You might also like
- Bio Factsheet: The Kidney: Excretion and OsmoregulationDocument4 pagesBio Factsheet: The Kidney: Excretion and OsmoregulationjesvinjesvinNo ratings yet
- Chapter 27 GuytonDocument6 pagesChapter 27 GuytonGabriella ChafrinaNo ratings yet
- Cafco Fendolite Mii Application Guidelines PDFDocument23 pagesCafco Fendolite Mii Application Guidelines PDFTanmay GorNo ratings yet
- Tubular ReabsorptionDocument42 pagesTubular Reabsorptionmina mounirNo ratings yet
- 6-Drugs Acting On The Renal System - 2Document65 pages6-Drugs Acting On The Renal System - 2Hamid Hussain HamidNo ratings yet
- PHS RenalDocument44 pagesPHS Renaltewogbadeomobuwajo005No ratings yet
- Pharmacology of Renal SystemDocument125 pagesPharmacology of Renal SystemBirhanu GetaNo ratings yet
- L5&6-Tubular Reabsorption& SecretionDocument38 pagesL5&6-Tubular Reabsorption& SecretionsairahhannahNo ratings yet
- Lec 14 - Kidney PDFDocument16 pagesLec 14 - Kidney PDFrajeshNo ratings yet
- Part 1 - US-Grade 4-BiochemistryDocument34 pagesPart 1 - US-Grade 4-BiochemistryFarah Bashar Al-RawachyNo ratings yet
- L3 +L4 Renal System 2023Document31 pagesL3 +L4 Renal System 2023mizare29gNo ratings yet
- CLS Aipmt 16 17 XI Zoo Study Package 2 SET 1 Chapter 6Document14 pagesCLS Aipmt 16 17 XI Zoo Study Package 2 SET 1 Chapter 6jaindhruv850No ratings yet
- 2 - Renal Secretion & AbsorptionDocument14 pages2 - Renal Secretion & AbsorptionHamzehNo ratings yet
- Renal NoteDocument20 pagesRenal Noteiroreredavid8No ratings yet
- Cicm Part 1 StudyDocument6 pagesCicm Part 1 StudyReesha CornelioNo ratings yet
- Mechanism of Filteration of Urine 5Document34 pagesMechanism of Filteration of Urine 5Akshay Pratap SinghNo ratings yet
- Proximal Tubule Function and Response To Acidosis: Norman P. Curthoys and Orson W. MoeDocument12 pagesProximal Tubule Function and Response To Acidosis: Norman P. Curthoys and Orson W. Moehrol31060No ratings yet
- QuestionsDocument4 pagesQuestionsA GoswamiNo ratings yet
- LOOP OF HENLE (Modified)Document25 pagesLOOP OF HENLE (Modified)Chuleha SethNo ratings yet
- UrinaryDocument87 pagesUrinaryJohn Paolo Dalida SalazarNo ratings yet
- 1 Renal Function - 20Document76 pages1 Renal Function - 20krystelmae009No ratings yet
- L4 Regional Transport 2023Document4 pagesL4 Regional Transport 2023bgj9cddvxhNo ratings yet
- Renal SystemDocument91 pagesRenal SystemKetheesaran LingamNo ratings yet
- DCT and Collecting DuctDocument29 pagesDCT and Collecting DuctayeshaNo ratings yet
- Handling of Certain Important Solutes by The Renal TubulesDocument14 pagesHandling of Certain Important Solutes by The Renal TubulesOsama MohamedNo ratings yet
- Excretion & Homeostasis Past Papers Q&ADocument13 pagesExcretion & Homeostasis Past Papers Q&AKimora Louetta JapNo ratings yet
- NCERT Solution For Class 11 Biology Chapter 19 Excretory Products and Their EliminationDocument6 pagesNCERT Solution For Class 11 Biology Chapter 19 Excretory Products and Their EliminationHafiz HussainNo ratings yet
- Transport Mech 09192011Document38 pagesTransport Mech 09192011Wesley SeeNo ratings yet
- Intestinal Ion Transport and The Pathophysiology of Diarrhea - PMCDocument22 pagesIntestinal Ion Transport and The Pathophysiology of Diarrhea - PMCtanatswa courtney matingoNo ratings yet
- NephronDocument5 pagesNephronrdeguzma100% (1)
- Test 4 Renal Gi Met DM AgingDocument9 pagesTest 4 Renal Gi Met DM AgingmeganNo ratings yet
- Physiology - BSDocument14 pagesPhysiology - BSkep1313No ratings yet
