You might also like
- Milady Standard Esthetics Advanced: Advanced Skin Care MassageDocument72 pagesMilady Standard Esthetics Advanced: Advanced Skin Care Massagechristina magallanesNo ratings yet
- Imci FormDocument3 pagesImci FormVon Jethro Palas100% (1)
- Case Presentation On Pre-EclampsiaDocument18 pagesCase Presentation On Pre-EclampsiaPabhat Kumar88% (8)
- Drugs Affecting The Cardiovascular SystemDocument27 pagesDrugs Affecting The Cardiovascular SystemCelestino Kuchena100% (3)
- Nursing Care Plan For Ineffective Tissue PerfusionDocument19 pagesNursing Care Plan For Ineffective Tissue Perfusionbrenhood78% (9)
- NCP For CHFDocument11 pagesNCP For CHFqingwen100% (5)
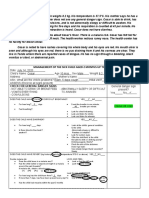
- Management of The Sick Child Aged 2 Months Up To 5 Years: Case#8: CesarDocument4 pagesManagement of The Sick Child Aged 2 Months Up To 5 Years: Case#8: CesarChloe MorningstarNo ratings yet
- Anti Infective AgentsDocument42 pagesAnti Infective AgentsDthird Mendoza ClaudioNo ratings yet
- Prepared By: Rashmi Regmi B. SC Nursing Manmohan Memorial Institute of Health SciencesDocument93 pagesPrepared By: Rashmi Regmi B. SC Nursing Manmohan Memorial Institute of Health SciencesNinaNo ratings yet
- Difficulty of BreathingDocument1 pageDifficulty of BreathingkingpinkNo ratings yet
- Stages of Labor Nursing Intervention: First StageDocument3 pagesStages of Labor Nursing Intervention: First StageJhanniel IreneaNo ratings yet
- Threatened Abortion ReportDocument8 pagesThreatened Abortion ReportMohamad RaisNo ratings yet
- Drug StudyDocument8 pagesDrug StudyJay-ar Batara SorianoNo ratings yet
- NCM106 Pharmacology - Module 1Document11 pagesNCM106 Pharmacology - Module 1Marco VillanuevaNo ratings yet
- Demography & Mortality Rates: by Dr. Muhammad Bilal ShahDocument39 pagesDemography & Mortality Rates: by Dr. Muhammad Bilal ShahmuhammadbilalshahNo ratings yet
- Pa Tho Physiology of RaDocument7 pagesPa Tho Physiology of Ralisalmar2008No ratings yet
- Perdido - Activity 1 Feeding Pregnant and Lactating WomenDocument4 pagesPerdido - Activity 1 Feeding Pregnant and Lactating WomenKariza Perdido100% (1)
- Imci ChartDocument26 pagesImci ChartDenise Espinosa100% (1)
- Drug Study For Multiple Sclerosis (Betaseron)Document4 pagesDrug Study For Multiple Sclerosis (Betaseron)Leslie Lagat PaguioNo ratings yet
- Drug StudyDocument16 pagesDrug Studyalice_lim01No ratings yet
- Case PresDocument100 pagesCase PresJoj BagnateNo ratings yet
- Nutrition Nursing: CarbohydratesDocument36 pagesNutrition Nursing: CarbohydratesAngelyka Nicole Bengco DavidNo ratings yet
- Reading and Understanding Nutrition LabelsDocument16 pagesReading and Understanding Nutrition Labelsapi-301586234100% (1)
- Drug StudyDocument7 pagesDrug StudyGladys NacionNo ratings yet
- Checklist - MseDocument2 pagesChecklist - MseAlessandra Dominique MarianoNo ratings yet
- BARANDINO, Jia Laurice (Gouty Arthritis)Document18 pagesBARANDINO, Jia Laurice (Gouty Arthritis)Deinielle Magdangal RomeroNo ratings yet
- CLUBFOOTDocument19 pagesCLUBFOOTKaryn Joy LamisNo ratings yet
- 2.3 HYPOCALCEMIA and HYPERCALCEMIADocument7 pages2.3 HYPOCALCEMIA and HYPERCALCEMIABooz Waief CaluzaNo ratings yet
- Nursing Care To Promote Fetal Maternal HealthDocument3 pagesNursing Care To Promote Fetal Maternal HealthLuna Sang-anNo ratings yet
