You might also like
- Concept and Reality in Early Buddhist Thought PDFDocument176 pagesConcept and Reality in Early Buddhist Thought PDFMatt Aldridge100% (1)
- Narrative Cognitive Behavior Therapy For PsychosisDocument12 pagesNarrative Cognitive Behavior Therapy For PsychosisGanellNo ratings yet
- Psychotherapy For Treating Anxiety DisordersDocument11 pagesPsychotherapy For Treating Anxiety DisordersShaista ArshadNo ratings yet
- DBT For PTSD Related To Childhood Sexual AbuseDocument5 pagesDBT For PTSD Related To Childhood Sexual Abusecameronanddianne3785No ratings yet
- Erickson - Experiencing Hypnosis v1Document164 pagesErickson - Experiencing Hypnosis v1Puruf PufNo ratings yet
- Buddhist Mindful Vs Contemporary Psychology Paradox ArticleDocument6 pagesBuddhist Mindful Vs Contemporary Psychology Paradox ArticleMatt AldridgeNo ratings yet
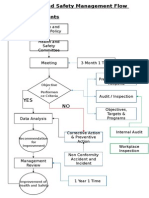
- Health and Safety FlowDocument6 pagesHealth and Safety Flowzaki0304No ratings yet
- Spiritual Crisis and RecoveryDocument8 pagesSpiritual Crisis and RecoveryMatt AldridgeNo ratings yet
- The Philosophy of Science - A Very Short Introduction PDFDocument1 pageThe Philosophy of Science - A Very Short Introduction PDFMatt Aldridge0% (1)
- FCA (SA) - Part - II - Past - Papers 7Document29 pagesFCA (SA) - Part - II - Past - Papers 7matentenNo ratings yet
- Depression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesFrom EverandDepression Conceptualization and Treatment: Dialogues from Psychodynamic and Cognitive Behavioral PerspectivesChristos CharisNo ratings yet
- I. Introduction To Special EducationDocument9 pagesI. Introduction To Special EducationJennylyn Boiser100% (1)
- CASP Case Control Study Checklist 2018 - Fillable - Form PDFDocument6 pagesCASP Case Control Study Checklist 2018 - Fillable - Form PDFEllieNo ratings yet
- Sensorimotor Approach To TreatmentDocument23 pagesSensorimotor Approach To TreatmentJonathon BenderNo ratings yet
- The Oral Transmission of Early Buddhist Literature PDFDocument32 pagesThe Oral Transmission of Early Buddhist Literature PDFMatt AldridgeNo ratings yet
- Panic Disorder Francesetti PDFDocument11 pagesPanic Disorder Francesetti PDFCésarRuizNo ratings yet
- SchizophreniaDocument10 pagesSchizophreniaapi-462485274100% (1)
- The Early Warning Signs in SchizophreniaDocument11 pagesThe Early Warning Signs in Schizophreniaamelia welindaNo ratings yet
- 2005 Max Birchwood Psychological Pathways To Depression in SchizophreniaDocument11 pages2005 Max Birchwood Psychological Pathways To Depression in Schizophreniaadni halianieNo ratings yet
- Development of Psychology and Psychiatry in Trinidad and TobagoDocument16 pagesDevelopment of Psychology and Psychiatry in Trinidad and Tobagokelsey abrahamNo ratings yet
- The Early Stages of Schizophrenia: Speculations On Pathogenesis, Pathophysiology, and Therapeutic ApproachesDocument14 pagesThe Early Stages of Schizophrenia: Speculations On Pathogenesis, Pathophysiology, and Therapeutic Approachespaul tNo ratings yet
- Bystritsky Anxiety Treatment Overview Pharm Therap 2013Document14 pagesBystritsky Anxiety Treatment Overview Pharm Therap 2013Amanuel MaruNo ratings yet
- Wolf 2014Document37 pagesWolf 2014Cindy GautamaNo ratings yet
- Is Mindfulness For Psychosis Harmful? Deconstructing A Myth: EditorialDocument2 pagesIs Mindfulness For Psychosis Harmful? Deconstructing A Myth: EditorialReinhold MuñozNo ratings yet
- Progress in Neuropsychopharmacology & Biological PsychiatryDocument16 pagesProgress in Neuropsychopharmacology & Biological PsychiatryBetu SasuNo ratings yet