- Biokimia UrinDocument2 pagesBiokimia UrinAswin AgusNo ratings yet
- General Principles of Tubular ReabsorptionDocument54 pagesGeneral Principles of Tubular ReabsorptionRalph JacintoNo ratings yet
- Physiological Ion ChlorideDocument15 pagesPhysiological Ion ChlorideMohammad Arafat Siddiqui100% (2)
- Mechanism of Salivary GlandDocument5 pagesMechanism of Salivary GlandNirmala M. KarimatannisaNo ratings yet
- Differential Diagnosis of Hyperkalemia: An Update To A Complex ProblemDocument9 pagesDifferential Diagnosis of Hyperkalemia: An Update To A Complex ProblemMariana CabralNo ratings yet
- Hypokalemia: A Practical Approach To Diagnosis and TreatmentDocument17 pagesHypokalemia: A Practical Approach To Diagnosis and TreatmentIntan NoaNo ratings yet
- Excretory Products and Their EliminationDocument2 pagesExcretory Products and Their Eliminationadtydv007No ratings yet
- Filtration at Rest: Retention of WaterDocument19 pagesFiltration at Rest: Retention of WaterkoushiksarkerNo ratings yet
- Renal Extra Notes: Total Body Water (TBW) 0.6 X Body WeightDocument3 pagesRenal Extra Notes: Total Body Water (TBW) 0.6 X Body WeightKhaing26No ratings yet
- Ncert Solutions June6 For Class 11 Biology Chapter 19 Excretory Products and Their EliminationDocument7 pagesNcert Solutions June6 For Class 11 Biology Chapter 19 Excretory Products and Their Eliminationmehrahani03No ratings yet
- Ion TransportersDocument2 pagesIon TransportersfilipemedicinavrNo ratings yet
- Chapter 24. The Kidney.: 1. The Structure and Function of The NephronDocument8 pagesChapter 24. The Kidney.: 1. The Structure and Function of The NephronjeskevandiemenNo ratings yet
- Ex Cert IonDocument11 pagesEx Cert IonVicky BhardwajNo ratings yet
- Obat Pada Ginjal: Prof M.A.Widodo PHDDocument53 pagesObat Pada Ginjal: Prof M.A.Widodo PHDPriiya Ashiwini100% (1)
- Human Physiology Ii: School of BiochemistryDocument15 pagesHuman Physiology Ii: School of Biochemistrykeerthana t reddyNo ratings yet
- IM II - Fluids and Electrolytes (Lecture Trans)Document18 pagesIM II - Fluids and Electrolytes (Lecture Trans)Robert Francis DikioNo ratings yet
- Curt Hoys 2013Document12 pagesCurt Hoys 2013broken22No ratings yet
- Mabes Fluid and ElectrolytesDocument9 pagesMabes Fluid and ElectrolytesMabesNo ratings yet
- Renal Anatomy & PhysiologyDocument70 pagesRenal Anatomy & PhysiologyDeshi SportsNo ratings yet
- M - 126 Structure of Nephron and Function of The Kidney PDFDocument4 pagesM - 126 Structure of Nephron and Function of The Kidney PDFDr. Tapan Kr. Dutta100% (1)
- Urinary Tract PhysiologykulDocument72 pagesUrinary Tract PhysiologykulAya KamajayaNo ratings yet
- Distal Tubule Balance and Tubuloglomerular Feedback-Group 2Document42 pagesDistal Tubule Balance and Tubuloglomerular Feedback-Group 2Chuleha SethNo ratings yet
- Activity 36 - Urinary Tubular Reabsorption and SecretionDocument6 pagesActivity 36 - Urinary Tubular Reabsorption and SecretionKaren Joy MagbanuaNo ratings yet
- Distal Convoluted Tubules, Counter Current Mechanism, MicturitionDocument94 pagesDistal Convoluted Tubules, Counter Current Mechanism, MicturitionSarah BirechNo ratings yet
- Fluids and Electrolytes: 2. Interstitial SpaceDocument13 pagesFluids and Electrolytes: 2. Interstitial Spacehahahahaaaaaaa100% (1)
- 6 Renal PhysiologyDocument37 pages6 Renal PhysiologyD TekNo ratings yet
- Electrolyte Balance 2023Document51 pagesElectrolyte Balance 2023Salmonella TyphiNo ratings yet
