You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Animal TissueDocument32 pagesAnimal TissueIan Kerby Sollano100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Blood Bank Case 1 KeyDocument4 pagesBlood Bank Case 1 KeyGissele Palero75% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- THALASSEMIADocument33 pagesTHALASSEMIAMirzi Cuison100% (1)
- Techtalk August2010Document2 pagesTechtalk August2010Abu KhalidNo ratings yet
- Reviewer - Immunohematology - Part 1Document16 pagesReviewer - Immunohematology - Part 1Joshua TrinidadNo ratings yet
- Blood Banking and Serology and Immunology Refresher Exam With AnswersDocument8 pagesBlood Banking and Serology and Immunology Refresher Exam With AnswersJohn Rhel DenqueNo ratings yet
- Wwiy4300 PDFDocument6 pagesWwiy4300 PDFvenkat ramanaNo ratings yet
- 14 Anterolateral Thigh FlapDocument6 pages14 Anterolateral Thigh FlapAngga Putra100% (1)
- Advanced Anatomy Questions PDFDocument63 pagesAdvanced Anatomy Questions PDFJoanne BlancoNo ratings yet
- American Burn Association Practice GuidelinesDocument10 pagesAmerican Burn Association Practice GuidelinesJosé María Llerena Otiniano100% (1)
- Local Glutamine Metabolism in Wounds and Inflammation: Michael D. CaldwellDocument6 pagesLocal Glutamine Metabolism in Wounds and Inflammation: Michael D. CaldwellAngga PutraNo ratings yet
- Synchronous Premaxillary Osteotomy With Primary.5Document8 pagesSynchronous Premaxillary Osteotomy With Primary.5Angga PutraNo ratings yet
- Wound Healing Animal Kawasumi2012Document17 pagesWound Healing Animal Kawasumi2012Angga PutraNo ratings yet
- Amino Acid Supplementation and Impact OnDocument13 pagesAmino Acid Supplementation and Impact OnISABELNo ratings yet
- Acinobakter 222Document4 pagesAcinobakter 222Angga PutraNo ratings yet
- Efek Supplen GlutaminDocument13 pagesEfek Supplen GlutaminAngga PutraNo ratings yet
- IcvDocument1 pageIcvAngga PutraNo ratings yet
- Management of Pediatric Condyle FracturesDocument3 pagesManagement of Pediatric Condyle FracturesAngga PutraNo ratings yet
- Nasal Analysis and Anatomy: Anthropometric Proportional Assessment in Asians-Aesthetic Balance From Forehead To Chin, Part IDocument7 pagesNasal Analysis and Anatomy: Anthropometric Proportional Assessment in Asians-Aesthetic Balance From Forehead To Chin, Part IAngga PutraNo ratings yet
- Mandibula 2Document13 pagesMandibula 2Angga PutraNo ratings yet
- ANZ Burn GuidelinesDocument25 pagesANZ Burn GuidelinesAngga Putra Kusuma KusumaNo ratings yet
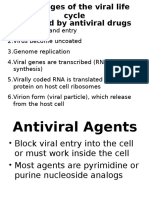
- Antiviral Acyclovir Pc2 DmsDocument5 pagesAntiviral Acyclovir Pc2 DmsAngga PutraNo ratings yet
- Rhinoplasty: Surface Aesthetics and Surgical TechniquesDocument13 pagesRhinoplasty: Surface Aesthetics and Surgical TechniquesAngga PutraNo ratings yet
- IcvDocument1 pageIcvAngga PutraNo ratings yet
- Hand Injury Full TextDocument4 pagesHand Injury Full TextAngga PutraNo ratings yet
- Jsssssssssssssssssssssssssssssssssssssss Kaa B KDocument1 pageJsssssssssssssssssssssssssssssssssssssss Kaa B KAngga PutraNo ratings yet
- IcvDocument1 pageIcvAngga PutraNo ratings yet
- Prosedur Penerimaan PPDSDocument4 pagesProsedur Penerimaan PPDSAngga PutraNo ratings yet
- Lshdgfjaaaaaaaaaaaaaaa Aaaaaaaaaaaaaaaaaa DLKCJVLXCV, XCVN, X VCJK AsvsvsdvDocument1 pageLshdgfjaaaaaaaaaaaaaaa Aaaaaaaaaaaaaaaaaa DLKCJVLXCV, XCVN, X VCJK AsvsvsdvAngga PutraNo ratings yet
- Lshdgfjaaaaaaaaaaaaaaa Aaaaaaaaaaaaaaaaaa DLKCJVLXCV, XCVN, X VCJK AsvsvsdvDocument1 pageLshdgfjaaaaaaaaaaaaaaa Aaaaaaaaaaaaaaaaaa DLKCJVLXCV, XCVN, X VCJK AsvsvsdvAngga PutraNo ratings yet
