You might also like
- PhenylketonuriaDocument17 pagesPhenylketonuriamovies villa hit hai broNo ratings yet
- PKU: Genetic Disorder Caused by Phenylalanine Metabolism DeficiencyDocument6 pagesPKU: Genetic Disorder Caused by Phenylalanine Metabolism DeficiencyAlbertEscanoNo ratings yet
- Continuing Education Activity: ObjectivesDocument4 pagesContinuing Education Activity: ObjectiveslalaaNo ratings yet
- SYMPOSIUM: MANAGING PHENYLKETONURIADocument5 pagesSYMPOSIUM: MANAGING PHENYLKETONURIAIntan RizanaNo ratings yet
- Phenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)Document1 pagePhenylketonuria (PKU) : (Metabolic Condition: Amino Acid Disorder)reriti2008No ratings yet
- MCH Group 8Document12 pagesMCH Group 8nafisatmuhammed452No ratings yet
- PKU genetic metabolic disorder causes brain damage without treatmentDocument2 pagesPKU genetic metabolic disorder causes brain damage without treatmentFerdianaNo ratings yet
- Phenyl Keto NuriaDocument3 pagesPhenyl Keto NuriawawawawaNo ratings yet
- Phenylketonuria (PKU) : PH Arn, Nemours Children's Clinic, Jacksonville, FL, USADocument3 pagesPhenylketonuria (PKU) : PH Arn, Nemours Children's Clinic, Jacksonville, FL, USAHappy612No ratings yet
- American Academy of Pediatrics Metabolic Disorders 2014 Practice TestDocument43 pagesAmerican Academy of Pediatrics Metabolic Disorders 2014 Practice TestPrabu KumarNo ratings yet
- Inborn Errors of MetabolismDocument40 pagesInborn Errors of MetabolismajjaNo ratings yet
- DR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHDocument2 pagesDR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHPonnusamy KumarNo ratings yet
- PHENYLKETONURIADocument22 pagesPHENYLKETONURIAIvy Ann AguirreNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaAnny AlvrzNo ratings yet
- PKU Genetic DisorderDocument3 pagesPKU Genetic DisorderUnnat ShresthaNo ratings yet
- PhenylketonuriaDocument7 pagesPhenylketonuriaReham QueNo ratings yet
- Inherited Metabolic DisorderDocument12 pagesInherited Metabolic DisorderTrisha Dianne RaquenioNo ratings yet
- Group 4 - Pku (BSN 1-A)Document11 pagesGroup 4 - Pku (BSN 1-A)oluanah13No ratings yet
- Pku Consens SUA 2000Document17 pagesPku Consens SUA 2000beloshita_88No ratings yet
- Biochemistry - METABOLISM OF PROTEINDocument44 pagesBiochemistry - METABOLISM OF PROTEINrebeccaNo ratings yet
- PHENYLKETONURIADocument3 pagesPHENYLKETONURIAMiwa IshiiNo ratings yet
- What Is PKU?: That Humans Obtain From Their Diet and Cannot Produce On Their Own.)Document2 pagesWhat Is PKU?: That Humans Obtain From Their Diet and Cannot Produce On Their Own.)SelliEfridaSiahaanNo ratings yet
- PhenylketonuriaDocument8 pagesPhenylketonuriaAmberlee PetiNo ratings yet
- Endocrine DisordersDocument33 pagesEndocrine DisordersBuvana VigneshNo ratings yet
- DR Kumar Ponnusamy Biochemistry-Genetics USMLE Preparatory Course BIOGEN Reusable On-Line Resources For Large Group Teaching-Learning in Relatively Short TimeDocument1 pageDR Kumar Ponnusamy Biochemistry-Genetics USMLE Preparatory Course BIOGEN Reusable On-Line Resources For Large Group Teaching-Learning in Relatively Short TimeDr Kumar Ponnusamy100% (1)
- Inborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaDocument19 pagesInborn Errors of Metabolism: Albinism, Cystinuria, Pentosuria And, of Course, AlkaptonuriaSubhi MishraNo ratings yet
- PhenylketonuriaDocument1 pagePhenylketonuriaHolly SevillanoNo ratings yet
- NCMA219Document11 pagesNCMA219Angelina Mei BenitezNo ratings yet
- Pku GRP 1Document19 pagesPku GRP 1Jersey MariNo ratings yet
- PhenylketonuriaDocument10 pagesPhenylketonuriaMalathy Ravendran100% (1)
- Phenylketonuria: Katrice Shorter, Steven Williams, Rodrigo Hallais, April Mcclendon "The Juice"Document24 pagesPhenylketonuria: Katrice Shorter, Steven Williams, Rodrigo Hallais, April Mcclendon "The Juice"Kimber ManiulitNo ratings yet
- PhenylketonuriaDocument14 pagesPhenylketonuriaMonica MoralesNo ratings yet
- PKU Definition and InheritanceDocument1 pagePKU Definition and InheritancemucwcburdwanNo ratings yet
- WIC Case StudyDocument3 pagesWIC Case Studydsaitta108No ratings yet
- Endocrine DisordersDocument33 pagesEndocrine DisordersTinaNo ratings yet
- Nufd 255 Midterm Paper - No ReferencesDocument7 pagesNufd 255 Midterm Paper - No Referencesapi-305349012No ratings yet