- Renal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledFrom EverandRenal Reflections: Exploring the Marvels of Nephrology: The Intricate Ballet of Kidney Functions UnveiledNo ratings yet
- 3.2 Risk Rate Measures Cohort Studies PDFDocument3 pages3.2 Risk Rate Measures Cohort Studies PDFSherida GibbsNo ratings yet
- DiscussionDocument3 pagesDiscussionSherida GibbsNo ratings yet
- Social Psychology: Lecture 3.3: Group Pressure and Conformity (Part 1)Document1 pageSocial Psychology: Lecture 3.3: Group Pressure and Conformity (Part 1)Sherida GibbsNo ratings yet
- Week2-4pptphysiology Nervous System Organisation 2Document9 pagesWeek2-4pptphysiology Nervous System Organisation 2Sherida GibbsNo ratings yet
- H-P Axis-Thyroid: Learning ObjectivesDocument9 pagesH-P Axis-Thyroid: Learning ObjectivesSherida GibbsNo ratings yet
- Jennifer Carbrey Ph.D. Department of Cell BiologyDocument13 pagesJennifer Carbrey Ph.D. Department of Cell BiologySherida GibbsNo ratings yet
- Jennifer Carbrey Ph.D. Department of Cell Biology: Image by OCAL,, Public DomainDocument11 pagesJennifer Carbrey Ph.D. Department of Cell Biology: Image by OCAL,, Public DomainSherida GibbsNo ratings yet
- Doing Together What We Would Not Do Alone: Social PsychologyDocument8 pagesDoing Together What We Would Not Do Alone: Social PsychologySherida GibbsNo ratings yet
- The Female Reproductive System - 1Document9 pagesThe Female Reproductive System - 1Sherida GibbsNo ratings yet
- Digestive System - 4: Learning ObjectivesDocument4 pagesDigestive System - 4: Learning ObjectivesSherida GibbsNo ratings yet
- The Nervous System Action Potentials: Jennifer Carbrey Ph.D. Department of Cell BiologyDocument9 pagesThe Nervous System Action Potentials: Jennifer Carbrey Ph.D. Department of Cell BiologySherida GibbsNo ratings yet
- The Nervous System Organization: Jennifer Carbrey Ph.D. Department of Cell BiologyDocument8 pagesThe Nervous System Organization: Jennifer Carbrey Ph.D. Department of Cell BiologySherida GibbsNo ratings yet
- Reading4-3-Plous The Psy of Prejudice, Stereotyping and DiscriminationDocument49 pagesReading4-3-Plous The Psy of Prejudice, Stereotyping and DiscriminationSherida GibbsNo ratings yet
- Pulmonary Function Tests and Alveolar Ventilation: Introductory Human PhysiologyDocument3 pagesPulmonary Function Tests and Alveolar Ventilation: Introductory Human PhysiologySherida GibbsNo ratings yet
- Week3-6pptcaridac MuscleDocument7 pagesWeek3-6pptcaridac MuscleSherida GibbsNo ratings yet
- Types of Erosion:: River ProcessesDocument3 pagesTypes of Erosion:: River ProcessesSherida GibbsNo ratings yet
- Types of Erosion:: River ProcessesDocument3 pagesTypes of Erosion:: River ProcessesSherida GibbsNo ratings yet
- Title: Plan and Design AimDocument9 pagesTitle: Plan and Design AimSherida GibbsNo ratings yet
- Social Psychology: Lecture 6.1: Bystander Intervention in EmergenciesDocument2 pagesSocial Psychology: Lecture 6.1: Bystander Intervention in EmergenciesSherida GibbsNo ratings yet
- Social Psychology: Lecture 2.8: The Ins and Outs of Social InfluenceDocument2 pagesSocial Psychology: Lecture 2.8: The Ins and Outs of Social InfluenceSherida GibbsNo ratings yet
- Slaters RuleDocument2 pagesSlaters RulelubaajamesNo ratings yet
- Content in Demo TeachingDocument6 pagesContent in Demo TeachingAgustines, Marie Char C.No ratings yet
- Experiment 1 Determination of Solid and Moisture Content in SoilDocument4 pagesExperiment 1 Determination of Solid and Moisture Content in SoilnityaNo ratings yet