- Reciprocal Relations of Worry, Rumination, and Psychopathology Symptoms After Loss: A Prospective Cohort StudyDocument14 pagesReciprocal Relations of Worry, Rumination, and Psychopathology Symptoms After Loss: A Prospective Cohort StudyChelsey XieNo ratings yet
- Evaluacion y Tratamiento Psicodinamico en Pacientes TraumatiDocument12 pagesEvaluacion y Tratamiento Psicodinamico en Pacientes TraumatijoNo ratings yet
- Seminar Handout - Terminal IllnessDocument5 pagesSeminar Handout - Terminal IllnessSwarnaa ChakrabortyNo ratings yet
- Drug Treatment of Depressive Symptoms in SchizophreniaDocument13 pagesDrug Treatment of Depressive Symptoms in SchizophreniaSamanNo ratings yet
- 情绪障碍跨诊断治疗的统一方案 治疗师指南 第二版 英文Document121 pages情绪障碍跨诊断治疗的统一方案 治疗师指南 第二版 英文Chunfeng LiuNo ratings yet
- Sesgos de Memoria en Los Trastornos de AnsiedadDocument15 pagesSesgos de Memoria en Los Trastornos de AnsiedadIMHNo ratings yet
- Capítulo 1 ComptonDocument22 pagesCapítulo 1 ComptonBooster CNo ratings yet
- Stuck in A Rut: Rethinking Depression and Its Treatment: Paul E. Holtzheimer and Helen S. MaybergDocument9 pagesStuck in A Rut: Rethinking Depression and Its Treatment: Paul E. Holtzheimer and Helen S. MaybergIlias MaNo ratings yet
- Psychoanalytic Versus Psychodynamic Therapy For DepressionDocument19 pagesPsychoanalytic Versus Psychodynamic Therapy For DepressionNéstor X. PortalatínNo ratings yet
- Assessment and Treatment of Individuals at High RiDocument8 pagesAssessment and Treatment of Individuals at High Rifahad rustamNo ratings yet
- NIH Public Access: Author ManuscriptDocument5 pagesNIH Public Access: Author ManuscriptHelena WagnerNo ratings yet
- 1 s2.0 S0272735817302957 Main PDFDocument26 pages1 s2.0 S0272735817302957 Main PDFQasim ChacharNo ratings yet
- Eggart 2020Document11 pagesEggart 2020Rikus OfAthasNo ratings yet
- Anxiety Disorder Psychological Testing Research WorkDocument7 pagesAnxiety Disorder Psychological Testing Research Workshaswat chaudharyNo ratings yet
- Emotions and IllnessDocument8 pagesEmotions and IllnessioanaNo ratings yet
- Psychoeducation For Severe Mental Illnesses Theory and Practice, Final Seminar PrintDocument22 pagesPsychoeducation For Severe Mental Illnesses Theory and Practice, Final Seminar PrintAnnPSWNo ratings yet
- 2019 EspenDocument10 pages2019 Espennermal93No ratings yet
- Wuthrich 2013Document8 pagesWuthrich 2013Rafael MoraesNo ratings yet
- Depression and Suicidality in First Episode PsychoDocument9 pagesDepression and Suicidality in First Episode PsychoNatalia Martinez CastroNo ratings yet
- Diagnosis of Depression in Elderly PatientsDocument8 pagesDiagnosis of Depression in Elderly PatientsJosé Jair Campos ReisNo ratings yet
- TMP ED34Document9 pagesTMP ED34FrontiersNo ratings yet
- RetrieveDocument12 pagesRetrieveAna Cristina Paiz ZepedaNo ratings yet
- Brosschot2006 - Emotii Si StresDocument12 pagesBrosschot2006 - Emotii Si StresgicutaNo ratings yet
- Suicide Attempts in First-Episode Psychosis 2Document6 pagesSuicide Attempts in First-Episode Psychosis 2Adam García BuenoNo ratings yet
- Symptoms and DiagnosisDocument5 pagesSymptoms and DiagnosisAndrew GrimesNo ratings yet
- Activation Vs Experiential Avoidance As A Transdia PDFDocument12 pagesActivation Vs Experiential Avoidance As A Transdia PDFpsicologia ejartNo ratings yet
- Horowitz 1997Document9 pagesHorowitz 1997Alexandra OanaNo ratings yet
