You might also like
- Oracle Forms Developer 10G Student Guide - 1Document440 pagesOracle Forms Developer 10G Student Guide - 1Jayant Agarwal100% (3)
- Investingunplugged PDFDocument225 pagesInvestingunplugged PDFWilliam MercerNo ratings yet
- Health 10 Performance TaskDocument4 pagesHealth 10 Performance TaskMary Kryss DG SangleNo ratings yet
- ETL Process in Data WarehouseDocument40 pagesETL Process in Data WarehouseshariqatariqNo ratings yet
- A Quick Guide To The FMD Pro PDFDocument24 pagesA Quick Guide To The FMD Pro PDFstouraNo ratings yet
- Treatment of Acute Viral Bronchiolitis: Ernst EberDocument6 pagesTreatment of Acute Viral Bronchiolitis: Ernst EberDyah Gaby KesumaNo ratings yet
- Bronchiolitis: Dr. Mustafa Mohamed Ahmed MBBS, MDDocument37 pagesBronchiolitis: Dr. Mustafa Mohamed Ahmed MBBS, MDYuusuf MubarikNo ratings yet
- Ibvt13i10p939Document11 pagesIbvt13i10p939David CraigNo ratings yet
- Special Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisDocument11 pagesSpecial Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisyundaNo ratings yet
- 2009 30 386 Tamara Wagner: Pediatrics in ReviewDocument12 pages2009 30 386 Tamara Wagner: Pediatrics in ReviewAlexandru CosminNo ratings yet
- Acute Bronchiolitis in Infants, A ReviewDocument10 pagesAcute Bronchiolitis in Infants, A ReviewDavid CraigNo ratings yet
- Acute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) NovemberDocument28 pagesAcute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) Novemberزكريا عمرNo ratings yet
- Bronquiolitis TXDocument36 pagesBronquiolitis TXDauris garcia diazNo ratings yet
- Blush 2012 Acute Bronchitis PDFDocument7 pagesBlush 2012 Acute Bronchitis PDFMarimar FilardoNo ratings yet
- BronchioitisDocument24 pagesBronchioitismitiku aberaNo ratings yet
- Diagnosis and Treatment of BronchiectasisDocument12 pagesDiagnosis and Treatment of Bronchiectasissunaryo lNo ratings yet
- Respiratory InfectionsDocument15 pagesRespiratory Infectionsnishi kNo ratings yet
- Tratamiento RinosinusitisDocument10 pagesTratamiento RinosinusitisrrrocafuNo ratings yet
- The Syndrome We Agreed To Call Bronchiolitis: PerspectiveDocument3 pagesThe Syndrome We Agreed To Call Bronchiolitis: PerspectiveaqilaNo ratings yet
- BronkiektasisDocument7 pagesBronkiektasisirenaNo ratings yet
- Fulltext Ajeccm v4 Id1053Document8 pagesFulltext Ajeccm v4 Id1053Killua X ZaoldyeckNo ratings yet
- Duke 2019Document3 pagesDuke 2019Diego AndradeNo ratings yet
- PDF DocumentDocument44 pagesPDF DocumentBintangemonNo ratings yet
- Bronchiolitis in Infants and Children - Treatment, Outcome, and Prevention - UpToDateDocument25 pagesBronchiolitis in Infants and Children - Treatment, Outcome, and Prevention - UpToDateAlejandra AubadNo ratings yet
- Final IntroductionDocument6 pagesFinal IntroductionFloramae LosaritaNo ratings yet
- Effectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisDocument9 pagesEffectiveness of thoracic-abdominal rebalancing technique for acute viral bronchiolitisrebeca paulinoNo ratings yet
- Bronchiolitis Guideline RecommendationsDocument10 pagesBronchiolitis Guideline RecommendationsAmi WilliamsNo ratings yet
- Diagnosing Bronchiectasis: An Overlooked DiseaseDocument6 pagesDiagnosing Bronchiectasis: An Overlooked DiseasefallenczarNo ratings yet
