You might also like
- Thiamine Deficiency Disease, Dysautonomia, and High Calorie MalnutritionFrom EverandThiamine Deficiency Disease, Dysautonomia, and High Calorie MalnutritionRating: 4.5 out of 5 stars4.5/5 (5)
- Phenylketonuria (PKU) : PH Arn, Nemours Children's Clinic, Jacksonville, FL, USADocument3 pagesPhenylketonuria (PKU) : PH Arn, Nemours Children's Clinic, Jacksonville, FL, USAHappy612No ratings yet
- Biochemical IndividualityDocument3 pagesBiochemical IndividualityPhysis.HolisticNo ratings yet
- Munyame 2018Document6 pagesMunyame 2018kemoNo ratings yet
- Phenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)Document1 pagePhenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)reriti2008No ratings yet
- Continuing Education Activity: ObjectivesDocument4 pagesContinuing Education Activity: ObjectiveslalaaNo ratings yet
- PKU: Genetic Disorder Caused by Phenylalanine Metabolism DeficiencyDocument6 pagesPKU: Genetic Disorder Caused by Phenylalanine Metabolism DeficiencyAlbertEscanoNo ratings yet
- 2515-Article Text-13813-1-10-20201215Document4 pages2515-Article Text-13813-1-10-20201215220868No ratings yet
- PhenylketonuriaDocument17 pagesPhenylketonuriamovies villa hit hai broNo ratings yet
- Biochemistry - METABOLISM OF PROTEINDocument44 pagesBiochemistry - METABOLISM OF PROTEINrebeccaNo ratings yet
- Phenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeDocument24 pagesPhenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeAsfoor gake1No ratings yet
- Articulo Final Verdadero!!!!Document6 pagesArticulo Final Verdadero!!!!lapzsssNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaAnny AlvrzNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaReham QueNo ratings yet
- Case 9: Phenylketonuria: Group 1C: Obligado, Ervin Panibon, Lindsy Que, Reham Remitar, Jaira Dizza Salang, Marie NicholeDocument12 pagesCase 9: Phenylketonuria: Group 1C: Obligado, Ervin Panibon, Lindsy Que, Reham Remitar, Jaira Dizza Salang, Marie NicholeReham QueNo ratings yet
- Group 4 - Pku (BSN 1-A)Document11 pagesGroup 4 - Pku (BSN 1-A)oluanah13No ratings yet
- Inborn Errors of MetabolismDocument40 pagesInborn Errors of MetabolismajjaNo ratings yet
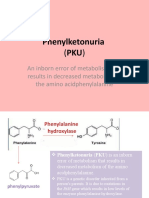
- Phenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino AcidphenylalanineDocument8 pagesPhenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino Acidphenylalanineელენე ბუჩუკურიNo ratings yet
- PKU Definition and InheritanceDocument1 pagePKU Definition and InheritancemucwcburdwanNo ratings yet
- PhenylketonuriaDocument8 pagesPhenylketonuriaAmberlee PetiNo ratings yet
- Bio 485 Final Paper Final DraftDocument8 pagesBio 485 Final Paper Final Draftapi-285174164No ratings yet
- Patogenesis, Skrining, Diagnosis, Dan Penatalaksanaan Phenylketonuria Screening, Diagnosis, and Management of PhenylketonuriaDocument10 pagesPatogenesis, Skrining, Diagnosis, Dan Penatalaksanaan Phenylketonuria Screening, Diagnosis, and Management of PhenylketonuriaAtinul KulsumNo ratings yet
- Inherited Metabolic DisorderDocument12 pagesInherited Metabolic DisorderTrisha Dianne RaquenioNo ratings yet
- Phenylketonuria: An Inborn Error of Phenylalanine MetabolismDocument11 pagesPhenylketonuria: An Inborn Error of Phenylalanine MetabolismAndreea StefanNo ratings yet
- PKU Case Study: Phenylketonuria Due to PAH Gene MutationDocument2 pagesPKU Case Study: Phenylketonuria Due to PAH Gene MutationLeonard Rey Suratos ManabatNo ratings yet
- Inborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaDocument19 pagesInborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaSubhi MishraNo ratings yet
- American Academy of Pediatrics Metabolic Disorders 2014 Practice TestDocument43 pagesAmerican Academy of Pediatrics Metabolic Disorders 2014 Practice TestPrabu KumarNo ratings yet
- Neurological of Biopterin Metabolism: AspectsDocument8 pagesNeurological of Biopterin Metabolism: AspectsabcNo ratings yet
- PhenylketonuriaDocument14 pagesPhenylketonuriaMonica MoralesNo ratings yet
