You might also like
- Thought Record SheetDocument1 pageThought Record Sheetpanickedchick100% (2)
- 10 1016@j JHT 2017 02 001 PDFDocument10 pages10 1016@j JHT 2017 02 001 PDFGusti Ayu KrisnayantiNo ratings yet
- Kavitt Robert T Diagnosis and Treatment of Peptic 2019Document10 pagesKavitt Robert T Diagnosis and Treatment of Peptic 2019Nix Santos100% (1)
- Binomial DistributionDocument22 pagesBinomial DistributionNix SantosNo ratings yet
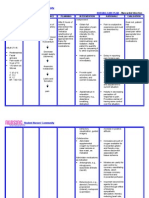
- Nursing Care Plan - Myocardial InfarctionDocument3 pagesNursing Care Plan - Myocardial Infarctionderic80% (10)
- DBT Skills Mods Pt3Document41 pagesDBT Skills Mods Pt3Ionelia Pașa100% (8)
- Sujok InpancreatitisDocument70 pagesSujok InpancreatitisFedericoz Zarra100% (1)
- Jurnal PendidikaDocument10 pagesJurnal PendidikaTessa Bagus AriyantoNo ratings yet
- Acupuncture For Primary Fibromyalgia: Study Protocol of A Randomized Controlled TrialDocument9 pagesAcupuncture For Primary Fibromyalgia: Study Protocol of A Randomized Controlled TrialSILVIA ROSARIO CHALCO MENDOZANo ratings yet
- Review ArticleDocument15 pagesReview ArticleAugustinNo ratings yet
- TENS - ArticleDocument10 pagesTENS - ArticleMickael LopesNo ratings yet
- Clinical StudyDocument8 pagesClinical Studylilis pratiwiNo ratings yet
- Review Article: The Effectiveness and Safety of Acupuncture For Patients With Chronic Urticaria: A Systematic ReviewDocument7 pagesReview Article: The Effectiveness and Safety of Acupuncture For Patients With Chronic Urticaria: A Systematic ReviewGianni MarinNo ratings yet
- Antipsychotics For Preventing Delirium in Hospitalized AdultsDocument12 pagesAntipsychotics For Preventing Delirium in Hospitalized AdultsLuis CsrNo ratings yet
- Efficacy of Transoral IncisionDocument14 pagesEfficacy of Transoral IncisionResidentes CirugiaNo ratings yet
- Bell's PalsyDocument12 pagesBell's Palsycorememories10No ratings yet
- Outcome Measures in Clinical Trials of TraditionalDocument8 pagesOutcome Measures in Clinical Trials of TraditionalOSMAR FAVIO FERNANDEZ SOLARNo ratings yet
- 2015 Article 815Document16 pages2015 Article 815silvia silalahiNo ratings yet
- Efficacy and Safety of Electroacupuncture For Post Stroke Depression: Study Protocol For A Randomized Controlled TrialDocument8 pagesEfficacy and Safety of Electroacupuncture For Post Stroke Depression: Study Protocol For A Randomized Controlled TrialwindapuspitasalimNo ratings yet
- Pulsed Radiofrequency ofDocument8 pagesPulsed Radiofrequency ofDiego Pinto PatroniNo ratings yet
- POLYDIOXANONE No.1 PDFDocument11 pagesPOLYDIOXANONE No.1 PDFHector Javier Torres GomezNo ratings yet
- TTH KronisDocument8 pagesTTH KronisseruniallisaaslimNo ratings yet
- A Randomized Clinical Trial of The Effectiveness of Mechanical Traction For Sub-Groups of Patients With Low Back Pain: Study Methods and RationaleDocument10 pagesA Randomized Clinical Trial of The Effectiveness of Mechanical Traction For Sub-Groups of Patients With Low Back Pain: Study Methods and RationaleNelsonRodríguezDeLeónNo ratings yet
- Lin2019 Article JinSThree-needleAcupunctureTecDocument9 pagesLin2019 Article JinSThree-needleAcupunctureTecIgnacio CoccioloNo ratings yet
- Surgical Versus Medical Treatment of Drug-Resistant Epilepsy: A Systematic Review and Meta-AnalysisDocument10 pagesSurgical Versus Medical Treatment of Drug-Resistant Epilepsy: A Systematic Review and Meta-AnalysisSebastianNo ratings yet
- Journal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDDocument9 pagesJournal of Hand Therapy: Hayat Hamzeh PT, MSC, Mohammad Madi PT, PHD, Alia A. Alghwiri PT, PHD, Ziad Hawamdeh MD, PHDWinda FRNo ratings yet
