You might also like
- 2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRDocument2 pages2000 - Frankel - Re Radical Prostatectomy For Localized Prostate Cancer Provides Durable Cancer Control With Excellent Quality of Life A STRPoljarLijanNo ratings yet
- Retroperitoneal MassDocument22 pagesRetroperitoneal Massapi-434838777No ratings yet
- NIH Public Access: Author ManuscriptDocument10 pagesNIH Public Access: Author ManuscriptNurci Efrilia SafitriNo ratings yet
- A Pain in The Butt - A Case Series of Gluteal Compartment Syndrome - PMCDocument6 pagesA Pain in The Butt - A Case Series of Gluteal Compartment Syndrome - PMCchhabraanNo ratings yet
- Menyhei 1994Document4 pagesMenyhei 1994Anett Pappné LeppNo ratings yet
- CCR3-5-1210Document3 pagesCCR3-5-1210NovelNo ratings yet
- Myasthenic Crisis with Myxedema and Dual Antibody PositivityDocument4 pagesMyasthenic Crisis with Myxedema and Dual Antibody PositivityFitria ChandraNo ratings yet
- Tumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupDocument5 pagesTumor Necrosis Factor Inhibitors in Patients With Takayasu Arteritis: Experience From A Referral Center With Long-Term FollowupMikhail PisarevNo ratings yet
- Pain Management in Blast Crisis Patient Revision 2Document8 pagesPain Management in Blast Crisis Patient Revision 2CaseoulliNo ratings yet
- Good Book AcupunctureDocument9 pagesGood Book AcupunctureyusuftravellersNo ratings yet
- Childhood Membranoproliferative Glomerulonephritis Type I: Limited Steroid TherapyDocument7 pagesChildhood Membranoproliferative Glomerulonephritis Type I: Limited Steroid TherapyKiki Celiana TiffanyNo ratings yet
- Asymptomatic Aplastic Anemia Case Due to Anti-TB DrugsDocument4 pagesAsymptomatic Aplastic Anemia Case Due to Anti-TB DrugsayuNo ratings yet
- Hepatotoxicity Induced by High Dose of Methylprednisolone Therapy in A Patient With Multiple Sclerosis: A Case Report and Brief Review of LiteratureDocument5 pagesHepatotoxicity Induced by High Dose of Methylprednisolone Therapy in A Patient With Multiple Sclerosis: A Case Report and Brief Review of LiteratureBayu ParmikaNo ratings yet
- Torj 12 125Document4 pagesTorj 12 125Tya VenyNo ratings yet
- 1 s2.0 S1550830716301665 MainDocument7 pages1 s2.0 S1550830716301665 MainAwadAyoubNo ratings yet
- 1 s2.0 S1550830716301665 MainDocument7 pages1 s2.0 S1550830716301665 MainAwadAyoubNo ratings yet
- Patient Diagnosed With Myocardial Infarct M006Document11 pagesPatient Diagnosed With Myocardial Infarct M006Kefix WritersHubNo ratings yet
- Biologic Treatments in Takayasu's Arteritis: A Comparative Study of Tumor Necrosis Factor Inhibitors and TocilizumabDocument16 pagesBiologic Treatments in Takayasu's Arteritis: A Comparative Study of Tumor Necrosis Factor Inhibitors and TocilizumabAsad KakarNo ratings yet
- Rheumatoid Arthritis Case PresentationDocument18 pagesRheumatoid Arthritis Case Presentationapi-434838777No ratings yet
- HyperthyroidDocument7 pagesHyperthyroidHaerun Nisa SiregarNo ratings yet
- Klair 2014Document3 pagesKlair 2014PabloIgLopezNo ratings yet
- Journal of DiabetesDocument6 pagesJournal of DiabetesSartika Rizky HapsariNo ratings yet
- ASIA Syndrome Following Breast Implant Placement: Case CommunicationsDocument3 pagesASIA Syndrome Following Breast Implant Placement: Case Communicationssilvana31No ratings yet
- Preprint Not Peer ReviewedDocument21 pagesPreprint Not Peer ReviewedАмина ПлотноваNo ratings yet
- BPJ Vol 10 No 3 P 1369-1377Document9 pagesBPJ Vol 10 No 3 P 1369-1377citra annisa fitriNo ratings yet
- Management of Neoplastic Pericardial EffusionsDocument4 pagesManagement of Neoplastic Pericardial EffusionsMamamia DonchanNo ratings yet
- 1985 Myocarditis Related To Drug Hypersensitivity.Document6 pages1985 Myocarditis Related To Drug Hypersensitivity.dolemite4No ratings yet
- Tuberculosis: in Patients With ErythematosusDocument4 pagesTuberculosis: in Patients With ErythematosusHarsha CNo ratings yet
- Paediatric Tolosa-Hunt Syndrome: The Need For Treatment Guidelines and Renewed CriteriaDocument2 pagesPaediatric Tolosa-Hunt Syndrome: The Need For Treatment Guidelines and Renewed CriteriaRakasiwi GalihNo ratings yet