- Nursing-Management A Respriotry Syncytial Bronchiolitis PDFDocument7 pagesNursing-Management A Respriotry Syncytial Bronchiolitis PDFAdarsh MuniNo ratings yet
- Management of recurrent preschool wheezeDocument9 pagesManagement of recurrent preschool wheezecarlaNo ratings yet
- Diagnosis and Treatment of BronchiectasisDocument12 pagesDiagnosis and Treatment of Bronchiectasisrichie_ciandraNo ratings yet
- Rhinopharyngeal Retrograde Clearance Induces Less Respiratory Effort and Fewer Adverse Effects in Comparison With Nasopharyngeal Aspiration in Infants With Acute Viral BronchiolitisDocument7 pagesRhinopharyngeal Retrograde Clearance Induces Less Respiratory Effort and Fewer Adverse Effects in Comparison With Nasopharyngeal Aspiration in Infants With Acute Viral Bronchiolitismariane bezerraNo ratings yet
- Acute Bronchitis - StatPearls - NCBI BookshelfDocument7 pagesAcute Bronchitis - StatPearls - NCBI BookshelfnurulishtimalNo ratings yet
- Early Human Development: A. Nicolai, M. Ferrara, C. Schiavariello, F. Gentile, M.E. Grande, C. Alessandroni, F. MidullaDocument5 pagesEarly Human Development: A. Nicolai, M. Ferrara, C. Schiavariello, F. Gentile, M.E. Grande, C. Alessandroni, F. MidullalalaNo ratings yet
- Community-acquired bacterial pneumonia in children....Document6 pagesCommunity-acquired bacterial pneumonia in children....MariaNo ratings yet
- Pediatric Lower Respiratory InfectionsDocument27 pagesPediatric Lower Respiratory InfectionsAzmachamberAzmacareNo ratings yet
- Primer: BronchiectasisDocument18 pagesPrimer: BronchiectasisAnanta Bryan Tohari WijayaNo ratings yet
- CAP Guidelines SA 2020Document22 pagesCAP Guidelines SA 2020kudzaimuregidubeNo ratings yet
- Children 08 00066 PDFDocument12 pagesChildren 08 00066 PDFVanessa RomeroNo ratings yet
- Bronquiolitis IIDocument48 pagesBronquiolitis IIISABELA GUEVARA ESPAÑANo ratings yet
- Journal Reading ParuDocument53 pagesJournal Reading ParuDaniel IvanNo ratings yet
- Bronchiolitis PDFDocument5 pagesBronchiolitis PDFjuniorebindaNo ratings yet
- Recommendation 1ADocument26 pagesRecommendation 1Asyahrizon thomasNo ratings yet
- Jurnal Cahaya InternasionalDocument9 pagesJurnal Cahaya InternasionalCahaya YusmaniNo ratings yet
- 04 Acute Bronchitis and Pneumonia in ChildrenDocument58 pages04 Acute Bronchitis and Pneumonia in ChildrenMi PatelNo ratings yet
- Bronchiolitis Rs V Current Concepts 2009Document75 pagesBronchiolitis Rs V Current Concepts 2009adnan.engineer17049No ratings yet
- CDC 8044 DS1Document8 pagesCDC 8044 DS1immanueldioNo ratings yet
- Acute Rhinosinusitis New GuidelinesDocument3 pagesAcute Rhinosinusitis New GuidelinesJuan Carlos Soria MaturinoNo ratings yet
- BPJ 45 Pneumonia Pages 25-29Document5 pagesBPJ 45 Pneumonia Pages 25-29Festijo , KennethNo ratings yet
- Recurrent croup diagnosis and managementDocument7 pagesRecurrent croup diagnosis and managementNadaNo ratings yet
- QCO.0000000000000357Document5 pagesQCO.0000000000000357Monica Aleja FernándezNo ratings yet
- Neumonia Complicada PDFDocument9 pagesNeumonia Complicada PDFadriana gallardoNo ratings yet
- CharacterisationDocument11 pagesCharacterisationDesti Oki LestariNo ratings yet
- Neumonía en niños_ tratamiento hospitalario - UpToDateDocument42 pagesNeumonía en niños_ tratamiento hospitalario - UpToDatepao.pearanda1998No ratings yet
