You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Radiation Incident Investigation Report FormDocument2 pagesRadiation Incident Investigation Report Formbenaoumeur benounaNo ratings yet
- RA11166 National HIV Law PresentationDocument40 pagesRA11166 National HIV Law PresentationRoots of HealthNo ratings yet
- Modifiers PDFDocument39 pagesModifiers PDFSyali SasidharanNo ratings yet
- PRC E-Tool Maternal Reviewed by Dr. BallenaDocument4 pagesPRC E-Tool Maternal Reviewed by Dr. BallenaMichael John F. NatividadNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document17 pagesPrinciples and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Sae TumNo ratings yet
- Directory of OfficersDocument5 pagesDirectory of OfficersAbhay Chauhan100% (1)
- One-Person Bag Valve Mask (BVM) : MarchDocument1 pageOne-Person Bag Valve Mask (BVM) : MarchSae TumNo ratings yet
- Head-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedDocument1 pageHead-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 14: Pain Medication and Antibiotic AdministrationDocument2 pagesSkills Assessment Checklist: MODULE 14: Pain Medication and Antibiotic AdministrationSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 19: Pre-Evacuation Procedures, Communication, and DocumentationDocument3 pagesSkills Assessment Checklist: MODULE 19: Pre-Evacuation Procedures, Communication, and DocumentationSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : Skill InstructionsDocument3 pagesPrinciples and Application of Tactical Field Care (TFC) : Skill InstructionsSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : Skill InstructionsDocument3 pagesPrinciples and Application of Tactical Field Care (TFC) : Skill InstructionsSae TumNo ratings yet
- One-Person Drag/Carry: Kit or Arm DragDocument5 pagesOne-Person Drag/Carry: Kit or Arm DragSae TumNo ratings yet
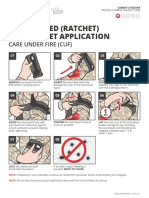
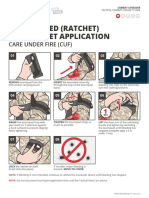
- One-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Document1 pageOne-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Sae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- Atbf Ista PDFDocument12 pagesAtbf Ista PDFSae TumNo ratings yet
- Atbf PDFDocument1 pageAtbf PDFSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 7: Airway ManagementDocument6 pagesSkills Assessment Checklist: MODULE 7: Airway ManagementSae TumNo ratings yet
- Two-Person Drag/Carry: Kit or Arm DragDocument3 pagesTwo-Person Drag/Carry: Kit or Arm DragSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 4: Principles and Application of Tactical Field CareDocument1 pageSkills Assessment Checklist: MODULE 4: Principles and Application of Tactical Field CareSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCDocument7 pagesSkills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCSae TumNo ratings yet
- Module 03 - Care Under Fire: Speaker NotesDocument12 pagesModule 03 - Care Under Fire: Speaker NotesSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- Module 14 - Analgesia and Antibiotic Administration: Speaker NotesDocument5 pagesModule 14 - Analgesia and Antibiotic Administration: Speaker NotesSae TumNo ratings yet
- Two-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Document1 pageTwo-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Sae TumNo ratings yet
- Evacuation Procedures: Skill InstructionsDocument3 pagesEvacuation Procedures: Skill InstructionsSae TumNo ratings yet
- Analgesia Administration/ Antibiotic Admin: Skill InstructionsDocument3 pagesAnalgesia Administration/ Antibiotic Admin: Skill InstructionsSae TumNo ratings yet
- Massive Hemorrhage Control in TFC: Skill InstructionsDocument8 pagesMassive Hemorrhage Control in TFC: Skill InstructionsSae TumNo ratings yet
- Module 13 - Eye Injuries: Speaker NotesDocument5 pagesModule 13 - Eye Injuries: Speaker NotesSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document17 pagesPrinciples and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Sae Tum0% (1)