- E-Poster-Diagnostic in Hand Injury Before Operation, Does It Matter - For MergeDocument1 pageE-Poster-Diagnostic in Hand Injury Before Operation, Does It Matter - For MergeAngga PutraNo ratings yet
- Effect of NAC After Thermal InjuryDocument7 pagesEffect of NAC After Thermal InjuryAngga PutraNo ratings yet
- Lower Extremity: Departement of Anatomy Medical Faculty of North Sumatera UtaraDocument23 pagesLower Extremity: Departement of Anatomy Medical Faculty of North Sumatera UtaraAngga Putra100% (1)
- Departement of Anatomy Medical Faculty of North Sumatra UniversityDocument65 pagesDepartement of Anatomy Medical Faculty of North Sumatra UniversityAngga PutraNo ratings yet
- K-30, K-31 Kuliah FK Kista Dan InfeksiDocument43 pagesK-30, K-31 Kuliah FK Kista Dan InfeksiAngga PutraNo ratings yet
- K-13 Lapkas OsteomyelitisDocument33 pagesK-13 Lapkas OsteomyelitisAngga PutraNo ratings yet
- K-21 Miopati 2011Document70 pagesK-21 Miopati 2011Angga PutraNo ratings yet
- Session #14 SAS - AnaPhy (Lab)Document8 pagesSession #14 SAS - AnaPhy (Lab)G INo ratings yet
- NOTESDocument101 pagesNOTESPaul AshburnerNo ratings yet
- CH 41: Hematological Assessment (Per Amendolair)Document28 pagesCH 41: Hematological Assessment (Per Amendolair)USC Upstate Nursing CoachesNo ratings yet
- Unit 4 Circulatory SystemDocument157 pagesUnit 4 Circulatory SystemChandan ShahNo ratings yet
- PT InrDocument3 pagesPT InrJeniah Lerios OcsioNo ratings yet
- Blood Group Testing: Hong-Yang Li and Kai GuoDocument11 pagesBlood Group Testing: Hong-Yang Li and Kai Guodkp rbmNo ratings yet
- Thromboelastogram (TEG) - LITFL - CCC InvestigationsDocument10 pagesThromboelastogram (TEG) - LITFL - CCC InvestigationsMarcelliaNo ratings yet
- Chart Transfused Blood ProductsDocument2 pagesChart Transfused Blood ProductsAORN2008No ratings yet
- Anaphy Lab Quizlet Flashcards Converted For AnkiDocument6 pagesAnaphy Lab Quizlet Flashcards Converted For AnkiAldrin LimcuandoNo ratings yet
- Laboratory Test Normal Range in Us Units Normal Range in Si Units To Convert Ustosi UnitsDocument5 pagesLaboratory Test Normal Range in Us Units Normal Range in Si Units To Convert Ustosi Unitsloloko55113No ratings yet
- LupusDocument7 pagesLupusorapoosaNo ratings yet
- Special Collections and Point of Care TestingDocument42 pagesSpecial Collections and Point of Care Testingmicah cajandabNo ratings yet
- AO Manual of Fracture Management - Internal Fixators, Thieme 2006-TLS (Michael Wagner)Document889 pagesAO Manual of Fracture Management - Internal Fixators, Thieme 2006-TLS (Michael Wagner)Олексій ЮрченкоNo ratings yet
- Connective TissuesDocument6 pagesConnective TissuesPenelopeNo ratings yet
- Lab ResultDocument1 pageLab Resultrakibul islamNo ratings yet
- Reviewer in Phleb 102 (Week 2)Document6 pagesReviewer in Phleb 102 (Week 2)Hannah Viktoria HernandezNo ratings yet
- Peripheral SmearDocument12 pagesPeripheral Smearapi-3823785100% (1)
- Laboratory Evaluation of FibrinolysisDocument14 pagesLaboratory Evaluation of FibrinolysisSusielyn Anne Tumamao Angobung100% (2)
- 127-Article Text-817-6-10-20180329Document4 pages127-Article Text-817-6-10-20180329Riri Andriani MinHoNo ratings yet
- Medical Technologist-On-Duty: Myrna N. Caranto, RMT Brenda I. Rosuman, MD, FPSPDocument9 pagesMedical Technologist-On-Duty: Myrna N. Caranto, RMT Brenda I. Rosuman, MD, FPSPJeng HidalgoNo ratings yet
- Jadual Graf Bacaan Tekanan DarahDocument2 pagesJadual Graf Bacaan Tekanan Darahsharimax06No ratings yet
- Circulatory TestDocument7 pagesCirculatory TestgarnetNo ratings yet