- Laws Affecting Nursing PracticeDocument52 pagesLaws Affecting Nursing Practiceapi-3731845100% (3)
- Health Assessment ToolDocument3 pagesHealth Assessment ToolGail GenturalezNo ratings yet
- Newborn Journal PDFDocument8 pagesNewborn Journal PDFRose Ann ManalastasNo ratings yet
- Administering MedicationsDocument24 pagesAdministering MedicationsCharmie GandaNo ratings yet
- Case-Scenario-No-1-Shortness-of-Breath-CVS-1 - نسخةDocument2 pagesCase-Scenario-No-1-Shortness-of-Breath-CVS-1 - نسخةAseem AlrehiliNo ratings yet
- Tenofovir Disoproxil Fumarate: Therese M. Chapman, Jane K. Mcgavin and Stuart NobleDocument12 pagesTenofovir Disoproxil Fumarate: Therese M. Chapman, Jane K. Mcgavin and Stuart NobleBagusHibridaNo ratings yet
- HANDOUT Chapter 11 Promoting Fetal and Maternal HealthDocument7 pagesHANDOUT Chapter 11 Promoting Fetal and Maternal HealthClouiseNo ratings yet
- Widdoes ST., Brgy. II, City of San Fernando, La Union 2500 PhilippinesDocument7 pagesWiddoes ST., Brgy. II, City of San Fernando, La Union 2500 Philippinesricky torresNo ratings yet
- Neonatal SepsisDocument8 pagesNeonatal SepsisPrabiñKhadkaNo ratings yet
- 109lec Week 5Document16 pages109lec Week 5claire yowsNo ratings yet
- Gordons 11 Health Pattern Guide Format and Questions Converted 1Document11 pagesGordons 11 Health Pattern Guide Format and Questions Converted 1Kim BadillesNo ratings yet
- v3.PhilHealth Presentation For DepEd PRO III - 072619Document127 pagesv3.PhilHealth Presentation For DepEd PRO III - 072619Hazelle BondocNo ratings yet
- Far Eastern University: Institute of NursingDocument3 pagesFar Eastern University: Institute of Nursingshendae cosmianoNo ratings yet
- Pathophy NCADocument1 pagePathophy NCAKaren ValdezNo ratings yet
- HandwashingDocument6 pagesHandwashingKhemz Dalde Lim100% (1)
- GASTRITISDocument14 pagesGASTRITISRoyster CabralNo ratings yet
- NCM 109 MCN Semifinals Gestational ConditionsDocument6 pagesNCM 109 MCN Semifinals Gestational ConditionsQUEZON, BRITNEY KIM E.No ratings yet
- Sexually Transmitted InfectionsDocument34 pagesSexually Transmitted InfectionsMariana Creciun100% (1)
- Einc PDFDocument69 pagesEinc PDFIvan BibonNo ratings yet
- Burn - Daily Physical AssessmentDocument8 pagesBurn - Daily Physical AssessmentkrishcelNo ratings yet
- History and Physical Examination in Pediatrics (1) - 1Document44 pagesHistory and Physical Examination in Pediatrics (1) - 1okwadha simion100% (1)
- NCM 104 Cellular Aberration Lecture 2007Document104 pagesNCM 104 Cellular Aberration Lecture 2007Kris TejereroNo ratings yet
- Physical Evaluation Checklist For NurseDocument3 pagesPhysical Evaluation Checklist For NurseGiridhar RagavasimhanNo ratings yet
- 4 ConceptDocument1 page4 ConceptStacey GarciaNo ratings yet
- Pregestational ConditionsDocument46 pagesPregestational ConditionsSheryl M. Ablao50% (2)
- 8. Care of Child With GI Dysfunction (1) ءءءءDocument44 pages8. Care of Child With GI Dysfunction (1) ءءءءNuhaNo ratings yet
- Case in Herniorraphy BESTCASEDocument23 pagesCase in Herniorraphy BESTCASEAdrian MallarNo ratings yet
- Case StudyDocument8 pagesCase StudyJay-ann MendozaNo ratings yet
- Pharma RLE OverviewDocument10 pagesPharma RLE OverviewNathaniel PulidoNo ratings yet
- Case Presentation 12319Document52 pagesCase Presentation 12319Salazar DaisyNo ratings yet