- Module 07 - Airway Management in TFC: Speaker NotesDocument7 pagesModule 07 - Airway Management in TFC: Speaker NotesSae TumNo ratings yet
- Massive Hemorrhage Control in TFC: Skill InstructionsDocument8 pagesMassive Hemorrhage Control in TFC: Skill InstructionsSae TumNo ratings yet
- Module 11 - Hypothermia Prevention: Speaker NotesDocument6 pagesModule 11 - Hypothermia Prevention: Speaker NotesSae TumNo ratings yet
- Eye Injuries: Skill InstructionsDocument3 pagesEye Injuries: Skill InstructionsSae TumNo ratings yet
- Airway Management in TFC: Skill InstructionsDocument8 pagesAirway Management in TFC: Skill InstructionsSae TumNo ratings yet
- FD PDFDocument580 pagesFD PDFAinul LuthfiNo ratings yet
- Careers in MicrobiologyDocument3 pagesCareers in MicrobiologyAlisha patelNo ratings yet
- Piramal Ar Full 2015 16Document292 pagesPiramal Ar Full 2015 16Naman TandonNo ratings yet
- Wound Care Observation Checklist - FINALDocument2 pagesWound Care Observation Checklist - FINALHagar HanounNo ratings yet
- Unstructured Clinical Gestalt Vs Clinical Scores in Pulmonary EmbolismDocument21 pagesUnstructured Clinical Gestalt Vs Clinical Scores in Pulmonary EmbolismViswanath Reddy ChintaNo ratings yet
- Activity 12 MicrolabDocument3 pagesActivity 12 MicrolabDarius June Nolasco SacupasoNo ratings yet
- ICMR Consensus Guidelines On Do Not Attempt Resuscitation': Policy DocumentDocument8 pagesICMR Consensus Guidelines On Do Not Attempt Resuscitation': Policy DocumentAryan TiuNo ratings yet
- FCPS Community Medicine Training Program at Health Services Academy - Web ContentDocument13 pagesFCPS Community Medicine Training Program at Health Services Academy - Web ContentDrMubashir ShaikhNo ratings yet
- Updated Guidance BDDS Providers Temp Policy ChangesDocument17 pagesUpdated Guidance BDDS Providers Temp Policy ChangesIndiana Family to FamilyNo ratings yet
- Assessment Analysis Asgn - PattiDocument4 pagesAssessment Analysis Asgn - Pattiapi-449656005No ratings yet
- Literature Review On Maternal MortalityDocument8 pagesLiterature Review On Maternal Mortalityaflsqrbnq100% (1)
- Human Trafficking EssayDocument10 pagesHuman Trafficking EssayMeghri AshekianNo ratings yet
- FORM 2E: Health Plan Implementation For: Maternal Health: Post-Partum CareDocument2 pagesFORM 2E: Health Plan Implementation For: Maternal Health: Post-Partum CarePaul Mark PilarNo ratings yet
- Dr. Moni BhargavaDocument1 pageDr. Moni BhargavaAnirudh MittalNo ratings yet
- Super Speciality Hospital in KanpurDocument178 pagesSuper Speciality Hospital in KanpurgauravsriNo ratings yet
- JR 2 Prosthodontic Treatment in Patients With Temporomandibular Disorders and Orofacial Pain And:or BruxismDocument10 pagesJR 2 Prosthodontic Treatment in Patients With Temporomandibular Disorders and Orofacial Pain And:or Bruxismaulia zahroNo ratings yet
- Evidence Based Reading FormatDocument1 pageEvidence Based Reading Formatako at ang exoNo ratings yet
- Anesthesia and Monitoring Guidelines PDFDocument24 pagesAnesthesia and Monitoring Guidelines PDFAdan ManzanaresNo ratings yet
- Hospital Rules & Restrictions Within The Hospital Premises: Patient Helpline International Patient Mail UsDocument5 pagesHospital Rules & Restrictions Within The Hospital Premises: Patient Helpline International Patient Mail UsshangaviNo ratings yet
- Nursing at Harvard UNY 2Document4 pagesNursing at Harvard UNY 2Drajat FebrianNo ratings yet
- The Future of Quality and Accreditation SurveysDocument3 pagesThe Future of Quality and Accreditation SurveysnovizainNo ratings yet
- Welfare Checks and Therapeutic Risk Management.8Document5 pagesWelfare Checks and Therapeutic Risk Management.8Marco Dave Gutierrez ParedesNo ratings yet
- CaNaMed 2022 - Versiunea 04.11.2021Document266 pagesCaNaMed 2022 - Versiunea 04.11.2021Claudia BlmNo ratings yet
- Skripsi: ADLN Perpustakaan Universitas AirlanggaDocument48 pagesSkripsi: ADLN Perpustakaan Universitas Airlanggaalfian maulanaNo ratings yet
- Second Admission List Rematching PG 2024Document17 pagesSecond Admission List Rematching PG 2024amit996No ratings yet