You might also like
- Psoriatic arthritis: causes, symptoms and treatmentDocument6 pagesPsoriatic arthritis: causes, symptoms and treatmentAndu1991No ratings yet
- Come Back To Your Senses Use Your Body: Psychologyt LsDocument1 pageCome Back To Your Senses Use Your Body: Psychologyt LsMarina Moran100% (1)
- Ats, TT, Tig: Anti Tetanus Serum, Tetanus Toxoid, Tetanus Immuno-GlobulinDocument15 pagesAts, TT, Tig: Anti Tetanus Serum, Tetanus Toxoid, Tetanus Immuno-Globulinjisoo100% (2)
- Hand Conditions and Examinations: a Rheumatologic and Orthopaedic ApproachFrom EverandHand Conditions and Examinations: a Rheumatologic and Orthopaedic ApproachNo ratings yet
- By Kerri Rivera, Kimberly Mcdaniel and Daniel Bender: Healing The Symptoms Known As Autism Second EditionDocument24 pagesBy Kerri Rivera, Kimberly Mcdaniel and Daniel Bender: Healing The Symptoms Known As Autism Second EditionMarilen De Leon EbradaNo ratings yet
- Understanding Osteoarthritis: Causes, Symptoms, Diagnosis and TreatmentDocument18 pagesUnderstanding Osteoarthritis: Causes, Symptoms, Diagnosis and Treatmentikram hanafiNo ratings yet
- Conveying Water Distribution SEODocument90 pagesConveying Water Distribution SEOmichelghanemNo ratings yet
- A Regional Approach To Foot and Ankle MRIDocument17 pagesA Regional Approach To Foot and Ankle MRInior100% (1)
- MKSAP 15 RheumatologyDocument177 pagesMKSAP 15 Rheumatologyfelipepatagon100% (2)
- Nestle Write UpDocument18 pagesNestle Write UpAnjana CarriNo ratings yet
- Approach To Arthritis: Clinical GuideDocument4 pagesApproach To Arthritis: Clinical GuideaveekumbharNo ratings yet
- SWRO-200C Operation Manual AppendicesDocument38 pagesSWRO-200C Operation Manual AppendicestonbaldinNo ratings yet
- POTT's DiseaseDocument3 pagesPOTT's DiseaseFema Jill AtrejenioNo ratings yet
- SACROILIITISDocument13 pagesSACROILIITISRiana KhairaniNo ratings yet
- API 578 Mock QuestionDocument4 pagesAPI 578 Mock QuestionsheikmoinNo ratings yet
- Osteoarthritis: OsteoartriteDocument9 pagesOsteoarthritis: OsteoartriteSofia Cerezo MuñozNo ratings yet
- Refrat PsoriaticDocument15 pagesRefrat PsoriaticnadddNo ratings yet
- Rheumatoid Arthritis Module IDocument14 pagesRheumatoid Arthritis Module ISamhitha Ayurvedic ChennaiNo ratings yet
- UW Radiology: Axial ArthritisDocument24 pagesUW Radiology: Axial Arthritisskype72214No ratings yet
- Septic Arthritis of The Wrist ENGDocument11 pagesSeptic Arthritis of The Wrist ENGInce NurfiantyNo ratings yet
- Case Psoriatic ArthritisDocument5 pagesCase Psoriatic ArthritisAyuNo ratings yet
- Jact13i2p154 Arya Osteoarthritis of The Knee Joint An OverviewDocument9 pagesJact13i2p154 Arya Osteoarthritis of The Knee Joint An OverviewErwynk EriantoNo ratings yet
- Acutely Swollen JointDocument7 pagesAcutely Swollen JointHossein VakiliNo ratings yet
- Knee Osteoarthritis: DefinitionDocument19 pagesKnee Osteoarthritis: DefinitionShrouq BadrNo ratings yet
- Krakowski 2018Document10 pagesKrakowski 2018Nguyễn Công LýNo ratings yet
- Radiologic Mimics of Juvenile RheumatoidDocument12 pagesRadiologic Mimics of Juvenile RheumatoidHosne araNo ratings yet
