You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fpgee Study Guide GurudattaDocument31 pagesFpgee Study Guide GurudattaWINSOMETAB33% (3)
- Steps of The Research ProcessDocument8 pagesSteps of The Research ProcessDee DiahNo ratings yet
- A Grammar of The Arabic LanguageDocument378 pagesA Grammar of The Arabic LanguagemanelaoNo ratings yet
- Clinical Application Meridian Diagnosis-FratkinDocument20 pagesClinical Application Meridian Diagnosis-Fratkinocoxodo100% (3)
- Analgesic Mechanism of Electroacupuncture in An Arthritic Pain Model of Rats: A Neurotransmitter StudyDocument6 pagesAnalgesic Mechanism of Electroacupuncture in An Arthritic Pain Model of Rats: A Neurotransmitter Studyocoxodo0% (1)
- Chapt 01Document12 pagesChapt 01ocoxodoNo ratings yet
- Treating Musculo-Skeletal Pain With Traditional Chinese MedicineDocument2 pagesTreating Musculo-Skeletal Pain With Traditional Chinese MedicineocoxodoNo ratings yet
- Measures A: J. B. P. StephensonDocument2 pagesMeasures A: J. B. P. StephensonocoxodoNo ratings yet
- Research Article: Effects of Electroacupuncture at BL60 On Formalin-Induced Pain in RatsDocument7 pagesResearch Article: Effects of Electroacupuncture at BL60 On Formalin-Induced Pain in RatsocoxodoNo ratings yet
- Some Common A: Acupuncture For Evaluative ResearchDocument5 pagesSome Common A: Acupuncture For Evaluative ResearchocoxodoNo ratings yet
- AnestesiaDocument4 pagesAnestesiaocoxodoNo ratings yet
- Chronic PainDocument13 pagesChronic PainocoxodoNo ratings yet
- Effect of Acupuncture Depth On Muscle Pain: Research Open AccessDocument5 pagesEffect of Acupuncture Depth On Muscle Pain: Research Open AccessocoxodoNo ratings yet
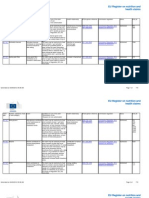
- Claims FoodDocument68 pagesClaims FoodocoxodoNo ratings yet
- Health ClaimsDocument719 pagesHealth ClaimsocoxodoNo ratings yet
- Document Code List For Uploading IcegateDocument5 pagesDocument Code List For Uploading IcegateRajesh GadaNo ratings yet
- AAOS Trauma 2018Document88 pagesAAOS Trauma 2018alealer2708No ratings yet
- AWWA B300 - 2011 HypochloritesDocument31 pagesAWWA B300 - 2011 HypochloritesestanilorenteNo ratings yet
- Ortodontic DentistryDocument5 pagesOrtodontic DentistryazdnonNo ratings yet
- Unscear 2016 ReportDocument512 pagesUnscear 2016 ReportKhairul Anuar AbdullahNo ratings yet
- Committees On Decentralisation (Government of India) : RecommendationsDocument92 pagesCommittees On Decentralisation (Government of India) : RecommendationsK Rajasekharan0% (1)
- Prevention - November 2016Document100 pagesPrevention - November 2016ARmani KhaledNo ratings yet
- Nursing ProcedureDocument240 pagesNursing ProcedurerainNo ratings yet
- Supernatural HealingDocument131 pagesSupernatural HealingKelvin Anthony OssaiNo ratings yet
- Effects of Geopathic Stress and VastuDocument12 pagesEffects of Geopathic Stress and VastuDeepak Singh RaghuvansheNo ratings yet
- Production RAF ReportDocument92 pagesProduction RAF ReportPrabhatNo ratings yet
- Sample ReflectionDocument2 pagesSample ReflectionRhiza Joy HiposNo ratings yet
- MUHAMMAD's Health Passport 26-04-2022Document1 pageMUHAMMAD's Health Passport 26-04-2022Asif KhanNo ratings yet
- COMD358 SunumuDocument29 pagesCOMD358 SunumuSerhan DağlıNo ratings yet
- Remote Control R/F System: DREX-W20PE8Document9 pagesRemote Control R/F System: DREX-W20PE8german.martinezd3528No ratings yet
- Sehat Nov 2022Document20 pagesSehat Nov 2022prolanis puskesmaskendal1No ratings yet
- 2023 Peterborough Regional Science Fair WinnersDocument125 pages2023 Peterborough Regional Science Fair WinnersPeterborough ExaminerNo ratings yet
- Problems & Management of Psycho-GeriatricsDocument39 pagesProblems & Management of Psycho-GeriatricsAnugrah Adiatmika0% (1)
- Tumor Targeting: Presented by M.Pharm 2 Semester (Pharmaceutics) Reg No. 121725101005Document41 pagesTumor Targeting: Presented by M.Pharm 2 Semester (Pharmaceutics) Reg No. 121725101005TridevNo ratings yet
- Dasar VentilatorDocument40 pagesDasar Ventilatorsingle_ladyNo ratings yet
- Non Specific DefenseDocument27 pagesNon Specific Defensededhi yustendi ternakNo ratings yet
- Infy Mock Test 07a Verbal FDocument7 pagesInfy Mock Test 07a Verbal FSaravana KarthikeyanNo ratings yet
- Analyzing Negative Experiences Without Ruminating The Role of Self-Distancing in Enabling Adaptive Self-ReflectionDocument14 pagesAnalyzing Negative Experiences Without Ruminating The Role of Self-Distancing in Enabling Adaptive Self-Reflection12traderNo ratings yet
- MC 2018-2157 Annex PDFDocument19 pagesMC 2018-2157 Annex PDFChristine Joy Mancha100% (1)
- Nijhuis Water Technology - Corporate BrochureDocument15 pagesNijhuis Water Technology - Corporate BrochureMark James AlburoNo ratings yet
- Imatinib - Drug Information PDFDocument20 pagesImatinib - Drug Information PDFabuzeid5No ratings yet
- RedactedDocument8 pagesRedactedChristina GiardinelliNo ratings yet
- Temas de Redaccion BachilleratoDocument7 pagesTemas de Redaccion BachilleratopatNo ratings yet