- Acute Bronchitis in Adults - UpToDateDocument41 pagesAcute Bronchitis in Adults - UpToDateEnrique Vazquez RodriguezNo ratings yet
- Nac 2017Document18 pagesNac 2017Nataly CortesNo ratings yet
- Sinusitis: Effects of The Traditional Mediterranean Diet in Childhood Recurrent Acute RhinosinusitisDocument15 pagesSinusitis: Effects of The Traditional Mediterranean Diet in Childhood Recurrent Acute RhinosinusitisGeko AndikaNo ratings yet
- Pneumonia Pada Kasus PediatrikDocument41 pagesPneumonia Pada Kasus PediatrikasriNo ratings yet
- Lower Respiratory Tract Infections (Lrtis) BronchitisDocument11 pagesLower Respiratory Tract Infections (Lrtis) BronchitisAhmed Gh Al-zechrawiNo ratings yet
- Ventilator Associated Pneumonia in ChildrenDocument7 pagesVentilator Associated Pneumonia in ChildrendarlingcarvajalduqueNo ratings yet
- Acute Sinusitis in AdultsDocument9 pagesAcute Sinusitis in AdultsAndika Anjani AgustinNo ratings yet
- IJTLDeditorial Protecting HCworkers Form TBDocument2 pagesIJTLDeditorial Protecting HCworkers Form TBRoma ParyaniNo ratings yet
- 742 FullDocument2 pages742 FullveliiiNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- A Study On Childhood Development in Early Stage: October 2020Document13 pagesA Study On Childhood Development in Early Stage: October 2020Ariel BobisNo ratings yet
- 81 FullDocument15 pages81 Fulltessa wulandariNo ratings yet
- Can Low Vision Aids Improve The Quality of Life of Low Vision PatientsDocument4 pagesCan Low Vision Aids Improve The Quality of Life of Low Vision Patientstessa wulandariNo ratings yet
- Scala 2018Document4 pagesScala 2018Andi sutandiNo ratings yet
- Low Vision AaoDocument51 pagesLow Vision Aaotessa wulandariNo ratings yet
- Glaucoma GuidelinesDocument28 pagesGlaucoma GuidelinesRina RostianaNo ratings yet
- 81 FullDocument15 pages81 Fulltessa wulandariNo ratings yet
- The Treatment of Acute Bronchiolitis: Past, Present and FutureDocument4 pagesThe Treatment of Acute Bronchiolitis: Past, Present and Futuretessa wulandariNo ratings yet
- Hospital Care WHO Evidence 0Document176 pagesHospital Care WHO Evidence 0tessa wulandariNo ratings yet
- Acutebronchiolitisininfantsareview Oymar Skjerven MikalsenDocument11 pagesAcutebronchiolitisininfantsareview Oymar Skjerven Mikalsentessa wulandariNo ratings yet
- CPS-guidelines-bronchiolitis 2Document8 pagesCPS-guidelines-bronchiolitis 2tessa wulandariNo ratings yet
- Etiology of Acute Bronchiolitis and The RelationshDocument7 pagesEtiology of Acute Bronchiolitis and The Relationshtessa wulandariNo ratings yet
- Distribusi Nilai Pre TestDocument2 pagesDistribusi Nilai Pre Testtessa wulandariNo ratings yet
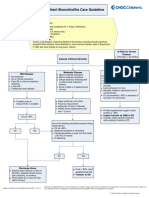
- Outpatient Bronchiolitis Care Guideline: Inclusion CriteriaDocument4 pagesOutpatient Bronchiolitis Care Guideline: Inclusion Criteriatessa wulandariNo ratings yet
- Alimentatia Copilului - OMSDocument112 pagesAlimentatia Copilului - OMSshugyosha77No ratings yet
- Practice Guidelines: ACOG Releases Clinical Guidelines On Management of Menopausal SymptomsDocument2 pagesPractice Guidelines: ACOG Releases Clinical Guidelines On Management of Menopausal Symptomstessa wulandariNo ratings yet
- Practice Guidelines: ACOG Releases Clinical Guidelines On Management of Menopausal SymptomsDocument2 pagesPractice Guidelines: ACOG Releases Clinical Guidelines On Management of Menopausal Symptomstessa wulandariNo ratings yet