- Good Reliability Questionable Validity O20170518 3475 Qhxhhe With Cover Page v2Document183 pagesGood Reliability Questionable Validity O20170518 3475 Qhxhhe With Cover Page v2Ary MfNo ratings yet
- Septic Arthritis UpgradedDocument47 pagesSeptic Arthritis UpgradedVishva Randhara AllesNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument29 pagesDr. Ali's Uworld Notes For Step 2 CKuyes100% (1)
- Ankylosing Spondylitis and Undifferentiated SpondyloarthropathyDocument33 pagesAnkylosing Spondylitis and Undifferentiated Spondyloarthropathylbc-602No ratings yet
- Apyogenous Arthritis: Department of Orthopaedics The First Affiliated Hospital Dalian Medical University Tang KaiDocument131 pagesApyogenous Arthritis: Department of Orthopaedics The First Affiliated Hospital Dalian Medical University Tang KaiFathimathNo ratings yet
- Osteoid Osteoma: BackgroundDocument11 pagesOsteoid Osteoma: BackgroundputriNo ratings yet
- Ankylosing Spondylitis Diagnosis with RadiographyDocument6 pagesAnkylosing Spondylitis Diagnosis with RadiographychrisantyNo ratings yet
- Osteoarthritis Guide: Causes, Symptoms, TreatmentsDocument3 pagesOsteoarthritis Guide: Causes, Symptoms, TreatmentsFrancisco Palma CarvajalNo ratings yet
- Arthroscopic Debridement and Drilling of Osteochondral Lesions of The TalusDocument15 pagesArthroscopic Debridement and Drilling of Osteochondral Lesions of The TalusAnonymous kdBDppigENo ratings yet
- Inflammatory Joint Diseases Handout-Admission ExamDocument11 pagesInflammatory Joint Diseases Handout-Admission ExamNona NadimNo ratings yet
- Rheumatoid ArthritisDocument5 pagesRheumatoid ArthritisValerrie NgenoNo ratings yet
- Calcific Tendinitis of The Rotator Cuff State of The Art in Diagnosis PDFDocument8 pagesCalcific Tendinitis of The Rotator Cuff State of The Art in Diagnosis PDFItai IzhakNo ratings yet
- Current Concepts in Diagnosing and Treating Extra-Articular Hip ImpingementDocument8 pagesCurrent Concepts in Diagnosing and Treating Extra-Articular Hip ImpingementClaudio NogueiraNo ratings yet
- Clinical Manifestations and Diagnosis of OsteoarthritisDocument25 pagesClinical Manifestations and Diagnosis of OsteoarthritisjaquimqNo ratings yet
- عرض تقديمي 28Document33 pagesعرض تقديمي 28saifmajidhammadiNo ratings yet
- Jurnal Artritis PDFDocument8 pagesJurnal Artritis PDFbella faniaNo ratings yet
- Differential Polyarthritis: Diagnosis ofDocument5 pagesDifferential Polyarthritis: Diagnosis ofKaran ChauhanNo ratings yet
- AR - Clínica y LaboratorioDocument8 pagesAR - Clínica y LaboratoriomonseibanezbarraganNo ratings yet
- Osteoarthritis Patient ProfilesDocument12 pagesOsteoarthritis Patient Profilesifa afifahNo ratings yet
- Septic Arthritis NAC OSCEDocument11 pagesSeptic Arthritis NAC OSCEngoc nhan nguyen thiNo ratings yet
- Acute Dislocation of The PatellaDocument17 pagesAcute Dislocation of The PatellaChEko SpaguettyNo ratings yet
- Anterior Knee Pain in The Young AthleteDocument7 pagesAnterior Knee Pain in The Young AthleteAngelica GarciaNo ratings yet