- Management of The Sick Child Aged 2 Months Up To 5 Years: ASSESS (Circle All Signs Present) ClassifyDocument1 pageManagement of The Sick Child Aged 2 Months Up To 5 Years: ASSESS (Circle All Signs Present) ClassifyCooky JeonNo ratings yet
- Imci Recording Form 2Document3 pagesImci Recording Form 2Dea Sabelle Castro100% (1)
- Case Recording FormDocument8 pagesCase Recording FormNathaniel PulidoNo ratings yet
- Imci Forms GuideDocument2 pagesImci Forms GuideFhey Bernadette BeltranNo ratings yet
- ALO Case Report PDFDocument5 pagesALO Case Report PDFemma mojokertoNo ratings yet
- Study Guide 4 Resit Exm TerminologyDocument13 pagesStudy Guide 4 Resit Exm Terminologyapi-87967494No ratings yet
- Case: Liver Cirrhosis Assessment:: Nursing InferenceDocument7 pagesCase: Liver Cirrhosis Assessment:: Nursing InferenceLovelyn GanirNo ratings yet
- Silikonoma Bali JournalDocument7 pagesSilikonoma Bali JournaldanielNo ratings yet
- Paclitaxel HandoutDocument5 pagesPaclitaxel HandoutFikaNo ratings yet
- CASE STUDY (ABNORMAL PREGNANCY) .Edited (2)Document9 pagesCASE STUDY (ABNORMAL PREGNANCY) .Edited (2)niyoc68859No ratings yet
- Assessment - Case StudyDocument7 pagesAssessment - Case StudyEfrylrose CorderoCasayNo ratings yet
- Urino (Urine) Therapy AI Translated (G.P. Malakhov) (Z-Library)Document98 pagesUrino (Urine) Therapy AI Translated (G.P. Malakhov) (Z-Library)CeciliavasNo ratings yet
- Reviewer Chapter 35 MedicationsDocument4 pagesReviewer Chapter 35 MedicationsKeren GaciasNo ratings yet
- Pcol 2 LAB Activity 1 & 2 VIDEO TRANSCRIPTDocument5 pagesPcol 2 LAB Activity 1 & 2 VIDEO TRANSCRIPTMarecar VeniegasNo ratings yet
- Burns - Tissue Perfusion, IneffectiveDocument3 pagesBurns - Tissue Perfusion, Ineffectivemakyofrancis20100% (1)
- DM Foot 81Document20 pagesDM Foot 81Zar Ni OoNo ratings yet
- ACUTE INFLAMMATION (Vascular Changes)Document22 pagesACUTE INFLAMMATION (Vascular Changes)Ramesh KumarNo ratings yet
- Patient Interview Guide: Chief ComplaintDocument3 pagesPatient Interview Guide: Chief ComplaintR HariNo ratings yet
- The Causes of EdemaDocument3 pagesThe Causes of EdemaNUR ZAMZAM AZIZAHNo ratings yet
- TOPNOTCH Patho Supplement Handout For Sept 2018 UPDATED May 2018Document25 pagesTOPNOTCH Patho Supplement Handout For Sept 2018 UPDATED May 2018Waiwit KritayakiranaNo ratings yet
- IV TherapyDocument27 pagesIV TherapyTeresa Bellessa DiekmannNo ratings yet
- MassDocument8 pagesMassYara YousefNo ratings yet
- Head Injury Rupani3Document203 pagesHead Injury Rupani3Anonymous udSI3fQ5No ratings yet
- Pregnancy Induced Hypertension Nursing Diagnosis NANDADocument9 pagesPregnancy Induced Hypertension Nursing Diagnosis NANDASanal S SalimNo ratings yet
- UNIT 7 - Achievement TestDocument3 pagesUNIT 7 - Achievement TestHo Hong Gia HuyNo ratings yet
- Chapter 4Document34 pagesChapter 4Gwenilda Ma-aslum MabanaNo ratings yet
- Orthopedic Case Proformas-1Document19 pagesOrthopedic Case Proformas-1md maaz100% (1)
- Lymphedema: Pathogenesis and Novel Therapies: Annual Review of MedicineDocument14 pagesLymphedema: Pathogenesis and Novel Therapies: Annual Review of MedicineClaudia GutiérrezNo ratings yet
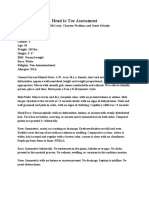
- Weebly Head To Toe AssessmentDocument3 pagesWeebly Head To Toe Assessmentapi-608265381No ratings yet
- DyspneuDocument9 pagesDyspneuAmy KochNo ratings yet