You might also like
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Pharma Mcq'sDocument47 pagesPharma Mcq'ssimi yNo ratings yet
- IIMA Casebook 2nd EditionDocument101 pagesIIMA Casebook 2nd Editionmanav fakey100% (2)
- Burton's Microbiology For The Health Sciences: Chapter 18. Viral InfectionsDocument20 pagesBurton's Microbiology For The Health Sciences: Chapter 18. Viral Infectionsmirai desu100% (1)
- Genetics in OrthoDocument58 pagesGenetics in OrthoAthira JithendranathNo ratings yet
- Protein SynthesisDocument29 pagesProtein SynthesisEugenia Migranova100% (9)
- Infections During PregnancyDocument9 pagesInfections During PregnancyKarina Madriaga100% (4)
- WTTH - Multidrug Resistant Urinary Tract Infection in A Dog 33066 ArticleDocument5 pagesWTTH - Multidrug Resistant Urinary Tract Infection in A Dog 33066 ArticleCabinet VeterinarNo ratings yet
- Small Animal/ExoticsDocument4 pagesSmall Animal/Exoticstaner_soysurenNo ratings yet
- Fistula THDocument3 pagesFistula THKatarina SimicicNo ratings yet
- Drug Study: Jocelyn Jacosalem DiagnosisDocument3 pagesDrug Study: Jocelyn Jacosalem DiagnosisMichelleNo ratings yet
- Cix 652Document3 pagesCix 652Rhea UyNo ratings yet
- Drug Study on Ampicillin's Uses, Side Effects and Nursing ResponsibilitiesDocument9 pagesDrug Study on Ampicillin's Uses, Side Effects and Nursing ResponsibilitiesMontero, Ma. Cecilia - BSN 3-BNo ratings yet
- Amoxi Tabs PDFDocument1 pageAmoxi Tabs PDFSubhrashis Guha NiyogiNo ratings yet
- Description of AntibacterialDocument102 pagesDescription of AntibacterialChristopher SongoroNo ratings yet
- AmoxicillinDocument4 pagesAmoxicillinJuliandri JNo ratings yet
- HBS Block 9-1Document15 pagesHBS Block 9-1Irfan AlemiNo ratings yet
- HT Emergencies FinalDocument1 pageHT Emergencies Finalsubha95No ratings yet
- Activity No. 9: Name: Lacastesantos, Bryan E. Course and Section: BSN 1-1EDocument4 pagesActivity No. 9: Name: Lacastesantos, Bryan E. Course and Section: BSN 1-1EKeen Jude CaminosNo ratings yet
- Eficacia Terapéutica Del Orbifloxacino de La Pioderma Canina: Un Estudio Clínico AbiertoDocument4 pagesEficacia Terapéutica Del Orbifloxacino de La Pioderma Canina: Un Estudio Clínico AbiertoscribdmanNo ratings yet
- Pharmacology, Biochemistry and Behavior: H.F. Miranda, V. Noriega, F. Sierralta, J.C. PrietoDocument5 pagesPharmacology, Biochemistry and Behavior: H.F. Miranda, V. Noriega, F. Sierralta, J.C. PrietoJuani Arcos OlivaresNo ratings yet
- Briefcommunications: A Clinical Drug Library Screen Identifies Astemizole As An Antimalarial AgentDocument14 pagesBriefcommunications: A Clinical Drug Library Screen Identifies Astemizole As An Antimalarial AgentLISSETH ALEJANDRA MEJÍA GÓMEZNo ratings yet
- Empiric Therapy: An SEO-Optimized Title for Antimicrobial TherapyDocument3 pagesEmpiric Therapy: An SEO-Optimized Title for Antimicrobial Therapyرجمه ديوانNo ratings yet
- 5drug StudyDocument7 pages5drug StudyPALEN, DONNA GRACE B.No ratings yet
- The Comparative Arthropathy of Uoroquinolones in DogsDocument8 pagesThe Comparative Arthropathy of Uoroquinolones in DogsNayra Cristina Herreira do ValleNo ratings yet