- Frazzitta Et AlDocument8 pagesFrazzitta Et Alalex ormazabalNo ratings yet
- MeduriDocument4 pagesMeduriSilvia Leticia BrunoNo ratings yet
- How Effective Are Physiotherapy Interventions in Treating People With Sciatica? A Systematic Review and Meta AnalysisDocument18 pagesHow Effective Are Physiotherapy Interventions in Treating People With Sciatica? A Systematic Review and Meta AnalysisXavi MartinezNo ratings yet
- RCR MindfullnesDocument9 pagesRCR MindfullnesDian Oktaria SafitriNo ratings yet
- Aphasia Recovery: When, How and Who To Treat?Document7 pagesAphasia Recovery: When, How and Who To Treat?Mohammed Dr.adjedNo ratings yet
- Complementaria 1. Aphasia Recovery When, How and Who To TreatDocument7 pagesComplementaria 1. Aphasia Recovery When, How and Who To TreatCarlonchaCáceresNo ratings yet
- 2014 - Auricular Acupressure Helps Improve Sleep Quality For Severe Insomnia in Maintenance Hemodialysis Patients A Pilot StudyDocument8 pages2014 - Auricular Acupressure Helps Improve Sleep Quality For Severe Insomnia in Maintenance Hemodialysis Patients A Pilot StudyJoão PauloNo ratings yet
- 2017 Article 1792Document12 pages2017 Article 1792CarlaMNo ratings yet
- Insomnia 6Document14 pagesInsomnia 6Utomo FemtomNo ratings yet
- The Effect of A Structured Medication Review On Quality of Life in Parkinson's Disease The Study ProtocolDocument7 pagesThe Effect of A Structured Medication Review On Quality of Life in Parkinson's Disease The Study ProtocolGurgehNo ratings yet
- Complementary Therapies in Medicine: Matthew Krouwel, Amanda Farley, Sheila Greenfield, Tariq Ismail, Kate JollyDocument9 pagesComplementary Therapies in Medicine: Matthew Krouwel, Amanda Farley, Sheila Greenfield, Tariq Ismail, Kate JollyPhilippe MirasNo ratings yet
- Acupuncture Methods For Functional Constipation: Protocol For A Systematic Review and Network Meta-AnalysisDocument10 pagesAcupuncture Methods For Functional Constipation: Protocol For A Systematic Review and Network Meta-AnalysisMohmmad Hossein NazariNo ratings yet
- Bmjopen 2014 005092Document8 pagesBmjopen 2014 005092MartaNo ratings yet
- Appi Ajp 2021 21121221Document3 pagesAppi Ajp 2021 21121221benediktNo ratings yet
- Vagal Nerve Stimulation For Treatment Resistant DepressionDocument14 pagesVagal Nerve Stimulation For Treatment Resistant DepressionCTAFDocuments100% (1)
- Rapid Rehabilitation Nursing in Postoperative Patients With Colorectal Cancer and Quality of LifeDocument8 pagesRapid Rehabilitation Nursing in Postoperative Patients With Colorectal Cancer and Quality of Lifejamie carpioNo ratings yet
- Jurnal Anes 3Document10 pagesJurnal Anes 3Ari SamadNo ratings yet
- Review Article: Clinical Efficacy of Acupuncture On Rheumatoid Arthritis and Associated Mechanisms: A Systemic ReviewDocument22 pagesReview Article: Clinical Efficacy of Acupuncture On Rheumatoid Arthritis and Associated Mechanisms: A Systemic Reviewdeepa rNo ratings yet
- Ramirez 2013Document10 pagesRamirez 2013Nadia Farah FadhilaNo ratings yet
- Eye Acupuncture For Pain Conditions: A Scoping Review of Clinical StudiesDocument10 pagesEye Acupuncture For Pain Conditions: A Scoping Review of Clinical StudiesIngdrawati TjiangNo ratings yet
- 1 s2.0 S1876382020302237 MainDocument9 pages1 s2.0 S1876382020302237 MainosmarcruzNo ratings yet
- Do Analgesics Improve Functioning in Patients With Chronic Low Back Pain? An Explorative Triple-Blinded RCTDocument7 pagesDo Analgesics Improve Functioning in Patients With Chronic Low Back Pain? An Explorative Triple-Blinded RCTMiki DoktorNo ratings yet
- Upper Airway Stimulation For Obstructive Sleep Apnea: Durability of The Treatment Effect at 18 MonthsDocument9 pagesUpper Airway Stimulation For Obstructive Sleep Apnea: Durability of The Treatment Effect at 18 MonthsHamzeh AlsalhiNo ratings yet