- Generalized Anxiety Disorder: The Diagnosis and Treatment ofDocument20 pagesGeneralized Anxiety Disorder: The Diagnosis and Treatment ofRonaMaulidiaBakhitaNo ratings yet
- Treatment of Acute Stress DisorderDocument11 pagesTreatment of Acute Stress DisorderKusnanto Penasehat Kpb RyusakiNo ratings yet
- Chochinov DistressDocument11 pagesChochinov DistressThatiana GimenesNo ratings yet
- Godlewska 2019 Cognitive Neuropsychological Theory of Antidepressant Action: A Modern-Day Approach To Depression and Its TreatmentDocument14 pagesGodlewska 2019 Cognitive Neuropsychological Theory of Antidepressant Action: A Modern-Day Approach To Depression and Its TreatmentJahlin HabbeiNo ratings yet
- Personality Dimensions and Depression: Review and CommentaryDocument11 pagesPersonality Dimensions and Depression: Review and Commentarysofia valloryNo ratings yet
- Schizophr Bull 2000 Garety 73 86CBTDocument14 pagesSchizophr Bull 2000 Garety 73 86CBTPoupalou VasileiaNo ratings yet
- Biological Psychology: ArticleinfoDocument15 pagesBiological Psychology: ArticleinfoManuela SilvaNo ratings yet
- Behaviour Research and TherapyDocument8 pagesBehaviour Research and TherapyEl Andy de LongNo ratings yet
- Jurnal Psikiatri 3Document6 pagesJurnal Psikiatri 3LannydchandraNo ratings yet
- 2.psilocybin-Assisted Therapy For Depression A Systematic Review and Dose-Response Meta-Analysis of Human StudiesDocument16 pages2.psilocybin-Assisted Therapy For Depression A Systematic Review and Dose-Response Meta-Analysis of Human StudiesMarcos MouraNo ratings yet
- DownloadDocument5 pagesDownloadSreyoshi Roy ChowdhuryNo ratings yet
- Kelley RA 97Document10 pagesKelley RA 97Mihaela GhermanNo ratings yet
- Cognitive Difusion GADDocument16 pagesCognitive Difusion GADalvarogmc02100% (1)
- Comparing Mindfulness Based Cognitive THDocument5 pagesComparing Mindfulness Based Cognitive THolgasacristan316No ratings yet
- Research PaperDocument10 pagesResearch PaperJan LAWNo ratings yet
- 2014 - Keller - Depression Sudden GainsDocument19 pages2014 - Keller - Depression Sudden GainsMarinaNo ratings yet
- Meditation With Yoga, Group Therapy With Hypnosis, and Psychoeducation For Long-Term Depressed Mood: A Randomized Pilot TrialDocument16 pagesMeditation With Yoga, Group Therapy With Hypnosis, and Psychoeducation For Long-Term Depressed Mood: A Randomized Pilot TrialAnonymous 6h9W2AeSCNo ratings yet
- The Mental Mirror: Reflections on Psychiatry: Beyond the Looking Glass: The Enigmatic Odyssey of the MindFrom EverandThe Mental Mirror: Reflections on Psychiatry: Beyond the Looking Glass: The Enigmatic Odyssey of the MindNo ratings yet
- Designing Things Together - Intersections of Co-Design and Actor-Network TheoryDocument4 pagesDesigning Things Together - Intersections of Co-Design and Actor-Network TheoryMatt AldridgeNo ratings yet
- Buddhist Ayurvedic Therapy (BAT) in The NHS - Article Published by The Ayurveda Professionals AssociationDocument8 pagesBuddhist Ayurvedic Therapy (BAT) in The NHS - Article Published by The Ayurveda Professionals AssociationMatt AldridgeNo ratings yet
- Disengaged BuddhismDocument53 pagesDisengaged BuddhismMatt AldridgeNo ratings yet
- Buddhist-Derived Loving-Kindness and Compassion Meditation For The Treatment of Psychopathology - A Systematic ReviewDocument20 pagesBuddhist-Derived Loving-Kindness and Compassion Meditation For The Treatment of Psychopathology - A Systematic ReviewMatt AldridgeNo ratings yet
- Repentance in Chinese Buddhism - Implications For Mental Health ProfessionalsDocument26 pagesRepentance in Chinese Buddhism - Implications For Mental Health ProfessionalsMatt AldridgeNo ratings yet