- Chronic Generalized Dermatophilosis in A BuffaloDocument3 pagesChronic Generalized Dermatophilosis in A BuffaloHendroNo ratings yet
- Drug Study 4Document5 pagesDrug Study 4Saito SanNo ratings yet
- Oxymetholone Therapy: in Aplastic AnemiaDocument8 pagesOxymetholone Therapy: in Aplastic AnemiaUrsus BarriosNo ratings yet
- 5 Cefuroxime Drug StudyDocument4 pages5 Cefuroxime Drug Studyshadow gonzalezNo ratings yet
- Shell Rot Infection in Red Eared Turtle: August 2017Document3 pagesShell Rot Infection in Red Eared Turtle: August 2017dwi putriNo ratings yet
- Managing Bronchodilator Therapy for Reversible Airway ObstructionDocument17 pagesManaging Bronchodilator Therapy for Reversible Airway ObstructionBea Marie A. ValdezNo ratings yet
- Traditional Chinese Herbal Treatment For Chronic Rhinitis in A CatDocument8 pagesTraditional Chinese Herbal Treatment For Chronic Rhinitis in A CatvillindaNo ratings yet
- Doerr BI 1982Document6 pagesDoerr BI 1982reclinpharmaNo ratings yet
- 1a Antiinfective DrugsDocument4 pages1a Antiinfective DrugsMaria Donabella OngueNo ratings yet
- Name: Ma Rupina B. Ponce Course: Bachelor of Science Major in Nursing Section: CDocument10 pagesName: Ma Rupina B. Ponce Course: Bachelor of Science Major in Nursing Section: CMaria Pina Barbado PonceNo ratings yet
- 10 Kinds of Antibacterial For PigsDocument3 pages10 Kinds of Antibacterial For PigsAustin DrykeNo ratings yet
- Case Based Learning Antimicrobials 05-12-2023Document50 pagesCase Based Learning Antimicrobials 05-12-2023aditya.3757No ratings yet
- Art 20632Document3 pagesArt 20632Monyet...No ratings yet
- Drugsstudy Different ObDocument8 pagesDrugsstudy Different ObElvis DuotNo ratings yet
- Yokenella Regensburgei Infection in India Mimicking Enteric FeverDocument5 pagesYokenella Regensburgei Infection in India Mimicking Enteric FeverKevin Fabricio Pichucho MusoNo ratings yet
- 9421329Document2 pages9421329tinahra1992No ratings yet
- Infestation of Oxyuris Equi in Horse and Its Successful Therapeutic ManagementDocument3 pagesInfestation of Oxyuris Equi in Horse and Its Successful Therapeutic Managementdh---pNo ratings yet
- Gastrointestinal Pro Kinetic Therapy-Motilin-Like DrugsDocument6 pagesGastrointestinal Pro Kinetic Therapy-Motilin-Like Drugstaner_soysurenNo ratings yet
- Surgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Document7 pagesSurgical Correction of Idiopathic Megacolon in Cats: Feline Practice January 1992Ayu DinaNo ratings yet
- Cheilitis Granulomatosa of Melkersson-Rosenthal Syndrome: Treatment With Intralesional Corticosteroid InjectionsDocument3 pagesCheilitis Granulomatosa of Melkersson-Rosenthal Syndrome: Treatment With Intralesional Corticosteroid InjectionsTatiana OrdoñezNo ratings yet
- 2017 - (69) Herrera-Uso Del Toxoide BotrópicoDocument5 pages2017 - (69) Herrera-Uso Del Toxoide BotrópicoClaudio ArceNo ratings yet
- Vulvovaginitis in CowDocument3 pagesVulvovaginitis in CowSbastian PratamaNo ratings yet
- The Use of Antihistamines in ChildrenDocument5 pagesThe Use of Antihistamines in ChildrenJin SniperNo ratings yet