- Acupuncture As An Early Treatment For Idiopathic SDocument8 pagesAcupuncture As An Early Treatment For Idiopathic SBTS LGONo ratings yet
- Acupoint Catgut Embedding Therapy For FunctionalDocument5 pagesAcupoint Catgut Embedding Therapy For FunctionalJuan Pablo MejíaNo ratings yet
- Osteopathic Health Outcomes in Chronic Low Back PainDocument8 pagesOsteopathic Health Outcomes in Chronic Low Back PainPaola GuerraNo ratings yet
- Research ArticleDocument20 pagesResearch ArticleHaisheng ZhangNo ratings yet
- Review ArticleDocument15 pagesReview ArticleVidya Fajrin NingtyasNo ratings yet
- Evidence Based OrthopaedicsDocument663 pagesEvidence Based Orthopaedicssamabdelaal2000No ratings yet
- Ini JugaDocument8 pagesIni JugaSasti aliciaNo ratings yet
- Effects of A Transitional Palliative Care Model On Patients With End-Stage Heart Failure - A Randomised Controlled TrialDocument9 pagesEffects of A Transitional Palliative Care Model On Patients With End-Stage Heart Failure - A Randomised Controlled TrialcharmyshkuNo ratings yet
- Decreased Blood Pressure Among Community Dwelling Older Adults Following Progressive Muscle Relaxation and Music Therapy (RESIK)Document6 pagesDecreased Blood Pressure Among Community Dwelling Older Adults Following Progressive Muscle Relaxation and Music Therapy (RESIK)Rara Mitha64No ratings yet
- HypertensiDocument7 pagesHypertensizazaNo ratings yet
- Aripiprazol LAI Vs Paliperidona LAI in SKDocument10 pagesAripiprazol LAI Vs Paliperidona LAI in SKRobert MovileanuNo ratings yet
- Soleimani 2015Document13 pagesSoleimani 2015Leila FortesNo ratings yet
- Ed 58Document8 pagesEd 58Luís CorreiaNo ratings yet
- Efficacy, Acceptability, and Safety of Antidepressants For Low Back Pain: A Systematic Review and Meta-AnalysisDocument13 pagesEfficacy, Acceptability, and Safety of Antidepressants For Low Back Pain: A Systematic Review and Meta-Analysisskola onlajnNo ratings yet
- Upper-Airway Stimulation For Obstructive Sleep Apnea: Intern:Arezo Hayati/ Attend:Dr - AzargounDocument34 pagesUpper-Airway Stimulation For Obstructive Sleep Apnea: Intern:Arezo Hayati/ Attend:Dr - AzargounAnonymous kVwp7DNo ratings yet
- Jurnal BekamDocument8 pagesJurnal BekamAprilia nur ainiNo ratings yet
- Papers: Systematic Review and Economic Evaluation of HelicobacterDocument6 pagesPapers: Systematic Review and Economic Evaluation of HelicobacterNix SantosNo ratings yet
- Capannolo Annalisa Duodenal Lymphocytosis in 2019Document4 pagesCapannolo Annalisa Duodenal Lymphocytosis in 2019Nix SantosNo ratings yet
- SAJPsy 25 1382 PDFDocument7 pagesSAJPsy 25 1382 PDFNix SantosNo ratings yet
- Ford A C Efficacy of Psychotropic Drugs in Functional 2015 PDFDocument11 pagesFord A C Efficacy of Psychotropic Drugs in Functional 2015 PDFNix SantosNo ratings yet
- Ford A C Efficacy of Psychotropic Drugs in Functional 2015 PDFDocument11 pagesFord A C Efficacy of Psychotropic Drugs in Functional 2015 PDFNix SantosNo ratings yet
- ACG - and - CAG - Clinical - Guideline - Management - of Dyspepsia PDFDocument26 pagesACG - and - CAG - Clinical - Guideline - Management - of Dyspepsia PDFhidayat0781No ratings yet
- Psychological Interventions For Non-Ulcer Dyspepsia (Unknown)Document14 pagesPsychological Interventions For Non-Ulcer Dyspepsia (Unknown)Nix SantosNo ratings yet
- Jung Hye Kyung Systematic Review With Meta Analysis 2015 PDFDocument2 pagesJung Hye Kyung Systematic Review With Meta Analysis 2015 PDFNix SantosNo ratings yet
- Soo Shelly Psychological Interventions For Non Ulcer 2005Document14 pagesSoo Shelly Psychological Interventions For Non Ulcer 2005Nix SantosNo ratings yet