- An Interview With Richard Dawkins PDFDocument1 pageAn Interview With Richard Dawkins PDFMatt AldridgeNo ratings yet
- Emotional Rescue - The Heart-Brain ConnectionDocument9 pagesEmotional Rescue - The Heart-Brain ConnectionMatt AldridgeNo ratings yet
- Scientific Background of Healthy and Nutritious FoodDocument8 pagesScientific Background of Healthy and Nutritious FoodMatt AldridgeNo ratings yet
- Encyclopaedic Dictionary of Yoga PDFDocument1 pageEncyclopaedic Dictionary of Yoga PDFMatt AldridgeNo ratings yet
- User-Centered Design in Developing CountriesDocument5 pagesUser-Centered Design in Developing CountriesMatt AldridgeNo ratings yet
- Ayurvedic Management of AchalasiaDocument6 pagesAyurvedic Management of AchalasiaMatt AldridgeNo ratings yet
- Buddhist Philosophy - A Historical Analysis PDFDocument1 pageBuddhist Philosophy - A Historical Analysis PDFMatt AldridgeNo ratings yet
- Ventilation Health Guide COVID 19Document25 pagesVentilation Health Guide COVID 19Carlos Valle TurciosNo ratings yet
- Jurnal HiperbilirubinemiaDocument5 pagesJurnal HiperbilirubinemiaWahyumi AmboahaNo ratings yet
- Sequalae of Wearing Complete DenturesDocument34 pagesSequalae of Wearing Complete DenturesAyeshaAslamNo ratings yet
- IvabradineDocument30 pagesIvabradinepashaNo ratings yet
- Dempul Epoxy 11-MSDSDocument3 pagesDempul Epoxy 11-MSDSAdam SuryaNo ratings yet
- A Client With Cushing's Syndrome: Nursing Care PlanDocument1 pageA Client With Cushing's Syndrome: Nursing Care PlanJulius Caesar ColladoNo ratings yet
- Opt WorkshopDocument15 pagesOpt WorkshopMhel Daz BabaysonNo ratings yet
- OTPeopleParkinsons PDFDocument84 pagesOTPeopleParkinsons PDFNovoNo ratings yet
- LP 20 Health Q3Document8 pagesLP 20 Health Q3Hazel Rubas SamsonNo ratings yet
- RRL ScriptDocument1 pageRRL Scriptjeron encaboNo ratings yet
- Nursing TherapyDocument121 pagesNursing TherapyIra AarisNo ratings yet
- Stem Cells Word Search 11-14Document1 pageStem Cells Word Search 11-14AnimeOtaku GirlNo ratings yet
- Branch Retinal Vein Occlusion (BRVO) : How Does BRVO Occur?Document3 pagesBranch Retinal Vein Occlusion (BRVO) : How Does BRVO Occur?merizNo ratings yet
- Kindergarten Physical Education LessonDocument7 pagesKindergarten Physical Education Lessonapi-185987237No ratings yet
- Brochure ISDocument4 pagesBrochure ISJAYESH VIKRAM RastogiNo ratings yet
- Vaccination Lesson PlanDocument2 pagesVaccination Lesson Planapi-517831630No ratings yet
- QMDocument12 pagesQMGs AbhilashNo ratings yet
- Priyanka Sen Final Practice School Internship ReportDocument35 pagesPriyanka Sen Final Practice School Internship ReportThakur Aditya PratapNo ratings yet
- Bed Bathing A PatientDocument5 pagesBed Bathing A PatientsalmaisazbouredNo ratings yet
- BMC Paediatric Department Guidelines 2011Document73 pagesBMC Paediatric Department Guidelines 2011Lexis SanchizieNo ratings yet
- MSDS of Rosuvastatin Calcium PDFDocument6 pagesMSDS of Rosuvastatin Calcium PDFSoheil JafariNo ratings yet
- Jaundice: From Superstition To ScienceDocument93 pagesJaundice: From Superstition To ScienceDr Muhammad ShoyabNo ratings yet
- Mental Health LetterDocument2 pagesMental Health LetterBethanyNo ratings yet
- Basic First Aid & CPR - A Guide: Indian Association of Occupational Health (IAOH)Document6 pagesBasic First Aid & CPR - A Guide: Indian Association of Occupational Health (IAOH)Sandeep KumarNo ratings yet
- Lung Cap DataDocument1 pageLung Cap DataKaren NelsonNo ratings yet