- Hutchings 2019Document9 pagesHutchings 2019nabilahNo ratings yet
- Jurnal NexgardDocument5 pagesJurnal NexgardadelliaputryNo ratings yet
- Antihistamine On ChildrenDocument10 pagesAntihistamine On ChildrenOpl OplNo ratings yet
- CE Forceris Art N4 LRDocument7 pagesCE Forceris Art N4 LRLài LêNo ratings yet
- Veterinary Antimicrobial DrugsDocument5 pagesVeterinary Antimicrobial DrugsLaureece Salm ApduhanNo ratings yet
- 48-Published Paper (Mazhar Et Al) PDFDocument5 pages48-Published Paper (Mazhar Et Al) PDFmakram_0451No ratings yet
- Anaplasmosis in A Malabari Goat - TPIDocument3 pagesAnaplasmosis in A Malabari Goat - TPIDeepak CNo ratings yet
- Various Animal Models For Preclinical Testing of Anti-Inflammatory AgentsDocument8 pagesVarious Animal Models For Preclinical Testing of Anti-Inflammatory AgentsDrShailesh Madhukar KewatkarNo ratings yet
- Treatment of Larva Migrans Syndrome With Long-Term Administration of AlbendazoleDocument6 pagesTreatment of Larva Migrans Syndrome With Long-Term Administration of AlbendazoleSartika Ayu NingsihNo ratings yet
- Hookworms (Human and Zoonotic)Document5 pagesHookworms (Human and Zoonotic)Kyaru FuentesNo ratings yet
- The Effect of Enro Oxacin On Sperm Quality in Male Mice: Faruk Aral, Fu Sun Karac Al, Fu Sun BabaDocument5 pagesThe Effect of Enro Oxacin On Sperm Quality in Male Mice: Faruk Aral, Fu Sun Karac Al, Fu Sun BabaSueNo ratings yet
- Final RheaDocument5 pagesFinal RheaRhealyn LegaspiNo ratings yet
- Bayer 3rd Proc'99 - HEINENDocument7 pagesBayer 3rd Proc'99 - HEINENsergioNo ratings yet
- Allergy: Adverse Reaction To DextromethorphanDocument3 pagesAllergy: Adverse Reaction To DextromethorphanAdina SerbanNo ratings yet
- Villamaria - Drug StudyDocument11 pagesVillamaria - Drug StudyHey LeunNo ratings yet
- poster CUVC ӦFCөDCөE7өE4ӦEEDocument1 pageposter CUVC ӦFCөDCөE7өE4ӦEEJuan PérezNo ratings yet
- Bronchodilator Effect of Alcoholic Extract of Euphorbia Hirta LinnDocument5 pagesBronchodilator Effect of Alcoholic Extract of Euphorbia Hirta LinnKATHLEEN MAY BARRILNo ratings yet
- The Principal Diseases of Lower VertebratesFrom EverandThe Principal Diseases of Lower VertebratesRating: 5 out of 5 stars5/5 (1)
- Q1. Gender: Male Female OtherDocument5 pagesQ1. Gender: Male Female OtherArima ChatterjeeNo ratings yet
- 6 Brands That Are Building Social Movements: Lena Roland Source: Warc Opinion, Lena RolandDocument4 pages6 Brands That Are Building Social Movements: Lena Roland Source: Warc Opinion, Lena RolandArima ChatterjeeNo ratings yet
- Strategic Themes in Food and Nutrition: Coronavirus Update: September 2020Document34 pagesStrategic Themes in Food and Nutrition: Coronavirus Update: September 2020Arima ChatterjeeNo ratings yet
- A New View On The Market For Protein BarsDocument25 pagesA New View On The Market For Protein BarsArima ChatterjeeNo ratings yet
- How Covid-19 Is Shaping The Snacks Market in IndiaDocument13 pagesHow Covid-19 Is Shaping The Snacks Market in IndiaArima ChatterjeeNo ratings yet
- American Bar Association Antitrust Law JournalDocument11 pagesAmerican Bar Association Antitrust Law JournalArima ChatterjeeNo ratings yet