- Arthritis Drug Therapy May Cause Deadly Blood DisorderDocument5 pagesArthritis Drug Therapy May Cause Deadly Blood DisorderShaysta KhanNo ratings yet
- Atypical GPA Presentation with Interstitial NephritisDocument6 pagesAtypical GPA Presentation with Interstitial NephritisAdriana NicoletaNo ratings yet
- 10 Relato de Caso Acute CoronaryDocument4 pages10 Relato de Caso Acute CoronaryAsis FitrianaNo ratings yet
- Methimazole Drug Induced Agranulocytosis DefinitionDocument21 pagesMethimazole Drug Induced Agranulocytosis DefinitionReyza ReyzaNo ratings yet
- Bartter-like Syndrome Case Due to CapreomycinDocument6 pagesBartter-like Syndrome Case Due to Capreomycinbagir_dm10No ratings yet
- Case Study Internal MedDocument3 pagesCase Study Internal MedChibueze AfugbuomNo ratings yet
- 1 PBDocument3 pages1 PBMartynaNo ratings yet
- DR Eric Brestel's Sep 5 2000 Letter To EditorDocument2 pagesDR Eric Brestel's Sep 5 2000 Letter To EditorRobert Davidson, M.D., Ph.D.No ratings yet
- Seronegative Myasthenia Gravis Presenting With PneumoniaDocument4 pagesSeronegative Myasthenia Gravis Presenting With PneumoniaJ. Ruben HermannNo ratings yet
- Diabetes y Quistes RenalesDocument11 pagesDiabetes y Quistes RenalesJairo StragaNo ratings yet
- Pan 1Document3 pagesPan 1Mithun CbNo ratings yet
- Non-Operative Treatment For Compartment Syndrome With Phenylephrine and DobutamineDocument3 pagesNon-Operative Treatment For Compartment Syndrome With Phenylephrine and DobutaminehanananwarNo ratings yet
- 83-Article Text-163-1-10-20180209Document4 pages83-Article Text-163-1-10-20180209Grace Meigawati IwantoNo ratings yet
- A Rare Cause of AA Amyloidosis and End-Stage Kidney Failure: QuestionsDocument3 pagesA Rare Cause of AA Amyloidosis and End-Stage Kidney Failure: QuestionsSezen YılmazNo ratings yet
- Guidelines EuromyastheniaDocument4 pagesGuidelines Euromyastheniadokter mudaNo ratings yet
- Case Report: Osteomyelitis of The Patella in A 10-Year-Old Girl: A Case Report and Review of The LiteratureDocument6 pagesCase Report: Osteomyelitis of The Patella in A 10-Year-Old Girl: A Case Report and Review of The LiteratureIfal JakNo ratings yet
- SynapseDocument8 pagesSynapsePabloIgLopezNo ratings yet
- Chiang OWM FIR-vs.-TAODocument4 pagesChiang OWM FIR-vs.-TAOIsmah KhairinaNo ratings yet
- The Role of Peritoneal Ultrafiltration in The Treatment of Refractory Congestive Heart FailureDocument3 pagesThe Role of Peritoneal Ultrafiltration in The Treatment of Refractory Congestive Heart FailureM. Ryan RamadhanNo ratings yet
- Concise Report: Efficacy and Tolerance of Infliximab in Refractory Takayasu Arteritis: French Multicentre StudyDocument5 pagesConcise Report: Efficacy and Tolerance of Infliximab in Refractory Takayasu Arteritis: French Multicentre StudyMikhail PisarevNo ratings yet
- Cabot 2007Document10 pagesCabot 2007Luis Andres Villar InfanteNo ratings yet
- King 2012 4AP Toxicity ReviewDocument8 pagesKing 2012 4AP Toxicity ReviewzernebochNo ratings yet
- Paraneoplastic Syndrome Mimicking Adult-Onset Still 'S Disease Caused by Advanced Lung Cancer: A Case ReportDocument4 pagesParaneoplastic Syndrome Mimicking Adult-Onset Still 'S Disease Caused by Advanced Lung Cancer: A Case Reportoralposter PIPKRA2023No ratings yet
- Takeuchi 2018Document5 pagesTakeuchi 2018Hiba MardiniNo ratings yet
- Chelation of Gadolinium Oxford 2009Document3 pagesChelation of Gadolinium Oxford 2009gasfgdNo ratings yet
- Use of Oral Dichloroacetate For Palliation of Leg Pain Arising From Metastatic Poorly Differentiated Carcinoma: A Case ReportDocument6 pagesUse of Oral Dichloroacetate For Palliation of Leg Pain Arising From Metastatic Poorly Differentiated Carcinoma: A Case ReportCezary TomczykNo ratings yet
- S39 Summer 2013Document2 pagesS39 Summer 2013Puskesmas TanjungdurenselatanNo ratings yet
- 1899 FullDocument6 pages1899 Fullmelanita_99No ratings yet
- Metronidazole-Induced Encephalopathy in A Patient With Liver CirrhosisDocument4 pagesMetronidazole-Induced Encephalopathy in A Patient With Liver CirrhosisMudassar SattarNo ratings yet