- Acutebronchiolitisininfantsareview Oymar Skjerven MikalsenDocument11 pagesAcutebronchiolitisininfantsareview Oymar Skjerven Mikalsentessa wulandariNo ratings yet
- Bronchiolitis Peds.2014 2742.fullDocument32 pagesBronchiolitis Peds.2014 2742.fullTowhidulIslamNo ratings yet
- Beam Loader Tributary ExcelDocument2 pagesBeam Loader Tributary ExcelHari Amudhan IlanchezhianNo ratings yet
- Men S Health South Africa - March 2017 PDFDocument132 pagesMen S Health South Africa - March 2017 PDFAbimaelGomesNo ratings yet
- A Seminar Report On Floating Wind TurbineDocument26 pagesA Seminar Report On Floating Wind Turbinevaishakh123450% (6)
- Techspec XS enDocument2 pagesTechspec XS enpesumasinadNo ratings yet
- IELTS PART 1 (Autoguardado)Document8 pagesIELTS PART 1 (Autoguardado)CARLOS CAICEDONo ratings yet
- 20171121hulten JBS 6-3 PDFDocument13 pages20171121hulten JBS 6-3 PDFJe RomeNo ratings yet
- FoCal Multi-class Toolkit GuideDocument32 pagesFoCal Multi-class Toolkit Guidethyagosmesme100% (1)
- PowerShell Advanced Function Parameter AttributesDocument6 pagesPowerShell Advanced Function Parameter Attributesignacio fernandez luengoNo ratings yet
- LAS IN ENTREPRENEURSHIP WEEK 4Document5 pagesLAS IN ENTREPRENEURSHIP WEEK 4IMELDA CORONACIONNo ratings yet
- Haslinda Mohd Anuar Senior Lecturer School of Law ColgisDocument24 pagesHaslinda Mohd Anuar Senior Lecturer School of Law ColgisSHAHEERANo ratings yet
- Tesco AnalysisDocument12 pagesTesco Analysisdanny_wch7990No ratings yet
- Modeling Drop Structures in HEC-RAS 3.1Document29 pagesModeling Drop Structures in HEC-RAS 3.1reluNo ratings yet
- Cambridge IGCSE: PHYSICS 0625/62Document12 pagesCambridge IGCSE: PHYSICS 0625/62yuNo ratings yet
- Motor Vehicles and Road Traffic Regulation 48.50Document411 pagesMotor Vehicles and Road Traffic Regulation 48.50Clayton AllenNo ratings yet
- Study of Altman's Z ScoreDocument8 pagesStudy of Altman's Z ScoreKatarina JovanovićNo ratings yet
- Ivent201 - Manual de Usuario (220-290)Document71 pagesIvent201 - Manual de Usuario (220-290)Wilber AleluyaNo ratings yet
- Microeconomics Primer 1Document15 pagesMicroeconomics Primer 1md1sabeel1ansariNo ratings yet
- 410 09e Checkliste For Assessment 13485 MDDDocument51 pages410 09e Checkliste For Assessment 13485 MDDeko Setyawan100% (1)
- Capital Expenditure Decision Making ToolsDocument19 pagesCapital Expenditure Decision Making ToolsRoshan PoudelNo ratings yet
- The Threat Landscape Quiz ResultsDocument5 pagesThe Threat Landscape Quiz ResultsKaskusemail88 EmailNo ratings yet
- Special Power of Attorney for Overseas EmploymentDocument2 pagesSpecial Power of Attorney for Overseas EmploymentJakeLeonciniNo ratings yet
- NN43001-712 02.02 SwIOFAULTDocument2,474 pagesNN43001-712 02.02 SwIOFAULTJoeNo ratings yet
- ASME B16: Standardization of Valves, Flanges, Fittings, and Gaskets # Standard DesignationDocument6 pagesASME B16: Standardization of Valves, Flanges, Fittings, and Gaskets # Standard DesignationNicolás MerinoNo ratings yet
- SheetMetal Bend Allowance GuideDocument3 pagesSheetMetal Bend Allowance GuidesunilbholNo ratings yet
- Chapter 3 - Excel SolutionsDocument8 pagesChapter 3 - Excel SolutionsHalt DougNo ratings yet