- Financial Habits: 21st Century Jam Jar Banking: Crawford Hollingworth Source: The Behavioural Architects, January 2015Document11 pagesFinancial Habits: 21st Century Jam Jar Banking: Crawford Hollingworth Source: The Behavioural Architects, January 2015Arima ChatterjeeNo ratings yet
- Biscuits and Snack BarsDocument2 pagesBiscuits and Snack BarsArima ChatterjeeNo ratings yet
- Nestlé Ok Nestlé Tell Me More AbDocument10 pagesNestlé Ok Nestlé Tell Me More AbArima ChatterjeeNo ratings yet
- Nielsen Featured Insights - Biting Into The Indian Snacking MarketDocument8 pagesNielsen Featured Insights - Biting Into The Indian Snacking MarketSamyak Spartacus JainNo ratings yet
- Demographic Profile India 2016 UpdatedDocument2 pagesDemographic Profile India 2016 UpdatedArima ChatterjeeNo ratings yet
- Name of Range One Liner Value Proposition Nutrition & Indulgence in A Crunch Category Locally Sourced: Vocal For LocalDocument3 pagesName of Range One Liner Value Proposition Nutrition & Indulgence in A Crunch Category Locally Sourced: Vocal For LocalArima ChatterjeeNo ratings yet
- The Big 15: Strategies and Priorities of Top Packaged Food Players in ComparisonDocument35 pagesThe Big 15: Strategies and Priorities of Top Packaged Food Players in ComparisonArima ChatterjeeNo ratings yet
- Effective Content Strategy Report Lessons From The 2019 WARC AwardsDocument36 pagesEffective Content Strategy Report Lessons From The 2019 WARC AwardsArima ChatterjeeNo ratings yet
- Twix A Tale of Two Bars - How STDocument19 pagesTwix A Tale of Two Bars - How STArima ChatterjeeNo ratings yet
- Ad AnalysisDocument4 pagesAd AnalysisArima ChatterjeeNo ratings yet
- Case WorkshopDocument26 pagesCase WorkshopAnonymous 6evPjkcE67% (3)
- New Text DocumentDocument2 pagesNew Text DocumentArima ChatterjeeNo ratings yet
- Market Entry Strategy For Nivea Face Was PDFDocument28 pagesMarket Entry Strategy For Nivea Face Was PDFJammigumpula PriyankaNo ratings yet
- Ad Analysis - QuestionsDocument9 pagesAd Analysis - QuestionsArima ChatterjeeNo ratings yet
- Case Approach Crasher: Market Entry Strategy For Renault DusterDocument27 pagesCase Approach Crasher: Market Entry Strategy For Renault DusterArima Chatterjee100% (1)
- Marketing Prep MFDocument31 pagesMarketing Prep MFArima ChatterjeeNo ratings yet
- Marketing PrepDocument521 pagesMarketing PrepArima ChatterjeeNo ratings yet
- GTM PrimerDocument2 pagesGTM PrimerArima ChatterjeeNo ratings yet
- New Text DocumentDocument1 pageNew Text DocumentArima ChatterjeeNo ratings yet
- ICT ICT Sadman SBM SBM Lunch OFD Dcci LSCM Dcci OFD Sadman LSCMDocument1 pageICT ICT Sadman SBM SBM Lunch OFD Dcci LSCM Dcci OFD Sadman LSCMArima ChatterjeeNo ratings yet
- 01 Summarized Kotler PDFDocument26 pages01 Summarized Kotler PDFMridulJainNo ratings yet
- Biochemistry and Medical Genetics: VideosDocument10 pagesBiochemistry and Medical Genetics: VideosRicardo ColomaNo ratings yet
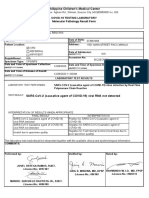
- Philippine Children's Medical Center: Covid-19 Testing Laboratory Molecular Pathology Result FormDocument1 pagePhilippine Children's Medical Center: Covid-19 Testing Laboratory Molecular Pathology Result FormRica RegorisNo ratings yet