- A 05 Suppl3 015Document5 pagesA 05 Suppl3 015Ashwath NarayanNo ratings yet
- Ki 1.1 Rotator Cuff Any 2 ASDocument29 pagesKi 1.1 Rotator Cuff Any 2 ASAgus TianyNo ratings yet
- IV Drug User's Septic ArthritisDocument53 pagesIV Drug User's Septic ArthritisAde Cahyo IslamiNo ratings yet
- Imaging of the Charcot Foot: Diagnosis Through ModalitiesDocument12 pagesImaging of the Charcot Foot: Diagnosis Through ModalitiesRajan PatelNo ratings yet
- Knee Disorders of The Inert Structures Capsular and Non-Capsular PatternsDocument16 pagesKnee Disorders of The Inert Structures Capsular and Non-Capsular PatternsFrankChenNo ratings yet
- عرض تقديمي 28Document33 pagesعرض تقديمي 28saifmajidhammadiNo ratings yet
- Killinger 2010Document8 pagesKillinger 2010Andrea TixeNo ratings yet
- Christopher W. DiGiovanni ArticleDocument10 pagesChristopher W. DiGiovanni ArticleRajiv NegandhiNo ratings yet
- Diagnostics 12 00618Document9 pagesDiagnostics 12 00618macox77No ratings yet
- Learning Issues FanyDocument3 pagesLearning Issues Fanyfaridatul jannahNo ratings yet
- Charcot foot imaging reviewDocument8 pagesCharcot foot imaging reviewAtika SugiartoNo ratings yet
- Spondyloarthritis: by Aishwarya Prasad Roll No 6Document22 pagesSpondyloarthritis: by Aishwarya Prasad Roll No 6irsyadilfikriNo ratings yet
- RheumatoidDocument26 pagesRheumatoidArja' WaasNo ratings yet
- Osteoarthritis of The Hip: Clinical PracticeDocument9 pagesOsteoarthritis of The Hip: Clinical PracticeMarina Tomasenco - DaniciNo ratings yet
- Common Rheumatologic Disease (Reichel's)Document9 pagesCommon Rheumatologic Disease (Reichel's)AhmedNo ratings yet
- Manifestaciones Clinicas de OsteoartritisDocument10 pagesManifestaciones Clinicas de OsteoartritisMeny GarciaNo ratings yet
- C PPPP "P P PP# PDocument11 pagesC PPPP "P P PP# PLeni CarununganNo ratings yet
- Osteoarthritis of The KneeDocument8 pagesOsteoarthritis of The Kneeas3syamut649250% (2)
- Atlas 5 AñosDocument10 pagesAtlas 5 AñosLeonardo GarciaNo ratings yet
- Cambios Radiograficos de Aps BJM 2005Document4 pagesCambios Radiograficos de Aps BJM 2005Leonardo GarciaNo ratings yet
- Aps Ustekinumab Falla TNFDocument10 pagesAps Ustekinumab Falla TNFLeonardo GarciaNo ratings yet
- Aps Etiologia PatogenesisDocument21 pagesAps Etiologia PatogenesisLeonardo GarciaNo ratings yet
- Aps y Ea Medicion ActividadDocument18 pagesAps y Ea Medicion ActividadLeonardo GarciaNo ratings yet
- Aps ApremilatsDocument7 pagesAps ApremilatsLeonardo GarciaNo ratings yet
- Aps ArticulacionDocument6 pagesAps ArticulacionLeonardo GarciaNo ratings yet
- Aps Tto 2015Document9 pagesAps Tto 2015Leonardo GarciaNo ratings yet
- Ateroesclerosis Sublcinica Ar RomanDocument8 pagesAteroesclerosis Sublcinica Ar RomanLeonardo GarciaNo ratings yet
- PSA Escalas de MediciónDocument22 pagesPSA Escalas de MediciónLeonardo GarciaNo ratings yet
- HypopituitarismoDocument4 pagesHypopituitarismoLeonardo GarciaNo ratings yet
- Copd Review 2002 ChestDocument8 pagesCopd Review 2002 ChestLeonardo GarciaNo ratings yet
- Copd Elderly ChestDocument12 pagesCopd Elderly ChestLeonardo GarciaNo ratings yet