- Manufacturing Process-I (Casting)Document25 pagesManufacturing Process-I (Casting)Rahul Deb PalNo ratings yet
- Liquid-in-Glass Thermometry PDFDocument6 pagesLiquid-in-Glass Thermometry PDFBan ZanganaNo ratings yet
- CHEMISTRY (XII) CHAPTER 03 (Group IIIA and IVA Elements Short QuestionsDocument6 pagesCHEMISTRY (XII) CHAPTER 03 (Group IIIA and IVA Elements Short QuestionsMajid HafeezNo ratings yet
- Carte Tratamente - 2019Document102 pagesCarte Tratamente - 2019ZaZaNo ratings yet
- Alkyd Resins: 2. Unmodified Alkyds 163Document34 pagesAlkyd Resins: 2. Unmodified Alkyds 163Dewala KutaNo ratings yet
- OC - Halogen Derivatives - EDocument100 pagesOC - Halogen Derivatives - EJohn Doe100% (1)
- F-2021111-02 ANSUL NFF 3x3 UL201Document2 pagesF-2021111-02 ANSUL NFF 3x3 UL201Peter SorialNo ratings yet
- Chem 2122 General Chemistry IIDocument11 pagesChem 2122 General Chemistry IINezuko ChanNo ratings yet
- Dera Ghazi Khan Cement Industry : (Nishat Group of Industries)Document30 pagesDera Ghazi Khan Cement Industry : (Nishat Group of Industries)Muhammad Hamza RaheelNo ratings yet
- Class 12 Chemistry Project On Testing The Amount of Casein in MilkDocument14 pagesClass 12 Chemistry Project On Testing The Amount of Casein in MilkKartik ThakurNo ratings yet
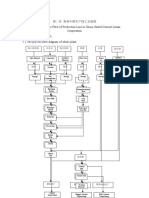
- 2 Process Flow of Production Line in China United Cement Lunan Corporation - Íð - + ÑêiDocument5 pages2 Process Flow of Production Line in China United Cement Lunan Corporation - Íð - + ÑêiNova HeriNo ratings yet
- Vol16 2Document19 pagesVol16 2Aivan BandiolaNo ratings yet
- Prequalified Vendor List 2020-2023 QRF/7.4/02Document88 pagesPrequalified Vendor List 2020-2023 QRF/7.4/02AJEET KUMARNo ratings yet
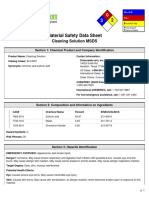
- Cleaning Solution MSDS: Section 1: Chemical Product and Company IdentificationDocument6 pagesCleaning Solution MSDS: Section 1: Chemical Product and Company Identificationfirman analisNo ratings yet
- J of Applied Polymer Sci - 2023 - Zhang - Advances in Wound Dressing Based On Electrospinning NanofibersDocument28 pagesJ of Applied Polymer Sci - 2023 - Zhang - Advances in Wound Dressing Based On Electrospinning NanofibersSelvabala904260No ratings yet
- ET78901LSDocument2 pagesET78901LSKhalid ZaeemNo ratings yet
- Spore Packing List Record (3) AutosaveDocument139 pagesSpore Packing List Record (3) AutosaveErlinawati Bintu SupiyoNo ratings yet
- General Standard For Cheese CXS 283-1978Document5 pagesGeneral Standard For Cheese CXS 283-1978Laidy ArtiNo ratings yet
- Catagory Ame Data PDF FreeDocument224 pagesCatagory Ame Data PDF FreeRICL Sales ISONo ratings yet
- Course Work ChemistryDocument4 pagesCourse Work ChemistryAamerNo ratings yet
- Roads: Master Specification RD-PV-D1 Pavement Design (Austroads Supplement)Document52 pagesRoads: Master Specification RD-PV-D1 Pavement Design (Austroads Supplement)La FoliakNo ratings yet
- S TR CIVIL ROAD (Rev.0 2018) 1648785718327Document18 pagesS TR CIVIL ROAD (Rev.0 2018) 1648785718327Vimala PonnusamyNo ratings yet
- Humic Acid From CoalDocument13 pagesHumic Acid From CoalChemical.AliNo ratings yet
- Sanifect Disinfectant-Sanitizer MSDSDocument3 pagesSanifect Disinfectant-Sanitizer MSDSdani ramdaniNo ratings yet
- Hexagonal Posts: One End Male Thread One End Female ThreadDocument1 pageHexagonal Posts: One End Male Thread One End Female ThreadAn AnNo ratings yet
- Chapter 55 - Environmental Pollution ControlDocument75 pagesChapter 55 - Environmental Pollution ControlSurya ChakradhariNo ratings yet