- Phylogenetic Project PowerpointDocument16 pagesPhylogenetic Project PowerpointBryan ThompsonNo ratings yet
- Histology BloodDocument6 pagesHistology BloodNeneng Cutin GanzonNo ratings yet
- Harnessing Nature's Germ Killer: HOClDocument4 pagesHarnessing Nature's Germ Killer: HOClrizki yuliani100% (1)
- The GP Note 2020Document306 pagesThe GP Note 2020firdauseahNo ratings yet
- Laboratory Testing For COVID-19 - Dr. Trilis Yulianti, M.kesDocument20 pagesLaboratory Testing For COVID-19 - Dr. Trilis Yulianti, M.kesYayax RakhmanNo ratings yet
- Pathophysiology of DementiaDocument3 pagesPathophysiology of DementiaIvy NNo ratings yet
- Defense Against Infectious Disease: Skin As A Barrier To InfectionDocument8 pagesDefense Against Infectious Disease: Skin As A Barrier To InfectionFranchesca Rosabel BudimanNo ratings yet
- Dimension Xpand Plus/Rxl Max Integrated Chemistry Systems: Global Test MenuDocument2 pagesDimension Xpand Plus/Rxl Max Integrated Chemistry Systems: Global Test Menujyoti ranjanNo ratings yet
- Protective Effects of Blue Light-Blocking Shades On Phototoxicity in Human Ocular Surface CellsDocument6 pagesProtective Effects of Blue Light-Blocking Shades On Phototoxicity in Human Ocular Surface CellsHans Steven KurniawanNo ratings yet
- Reflection 1Document2 pagesReflection 1azuitazoolkiflieNo ratings yet
- Hepatitis Virus, Liver Cirrhosis and Hepatoma (HCCDocument61 pagesHepatitis Virus, Liver Cirrhosis and Hepatoma (HCCYun ZhaNo ratings yet
- Anatomy and Physiology ReviewerDocument10 pagesAnatomy and Physiology ReviewerMae Christelle FigueroaNo ratings yet
- What Are Vectors?Document4 pagesWhat Are Vectors?Shay HarrisonNo ratings yet
- Hofmann 1998Document8 pagesHofmann 1998Sarly FebrianaNo ratings yet
- Identification of BacteriaDocument29 pagesIdentification of BacteriaRavi KoppoluNo ratings yet
- Cytometry Part B Clinical - 2007 - Wood - 2006 Bethesda International Consensus Recommendations On The ImmunophenotypicDocument10 pagesCytometry Part B Clinical - 2007 - Wood - 2006 Bethesda International Consensus Recommendations On The ImmunophenotypicAzaelBermudesTorresNo ratings yet
- B2 UNITS 5 and 6 CLIL Teacher's NotesDocument1 pageB2 UNITS 5 and 6 CLIL Teacher's NotesNuria GLNo ratings yet
- ch.3 Genetics BIO SL NOTESDocument70 pagesch.3 Genetics BIO SL NOTESkhyati manglaniNo ratings yet
- Multiple Dengue Virus Types Harbored by Individual MosquitoesDocument7 pagesMultiple Dengue Virus Types Harbored by Individual MosquitoesYL Slalu BahagieaNo ratings yet
- Bio-Energetic Frequency ChartsDocument37 pagesBio-Energetic Frequency ChartsHayden JamesNo ratings yet
- Amino Acid 2Document6 pagesAmino Acid 2Princess Janine CatralNo ratings yet
- Bone and Cartilage PDFDocument50 pagesBone and Cartilage PDFalviraNo ratings yet
- Multidrug Resistant Gram Negative BacteriaDocument6 pagesMultidrug Resistant Gram Negative BacteriaAniAliciaOrtizCastleNo ratings yet
- Isbn6641-4 EG 19-01Document4 pagesIsbn6641-4 EG 19-01Dewi Puspita ApsariNo ratings yet