You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Personal Data SheetDocument4 pagesPersonal Data SheetLeonil Estaño100% (7)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Laboratory Methods of Identification of Entamoeba Histolytica and Its Differentiation From Look-Alike Entamoeba SPPDocument8 pagesLaboratory Methods of Identification of Entamoeba Histolytica and Its Differentiation From Look-Alike Entamoeba SPPCedrickNo ratings yet
- ChatDocument3 pagesChatCedrickNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Schmidt Proteomicsb 2002Document29 pagesSchmidt Proteomicsb 2002CedrickNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
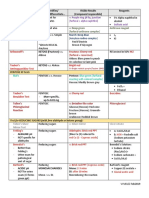
- ID Test Tabular Reviewer For Philippine PLE Module 2Document3 pagesID Test Tabular Reviewer For Philippine PLE Module 2ViaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- History of Medical Technology Education in The PhilippinesDocument45 pagesHistory of Medical Technology Education in The PhilippinesCedrickNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
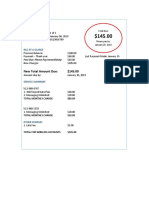
- Sample BillDocument1 pageSample BillCedrickNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Station Licensing 2018 (Receiving Copy)Document1 pageStation Licensing 2018 (Receiving Copy)CedrickNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Amino AnalysisDocument8 pagesAmino AnalysisVignesh ReddyNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- PBCC Seminar Registration FormDocument1 pagePBCC Seminar Registration FormCedrickNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Laboratory Department: Supplies / Reagents PriceDocument3 pagesLaboratory Department: Supplies / Reagents PriceCedrickNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Questions (MedTech Undergrad)Document3 pagesQuestions (MedTech Undergrad)CedrickNo ratings yet
- 2.1 Mission, Vision, Objective and ValuesDocument1 page2.1 Mission, Vision, Objective and ValuesCedrickNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- CPAP 423 Research ProjectDocument3 pagesCPAP 423 Research ProjectCedrickNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- CPAP (Parasitology)Document2 pagesCPAP (Parasitology)CedrickNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Our Lady of Fatima University College of Medical Laboratory ScienceDocument1 pageOur Lady of Fatima University College of Medical Laboratory ScienceCedrickNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Generalised Ultimate Loads For Pile GroupsDocument22 pagesGeneralised Ultimate Loads For Pile GroupsValerioNo ratings yet
- Strategi Meningkatkan Kapasitas Penangkar Benih Padi Sawah (Oriza Sativa L) Dengan Optimalisasi Peran Kelompok TaniDocument24 pagesStrategi Meningkatkan Kapasitas Penangkar Benih Padi Sawah (Oriza Sativa L) Dengan Optimalisasi Peran Kelompok TaniHilmyTafantoNo ratings yet
- Applications of Remote Sensing and Gis For UrbanDocument47 pagesApplications of Remote Sensing and Gis For UrbanKashan Ali KhanNo ratings yet
- Araldite 2020 + XW 396 - XW 397Document6 pagesAraldite 2020 + XW 396 - XW 397Paul Dan OctavianNo ratings yet
- Homework 1 Tarea 1Document11 pagesHomework 1 Tarea 1Anette Wendy Quipo Kancha100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Phrasal Verbs en Inglés.Document2 pagesPhrasal Verbs en Inglés.David Alexander Palomo QuirozNo ratings yet
- Nationalisation of Insurance BusinessDocument12 pagesNationalisation of Insurance BusinessSanjay Ram Diwakar50% (2)
- Balkhu Squatter SettlementDocument10 pagesBalkhu Squatter SettlementShramina ShresthaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Miso Soup Miso Soup Miso Soup: Ingredients Ingredients IngredientsDocument8 pagesMiso Soup Miso Soup Miso Soup: Ingredients Ingredients IngredientsEllie M.No ratings yet
- Calculating Measures of Position Quartiles Deciles and Percentiles of Ungrouped DataDocument43 pagesCalculating Measures of Position Quartiles Deciles and Percentiles of Ungrouped DataRea Ann ManaloNo ratings yet
- Simple Fat Burning Exercises at Home or GymDocument6 pagesSimple Fat Burning Exercises at Home or GymShirleyNo ratings yet
- DWDMDocument41 pagesDWDMKarthik KompelliNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Student's T DistributionDocument6 pagesStudent's T DistributionNur AliaNo ratings yet
- Topics For AssignmentDocument2 pagesTopics For AssignmentniharaNo ratings yet
- Yusuf Mahmood CVDocument3 pagesYusuf Mahmood CVapi-527941238No ratings yet
- FloodDocument9 pagesFloodapi-352767278No ratings yet
- The Morning Calm Korea Weekly - August 22,2008Document24 pagesThe Morning Calm Korea Weekly - August 22,2008Morning Calm Weekly NewspaperNo ratings yet
- E34-1 Battery Charging and Dishcharging BoardDocument23 pagesE34-1 Battery Charging and Dishcharging BoardGanesa MurthyNo ratings yet
- Finite Element Method For Eigenvalue Problems in ElectromagneticsDocument38 pagesFinite Element Method For Eigenvalue Problems in ElectromagneticsBhargav BikkaniNo ratings yet
- Form IEPF 2 - 2012 2013FDocument2,350 pagesForm IEPF 2 - 2012 2013FYam ServínNo ratings yet
- RAMSCRAM-A Flexible RAMJET/SCRAMJET Engine Simulation ProgramDocument4 pagesRAMSCRAM-A Flexible RAMJET/SCRAMJET Engine Simulation ProgramSamrat JanjanamNo ratings yet
- Lite Indicator Admin ManualDocument16 pagesLite Indicator Admin Manualprabakar070No ratings yet
- Veris Case StudyDocument2 pagesVeris Case StudyPankaj GargNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Inkolo Namasiko Kuyamakha Umuntu - Brainly - inDocument1 pageInkolo Namasiko Kuyamakha Umuntu - Brainly - inxqxfkqpy5qNo ratings yet
- Topics For Oral PresentationDocument6 pagesTopics For Oral PresentationMohd HyqalNo ratings yet
- Topic 3 - Analyzing The Marketing EnvironmentDocument28 pagesTopic 3 - Analyzing The Marketing Environmentmelissa chlNo ratings yet
- DS WhitePaper Troubleshooting 3DEXPERIENCE ABEND SituationsDocument26 pagesDS WhitePaper Troubleshooting 3DEXPERIENCE ABEND SituationsSam AntonyNo ratings yet
- New Python Basics AssignmentDocument5 pagesNew Python Basics AssignmentRAHUL SONI0% (1)
- Research Article: Dynamic Modelling of A Solar Water Pumping System With Energy StorageDocument13 pagesResearch Article: Dynamic Modelling of A Solar Water Pumping System With Energy Storagehabtamu melsewNo ratings yet
- MCQs + SEQs Medical Physics Midterm Exam Paper-Fall 2020Document3 pagesMCQs + SEQs Medical Physics Midterm Exam Paper-Fall 2020Ali Nouman100% (1)
- A Series of Fortunate Events: Chance and the Making of the Planet, Life, and YouFrom EverandA Series of Fortunate Events: Chance and the Making of the Planet, Life, and YouRating: 4.5 out of 5 stars4.5/5 (62)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)