- Guidelines For Management of Severe Sepsis and Septic ShockDocument2 pagesGuidelines For Management of Severe Sepsis and Septic ShockasupicuNo ratings yet
- Thai Occupational Safety, Health and Environment Act B.E. 2554 (A.d. 2011)Document32 pagesThai Occupational Safety, Health and Environment Act B.E. 2554 (A.d. 2011)DibbaSotaNanaNo ratings yet
- Market ReseachDocument3 pagesMarket ReseachSam Cy PuyalesNo ratings yet
- PCOS Diet Cookbook For Newly Diagnosed IndividualsDocument67 pagesPCOS Diet Cookbook For Newly Diagnosed Individualsmavendave4lifeNo ratings yet
- Miller Toyota-Conversion-Kit Letter ENG WEBDocument4 pagesMiller Toyota-Conversion-Kit Letter ENG WEBskyduckNo ratings yet
- Sulaiman Al Qudaibi Co.: Medium Term (1000 H) Hydrostatic Pressure Survival Test ProcedureDocument8 pagesSulaiman Al Qudaibi Co.: Medium Term (1000 H) Hydrostatic Pressure Survival Test ProcedureNADEEM AHMEDNo ratings yet
- Test A: Reading - Passage 1Document29 pagesTest A: Reading - Passage 1barishyayNo ratings yet
- Healthy Lifestyle HabitsDocument2 pagesHealthy Lifestyle HabitsJesus BaldeonNo ratings yet
- Polythionic Acid Stress Corrosion CrackingDocument2 pagesPolythionic Acid Stress Corrosion CrackingVajid MadathilNo ratings yet
- Providing Shelter and Safety: A Proposed Evacuation and Rehabilitation Center for Masbate CityDocument62 pagesProviding Shelter and Safety: A Proposed Evacuation and Rehabilitation Center for Masbate CityBenjamae MaqueNo ratings yet
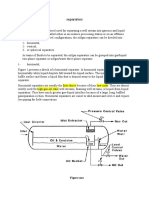
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- 2.factory Price - Alarm Accessories-Complete 20150325Document15 pages2.factory Price - Alarm Accessories-Complete 20150325FREE BUSINESS INTELLIGENCENo ratings yet
- CH 2Document20 pagesCH 2Vivek SinghNo ratings yet
- Fermentation Technology for Food Preservation and ProcessingDocument47 pagesFermentation Technology for Food Preservation and ProcessingAhmad Syamil Muhamad ZinNo ratings yet
- RESOLUTION 2022-08 Denial of Setback VarianceDocument5 pagesRESOLUTION 2022-08 Denial of Setback VarianceMatt McKinneyNo ratings yet
- Operator Manual For Respons920 With ISE - v2016.02Document358 pagesOperator Manual For Respons920 With ISE - v2016.02Juan Pablo CondoriNo ratings yet
- Concrete's enormous role in world's longest sea bridgeDocument3 pagesConcrete's enormous role in world's longest sea bridgeRafiath SiraNo ratings yet
- Trangia Worksheet IntroDocument2 pagesTrangia Worksheet Introjames.mccooeyNo ratings yet
- Glover 6e - Chapter 02Document41 pagesGlover 6e - Chapter 02JIGNESH DESAINo ratings yet
- Different Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowDocument6 pagesDifferent Surgical Modalities For Management of Postburn FL Exion Contracture of The ElbowMadhuchandra HirehalliNo ratings yet
- Tap ChangerDocument5 pagesTap ChangerRavindra AngalNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- Roof Construction Dr. Fixit Newcoat PDFDocument1 pageRoof Construction Dr. Fixit Newcoat PDFRishabh VijayNo ratings yet
- Mcimt NDT Kids at 1Document12 pagesMcimt NDT Kids at 1api-485106673No ratings yet