- Intoxicación Por AcetaminofenDocument4 pagesIntoxicación Por AcetaminofenGibsyVillacisMarriottNo ratings yet
- PSYE504a: Figure 1. Proofreading ProcessDocument7 pagesPSYE504a: Figure 1. Proofreading ProcessBianca Isabelle LariosaNo ratings yet
- DR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHDocument2 pagesDR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHPonnusamy KumarNo ratings yet
- 12 GMppt-chapter12-2020 (Ok)Document19 pages12 GMppt-chapter12-2020 (Ok)Kw ChanNo ratings yet
- Clinical FirstDocument342 pagesClinical FirstYasmeen AtiehNo ratings yet
- PKU-giovannini 2007 JimdDocument9 pagesPKU-giovannini 2007 JimdajjaNo ratings yet
- Treating Phenylketonuria with Medical Nutrition TherapyDocument13 pagesTreating Phenylketonuria with Medical Nutrition Therapymohammed alrubaiaanNo ratings yet
- MCH Group 8Document12 pagesMCH Group 8nafisatmuhammed452No ratings yet
- Case3 PhenylketunuriaDocument2 pagesCase3 PhenylketunuriaKath BoniolNo ratings yet
- Impaired Neurotransmission in Early-Treated Phenylketonuria PatientsDocument9 pagesImpaired Neurotransmission in Early-Treated Phenylketonuria PatientsAndreea StefanNo ratings yet
- Endocrine DisordersDocument33 pagesEndocrine DisordersBuvana VigneshNo ratings yet
- AAV-Mediated CRISPR/Cas9 Gene Editing in Murine PhenylketonuriaDocument12 pagesAAV-Mediated CRISPR/Cas9 Gene Editing in Murine PhenylketonuriaSpaceCadetNo ratings yet
- PKU Dietary Handbook in PKUDocument21 pagesPKU Dietary Handbook in PKUItzel Carrillo NietoNo ratings yet
- PKU genetic metabolic disorder causes brain damage without treatmentDocument2 pagesPKU genetic metabolic disorder causes brain damage without treatmentFerdianaNo ratings yet
- Lecture 1 Introduction To Genetic Metabolic DisordersDocument21 pagesLecture 1 Introduction To Genetic Metabolic Disordersamjadm2002No ratings yet
- PHENYLKETONURIADocument3 pagesPHENYLKETONURIAMiwa IshiiNo ratings yet
- Glycomacropeptide For Nutritional Management of Phenylketonuria: A Randomized, Controlled, Crossover TrialDocument12 pagesGlycomacropeptide For Nutritional Management of Phenylketonuria: A Randomized, Controlled, Crossover Trialjz1397No ratings yet
- PHENYLKETONURIADocument22 pagesPHENYLKETONURIAIvy Ann AguirreNo ratings yet
- Phenytoin-Diazepam Interaction: Objective Case SummaryDocument5 pagesPhenytoin-Diazepam Interaction: Objective Case SummaryNavisa HaifaNo ratings yet
- DR Kumar Ponnusamy Biochemistry-Genetics USMLE Preparatory Course BIOGEN Reusable On-Line Resources For Large Group Teaching-Learning in Relatively Short TimeDocument1 pageDR Kumar Ponnusamy Biochemistry-Genetics USMLE Preparatory Course BIOGEN Reusable On-Line Resources For Large Group Teaching-Learning in Relatively Short TimeDr Kumar Ponnusamy100% (1)
- Phenylketonur IA: Done byDocument27 pagesPhenylketonur IA: Done byAsfoor gake1100% (1)
- Se 10Document7 pagesSe 10nafamaulidinaNo ratings yet
- Biochemical Basis of Phenylketonuria and Maple Syrup SyndromeDocument5 pagesBiochemical Basis of Phenylketonuria and Maple Syrup SyndromeLauraTomicNo ratings yet
- PHENYLKETONURIADocument4 pagesPHENYLKETONURIAmarsiel03No ratings yet
- Pku Consens SUA 2000Document17 pagesPku Consens SUA 2000beloshita_88No ratings yet
- NCMA219Document11 pagesNCMA219Angelina Mei BenitezNo ratings yet
- PhenylketonuriaDocument1 pagePhenylketonuriaHolly SevillanoNo ratings yet
- The Complete European Guidelines On Phenylketonuria Diagnosis and TreatmentDocument56 pagesThe Complete European Guidelines On Phenylketonuria Diagnosis and TreatmentI'Jaz Farritz MuhammadNo ratings yet
- Nufd 255 Midterm Paper - No ReferencesDocument7 pagesNufd 255 Midterm Paper - No Referencesapi-305349012No ratings yet
- PhenyketonuriaDocument12 pagesPhenyketonuriamaryannejkiemNo ratings yet
- Impaired Neurotransmission in Early-Treated Phenylketonuria PatientsDocument9 pagesImpaired Neurotransmission in Early-Treated Phenylketonuria PatientsAndreea StefanNo ratings yet
- Identifying Chromosomes 12 and 14Document3 pagesIdentifying Chromosomes 12 and 14AstatinNo ratings yet
