29 pagesRespiratory Module Pathology Lecture 1, Upper Respiratory Tract, Atelectasis, ARDSalielabadi10No ratings yet
- ENT 2marksDocument10 pagesENT 2marksSaileekitha AjamoniNo ratings yet
- Bacterial, Viral, Fungal and Protozoal InfectionsDocument60 pagesBacterial, Viral, Fungal and Protozoal Infectionsmaroosh.khalidNo ratings yet
- Clinical Findings: A. Specimens, Microscopic Examination, and CultureDocument3 pagesClinical Findings: A. Specimens, Microscopic Examination, and CultureLeah VicenteNo ratings yet
- Suppurative Lung Diseases.Document37 pagesSuppurative Lung Diseases.Salman KhanNo ratings yet
- Common Fungal InfectionsDocument23 pagesCommon Fungal Infections180045No ratings yet
- PneumoniaDocument24 pagesPneumoniaWidhi AstutiNo ratings yet
- Microbial Diseases of The Different Organ System and Epidem.Document36 pagesMicrobial Diseases of The Different Organ System and Epidem.Ysabelle GutierrezNo ratings yet
- PatomekanismeDocument18 pagesPatomekanismeEdwin Pasha Jr.No ratings yet
- 8 Bacterial DiseasesDocument51 pages8 Bacterial DiseasesDavid JamuNo ratings yet
- Oral Medicine - Update For The Dental Practitioner Lumps and SwellingsDocument9 pagesOral Medicine - Update For The Dental Practitioner Lumps and SwellingsGowriNo ratings yet
- PneumoniaDocument48 pagesPneumoniaDammaqsaa W BiyyanaaNo ratings yet
- Orbital CellulitisDocument42 pagesOrbital Cellulitismuhammad iqbalNo ratings yet
- Chronic Suppurative Otitis Media: Drhpsingh Additional ProfessorDocument44 pagesChronic Suppurative Otitis Media: Drhpsingh Additional ProfessorIndieNo ratings yet
- Ear Infections: These Include Otitis Externa, Otitis Media, MastoiditisDocument32 pagesEar Infections: These Include Otitis Externa, Otitis Media, Mastoiditiseugene ugayNo ratings yet
- Eye DiseaseDocument31 pagesEye DiseaseTsegaye YalewNo ratings yet
- Bronchiectasis DesieDocument77 pagesBronchiectasis DesieAbebe GelawNo ratings yet
- Disorders of Middle EarDocument32 pagesDisorders of Middle EarAhmad fayazNo ratings yet
- CBL Blok 8 Group 1Document6 pagesCBL Blok 8 Group 1Laura Putri TraviraNo ratings yet
- RhinosinusitisDocument10 pagesRhinosinusitisErika De JesusNo ratings yet
- 25.suppurative Lung DiseasesDocument6 pages25.suppurative Lung DiseasesDIVEN SolvonNo ratings yet
- StreptococciDocument43 pagesStreptococciAyeshaNo ratings yet
- Group 11 MastoiditisDocument23 pagesGroup 11 MastoiditisYen-Naah AdamsNo ratings yet
- Sino Nasal Polyposis SsDocument42 pagesSino Nasal Polyposis SsJeffrinNo ratings yet
- Nasal Polyps: LECTURER Ass: DR Hussein Omar ZukeDocument26 pagesNasal Polyps: LECTURER Ass: DR Hussein Omar ZukeAbdiqani MahdiNo ratings yet
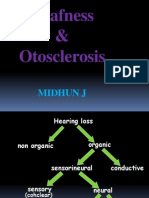
- Deafness & Otosclerosis: Midhun JDocument44 pagesDeafness & Otosclerosis: Midhun JRohit R PillaiNo ratings yet
- ENT Emergencies LectureDocument29 pagesENT Emergencies LectureThea Bertea100% (1)
- NoseDocument37 pagesNoseDawit workalemNo ratings yet
- The Oral Cavity - GIT PathologyDocument3 pagesThe Oral Cavity - GIT PathologyAakashNo ratings yet
- Infectious Uveitis AyuDocument19 pagesInfectious Uveitis AyuAndi Ayu LestariNo ratings yet
- Cavernous Sinus SyndromeDocument8 pagesCavernous Sinus SyndromeMuresan Ioana Catalina100% (1)
- Incidence: Specific Types of UveitisDocument15 pagesIncidence: Specific Types of UveitisImatunnisaZiNo ratings yet
- Suddensnhl 160220190525Document80 pagesSuddensnhl 160220190525mariahovhannisyanNo ratings yet
- 14-Diphtheria - Pertussis - and Brucellosis 44-45Document40 pages14-Diphtheria - Pertussis - and Brucellosis 44-45Manar AlhakamiNo ratings yet
- Behcet's DiseaseDocument21 pagesBehcet's DiseaseFazal DalalNo ratings yet
- Mirelesh Et Al, 1985 - Valproate and Clonazepam Comedication in Epilepsy-EpilepsiaDocument5 pagesMirelesh Et Al, 1985 - Valproate and Clonazepam Comedication in Epilepsy-EpilepsiaFazal DalalNo ratings yet
- Kwan Et Al 2000 - Epilepsy After The First Drug Fails Substitution or Addon?Document5 pagesKwan Et Al 2000 - Epilepsy After The First Drug Fails Substitution or Addon?Fazal DalalNo ratings yet
- French Et Al 2009 - Rational PolytherapyDocument6 pagesFrench Et Al 2009 - Rational PolytherapyFazal DalalNo ratings yet
- Baulac Et Al 2007 - Efficacy and Safety of Adjunctive Zonisamide Therapy For Refractory Partial SeizuresDocument9 pagesBaulac Et Al 2007 - Efficacy and Safety of Adjunctive Zonisamide Therapy For Refractory Partial SeizuresFazal DalalNo ratings yet