- A Patient With Hypercoagulable State Due To TuberculosisDocument4 pagesA Patient With Hypercoagulable State Due To TuberculosisAnnisa SufiNo ratings yet
- Ipcr-Samillano, John Vanne D. Samillano, Rmt-MaayonDocument3 pagesIpcr-Samillano, John Vanne D. Samillano, Rmt-MaayonGeline Joy D. SamillanoNo ratings yet
- (Merge) Hepatitis C Virus HCV Test Report Format Example Sample Temp 20240101 141Document5 pages(Merge) Hepatitis C Virus HCV Test Report Format Example Sample Temp 20240101 141M ShafiqNo ratings yet
- Viral PathogenesisDocument8 pagesViral PathogenesisBiofilm NSTUNo ratings yet
- Clinical Review - KEDRABDocument97 pagesClinical Review - KEDRABcoolchapNo ratings yet
- Part 2 CD Mastery TestDocument12 pagesPart 2 CD Mastery TestRika MaeNo ratings yet
- CHICKEN POX Genesis CarandangDocument10 pagesCHICKEN POX Genesis CarandangGenEsis CarandangNo ratings yet
- Guillain Barre SyndromeDocument2 pagesGuillain Barre SyndromeTheresia Avila KurniaNo ratings yet
- Program Hivr4p2018Document90 pagesProgram Hivr4p2018jadwongscribdNo ratings yet
- 2020 Pharmacology & Therapeutics Pharmacological Targets and Emerging Treatments For Respiratory Syncytial Virus BronchiolitisDocument18 pages2020 Pharmacology & Therapeutics Pharmacological Targets and Emerging Treatments For Respiratory Syncytial Virus BronchiolitisMayra Concha OstosNo ratings yet
- Ucat SCMNS PDFDocument58 pagesUcat SCMNS PDFJohnNo ratings yet
- HEALTH FITNESS TESTS & STI SYMPTOMSDocument6 pagesHEALTH FITNESS TESTS & STI SYMPTOMSAimee HernandezNo ratings yet
- Biological Hazards: Health Hazards Associated With Exposure To Biological AgentsDocument42 pagesBiological Hazards: Health Hazards Associated With Exposure To Biological AgentsKate PagalingNo ratings yet
- GOKU-Rheumatology-SLE-OTHER-Connective Tissue Diseases and VasculitisDocument30 pagesGOKU-Rheumatology-SLE-OTHER-Connective Tissue Diseases and VasculitisCas BuNo ratings yet
- Updated Guidelines on Management of Animal Bite PatientsDocument15 pagesUpdated Guidelines on Management of Animal Bite PatientsKaren ArchesNo ratings yet
- March, To It Now Being The Vast Majority of Our Sequenced CasesDocument6 pagesMarch, To It Now Being The Vast Majority of Our Sequenced Cases01 LudviaNo ratings yet
- 0 CFC SFC MM Central C Yearend Evaluation 2021Document127 pages0 CFC SFC MM Central C Yearend Evaluation 2021STEVE JHONSON LepasanaNo ratings yet
- Selflearning Kit Blood and Its Components2019Document18 pagesSelflearning Kit Blood and Its Components2019Jeff Bryan Arellano HimorNo ratings yet
- Acute Otitis Media in Young Children - Diagnosis and MGT PDFDocument9 pagesAcute Otitis Media in Young Children - Diagnosis and MGT PDFdanny17phNo ratings yet
- JURNALDocument9 pagesJURNALagus nugrahaNo ratings yet
- ADA Cal en DT ADS001150 Rev01Document1 pageADA Cal en DT ADS001150 Rev01vijayramaswamyNo ratings yet
- The Flu - Expository EssayDocument2 pagesThe Flu - Expository EssaytessafikriNo ratings yet
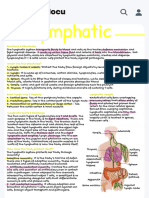
- Handwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuDocument1 pageHandwritten Lympathic - Functions & Structures The Lymphatic System Transports Fluids To Blood - StudocuAllyssa MarieNo ratings yet
- Red Blood Cells/Red Blood Corpuscles (RBC) : ErythrocytesDocument6 pagesRed Blood Cells/Red Blood Corpuscles (RBC) : ErythrocytesDeep RoyNo ratings yet
- BlepharitisDocument2 pagesBlepharitisAyu Anissa BahriNo ratings yet
- IntJYoga1245-2978617 081626Document11 pagesIntJYoga1245-2978617 081626panchagameNo ratings yet
- Sexually Transmitted DiseasesDocument29 pagesSexually Transmitted DiseasesDha DhaNo ratings yet
- Summary of Recommendations For Adult Immunization: (Age 19 Years & Older)Document4 pagesSummary of Recommendations For Adult Immunization: (Age 19 Years & Older)enquzerNo ratings yet
- Pus and WoundDocument16 pagesPus and WoundArmilyn Garcia NavarroNo ratings yet
- Acquired Immunodeficiency Syndrome Pediatric NursingDocument2 pagesAcquired Immunodeficiency Syndrome Pediatric Nursingjezreel tijingNo ratings yet
- Nutrition and Exercise ImmunologyDocument204 pagesNutrition and Exercise ImmunologytodayisnovemberNo ratings yet