- Metabolic Disorders GuideDocument80 pagesMetabolic Disorders GuideXeniyaFedoryakNo ratings yet
- Phenylketonuria PathogenesisDocument2 pagesPhenylketonuria PathogenesisIrene CerisseNo ratings yet
- Genetics of Metabolic Disorders IDocument17 pagesGenetics of Metabolic Disorders IGagan DhaliwalNo ratings yet
- Biology Transition Work 2023Document5 pagesBiology Transition Work 2023Sriihari BalasubramaniyamNo ratings yet
- Inborn Errors of MetabolismDocument12 pagesInborn Errors of Metabolismmichelle octavianiNo ratings yet
- Patogenesis, Skrining, Diagnosis, Dan Penatalaksanaan Phenylketonuria Screening, Diagnosis, and Management of PhenylketonuriaDocument10 pagesPatogenesis, Skrining, Diagnosis, Dan Penatalaksanaan Phenylketonuria Screening, Diagnosis, and Management of PhenylketonuriaAtinul KulsumNo ratings yet
- Mendelian Disorders Class 12Document22 pagesMendelian Disorders Class 12Harith KumarNo ratings yet
- 77: Hyperphenylalaninemia: Phenylalanine Hydroxylase DeficiencyDocument114 pages77: Hyperphenylalaninemia: Phenylalanine Hydroxylase DeficiencyFede0No ratings yet
- Phenylalanine and Tyrosine Metabolism (18 Oct)Document14 pagesPhenylalanine and Tyrosine Metabolism (18 Oct)api-19824406100% (6)
- SYMPOSIUM: MANAGING PHENYLKETONURIADocument5 pagesSYMPOSIUM: MANAGING PHENYLKETONURIAIntan RizanaNo ratings yet
- ProteinDocument89 pagesProteinAki OtaniNo ratings yet
- Biological Function of Protein in CellDocument4 pagesBiological Function of Protein in CellM HAZIM IRFAN MD NOORNo ratings yet
- The Complete European Guidelines On Phenylketonuria Diagnosis and TreatmentDocument56 pagesThe Complete European Guidelines On Phenylketonuria Diagnosis and TreatmentI'Jaz Farritz MuhammadNo ratings yet
- (Advances in Experimental Medicine and Biology 338) Wolfgang Pfleiderer (Auth.), Dr. June E. Ayling, M. Gopal Nair, Dr. Charles M. Baugh (Eds.)-Chemistry and Biology of Pteridines and Folates-SpringerDocument805 pages(Advances in Experimental Medicine and Biology 338) Wolfgang Pfleiderer (Auth.), Dr. June E. Ayling, M. Gopal Nair, Dr. Charles M. Baugh (Eds.)-Chemistry and Biology of Pteridines and Folates-SpringerdiannanicaNo ratings yet
- Bchemistry - Exercises 14-15Document30 pagesBchemistry - Exercises 14-15NIYONSHUTI VIATEUR100% (1)
- 11 01 Aminoacid 2012 ENDocument69 pages11 01 Aminoacid 2012 ENanthony.johNo ratings yet
- Original Contribution: Oxidative Stress in A Phenylketonuria Animal ModelDocument6 pagesOriginal Contribution: Oxidative Stress in A Phenylketonuria Animal ModelAndreea StefanNo ratings yet
- Answers To Case 38: Phenylketonuria (Pku) : Summary: A 1-Year-Old Girl Born Outside The United States With DevelopmentalDocument9 pagesAnswers To Case 38: Phenylketonuria (Pku) : Summary: A 1-Year-Old Girl Born Outside The United States With DevelopmentalKarilNo ratings yet
- 2016, Gene, A Novel Common Large Genomic Deletion and Two New MissenseDocument7 pages2016, Gene, A Novel Common Large Genomic Deletion and Two New MissenseRomana VulturarNo ratings yet
- PAH mutation map revised January 2007Document1 pagePAH mutation map revised January 2007Alvi-pba Santiago0% (1)
- Treating Phenylketonuria with Medical Nutrition TherapyDocument13 pagesTreating Phenylketonuria with Medical Nutrition Therapymohammed alrubaiaanNo ratings yet
- Glycomacropeptide For Nutritional Management of Phenylketonuria: A Randomized, Controlled, Crossover TrialDocument12 pagesGlycomacropeptide For Nutritional Management of Phenylketonuria: A Randomized, Controlled, Crossover Trialjz1397No ratings yet
- Phenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeDocument24 pagesPhenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeAsfoor gake1No ratings yet
- Alexander Kang - Poster Presentation 2023Document4 pagesAlexander Kang - Poster Presentation 2023alexanderkang0930No ratings yet
- PKU-Role of Pre-Natal DiagnosisDocument6 pagesPKU-Role of Pre-Natal DiagnosisSaeed HasanNo ratings yet
- Ordovas - Nutritional Genomics AnnRevHumGenetDocument50 pagesOrdovas - Nutritional Genomics AnnRevHumGenetSaumya SurekhaNo ratings yet