- A American Heart Journal 156-3-564-572.e2Document11 pagesA American Heart Journal 156-3-564-572.e2Nix SantosNo ratings yet
- NRSG Care Pacemaker - Implant PDFDocument1 pageNRSG Care Pacemaker - Implant PDFNix SantosNo ratings yet
- CHAPTER 15 Part 2 1Document5 pagesCHAPTER 15 Part 2 1Nix SantosNo ratings yet
- NRSG Care Pacemaker - Implant PDFDocument1 pageNRSG Care Pacemaker - Implant PDFNix SantosNo ratings yet
- Evidence Based Nursing ArticleDocument14 pagesEvidence Based Nursing ArticleNix SantosNo ratings yet
- Fundoscopic ExaminationDocument15 pagesFundoscopic ExaminationMarium Hayat0% (1)
- SUCCEESSFULLY Navigating The First Year of Surgical ResidencyDocument56 pagesSUCCEESSFULLY Navigating The First Year of Surgical ResidencyYoya LawiNo ratings yet
- Herbal Medicine Guide: Benefits, Uses and Safety TipsDocument12 pagesHerbal Medicine Guide: Benefits, Uses and Safety TipsVer BautistaNo ratings yet
- Cancer Chemotherapy and Its ComplicationDocument49 pagesCancer Chemotherapy and Its ComplicationLina AnisaNo ratings yet
- Hydrotherapy: Dr. Lakshmi NairDocument24 pagesHydrotherapy: Dr. Lakshmi NairLakshmi PavaniNo ratings yet
- Learning Contract SamplesDocument25 pagesLearning Contract SamplesClayton BaxterNo ratings yet
- Nursing Bylaws 2009Document30 pagesNursing Bylaws 2009Silviana FassicaNo ratings yet
- Oral Sensorimotor Therapy in Pediatric DysphagiaDocument1 pageOral Sensorimotor Therapy in Pediatric Dysphagiashaghala38No ratings yet
- General Explanation of Water Analysis ReportDocument2 pagesGeneral Explanation of Water Analysis Reportsuko winartiNo ratings yet
- Best Tips For Weight LossDocument2 pagesBest Tips For Weight LossRico LastNo ratings yet
- HHS Pre-doctoral Internship in Clinical NeuropsychologyDocument10 pagesHHS Pre-doctoral Internship in Clinical NeuropsychologyGifuGifuNo ratings yet
- 2012 IDF Guide For Nurses FINALDocument60 pages2012 IDF Guide For Nurses FINALkitsilcNo ratings yet
- Tongue Thrust and Braces: A Question and Answer GuideDocument2 pagesTongue Thrust and Braces: A Question and Answer GuideghyonasNo ratings yet
- SinnusitisDocument15 pagesSinnusitisAbigail BrillantesNo ratings yet
- EXPAREL Prescribing InformationDocument17 pagesEXPAREL Prescribing InformationcignalNo ratings yet
- Kelly Arrington ResumeDocument2 pagesKelly Arrington Resumeapi-413358891No ratings yet
- Red BWS - SDSDocument2 pagesRed BWS - SDSRezoanul Haque50% (2)
- GoiterDocument6 pagesGoiterslaya04No ratings yet
- 06-Systematic Review of Perforated Appendicitis and PhlegmonDocument7 pages06-Systematic Review of Perforated Appendicitis and PhlegmonTo MarNo ratings yet
- Book 1Document311 pagesBook 1Agie ArieNo ratings yet
- NPS Medicines ListDocument2 pagesNPS Medicines ListCin BinNo ratings yet
- Anaemia in PregnancyDocument28 pagesAnaemia in PregnancyUsman G. HingoroNo ratings yet
- Pacemaker ImplantationDocument17 pagesPacemaker ImplantationKaku ManishaNo ratings yet
- Moor Field UpdatedDocument754 pagesMoor Field UpdatedIrini ChatziralliNo ratings yet
- Hirschsprung Disease FarieDocument38 pagesHirschsprung Disease FarieFarie Farihan67% (3)
- Bene Ts of Using Fluorescence Induced Theragnosis in Fixed Orthodontic Therapy: Status, Technology and Future TrendsDocument7 pagesBene Ts of Using Fluorescence Induced Theragnosis in Fixed Orthodontic Therapy: Status, Technology and Future TrendsTiagoNo ratings yet
- Psychology: (8th Edition, in Modules) David MyersDocument23 pagesPsychology: (8th Edition, in Modules) David MyersJames ModulesNo ratings yet
- Lec. B12Document94 pagesLec. B12Arshad Mehmood MinhasNo ratings yet