- PhenylketonuriaDocument4 pagesPhenylketonuriaapi-444025342No ratings yet
- PKUDocument8 pagesPKUNader Smadi100% (1)
- Fenilcetonuria Genetica 2014Document8 pagesFenilcetonuria Genetica 2014Jhon NavarroNo ratings yet
- What Is Phenylketonuria?Document4 pagesWhat Is Phenylketonuria?Erica Joy Algire VillalunaNo ratings yet
- Biochemical IndividualityDocument3 pagesBiochemical IndividualityPhysis.HolisticNo ratings yet
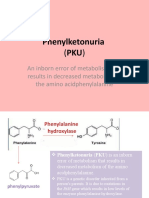
- Phenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino AcidphenylalanineDocument8 pagesPhenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino Acidphenylalanineელენე ბუჩუკურიNo ratings yet
- Fenilketonuria: Devi WuysangDocument23 pagesFenilketonuria: Devi WuysangChristantina Pradescha AssaNo ratings yet
- Treating Phenylketonuria with Medical Nutrition TherapyDocument13 pagesTreating Phenylketonuria with Medical Nutrition Therapymohammed alrubaiaanNo ratings yet
- Lecture 2 Disorders of Amino Acid Metabolism Phenylketonuria (PKU)Document22 pagesLecture 2 Disorders of Amino Acid Metabolism Phenylketonuria (PKU)amjadm2002No ratings yet
- 84mother ArticleDocument7 pages84mother ArticleGAYATHIRINo ratings yet
- Phenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeDocument24 pagesPhenylketonuria: Abbas A. A. Shawka Medical Student 2 GradeAsfoor gake1No ratings yet
- Casestudy Makato 2nd Pre EclampsiaDocument7 pagesCasestudy Makato 2nd Pre EclampsiaRainier IbarretaNo ratings yet
- Compilation of Research On PhenylketonuriaDocument12 pagesCompilation of Research On PhenylketonuriajudssalangsangNo ratings yet
- Searching for genetic clues to causes of pre-eclampsiaDocument16 pagesSearching for genetic clues to causes of pre-eclampsiaBian DaraNo ratings yet
- PDF TJP 1232Document3 pagesPDF TJP 1232Devi PediatriNo ratings yet
- Jurnal Reading PPT FixxeddDocument36 pagesJurnal Reading PPT Fixxeddiman prawiraNo ratings yet
- Congenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementFrom EverandCongenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementDiva D. De León-CrutchlowNo ratings yet
- PHENYLKETONURIADocument4 pagesPHENYLKETONURIAmarsiel03No ratings yet
- Pku - Phenyl KetonuriaDocument21 pagesPku - Phenyl KetonuriakvprasadchNo ratings yet
- Articulo Final Verdadero!!!!Document6 pagesArticulo Final Verdadero!!!!lapzsssNo ratings yet
- Neonatal HypocalcemiaDocument5 pagesNeonatal HypocalcemiaLekshmi ManuNo ratings yet
- Medicines in Pregnancy - PHAR3201Document48 pagesMedicines in Pregnancy - PHAR3201AINo ratings yet
- General Luna ST., 5000 Iloilo City, Philippines College of Nursing, Nutrition & Dietetics Nursing DepartmentDocument4 pagesGeneral Luna ST., 5000 Iloilo City, Philippines College of Nursing, Nutrition & Dietetics Nursing DepartmentAxel June JanagapNo ratings yet
- Shared Decision Making PDF 66142087186885Document32 pagesShared Decision Making PDF 66142087186885kemoNo ratings yet
- Revell 2014Document6 pagesRevell 2014kemoNo ratings yet
- Brier Ley 2020Document8 pagesBrier Ley 2020kemoNo ratings yet
- Article 10.1111/tog.12599Document8 pagesArticle 10.1111/tog.12599KeeranmayeeishraNo ratings yet
- Case Study of Bronchial Asthma in Acute ExacerbationDocument16 pagesCase Study of Bronchial Asthma in Acute Exacerbationdextroid1290% (29)
- Ppt-Project Management Baia MareDocument35 pagesPpt-Project Management Baia MareMarchiș AlexandraNo ratings yet
- Managing Corporate Real Estate: Leading and Emerging PracticesDocument24 pagesManaging Corporate Real Estate: Leading and Emerging PracticesramyeidNo ratings yet
- PSYCHOLOGY Lesson 2Document15 pagesPSYCHOLOGY Lesson 2KOSTKANo ratings yet
- Drug Addiction and Effects On EducationDocument3 pagesDrug Addiction and Effects On EducationRJ Castro ParedesNo ratings yet
- Clinical and Dermoscopic Features of Seborrheic KeratosisDocument1 pageClinical and Dermoscopic Features of Seborrheic KeratosisRicky SetiawanNo ratings yet
- Effect of Ethanol Leaf Extract of Chromolaena Odorata On Lipid Profile of Streptozotocin Induced Diabetic Wistar Albino RatsDocument9 pagesEffect of Ethanol Leaf Extract of Chromolaena Odorata On Lipid Profile of Streptozotocin Induced Diabetic Wistar Albino RatsPUBLISHER JOURNALNo ratings yet
- Pediatric Cardiology II Lecture SummaryDocument5 pagesPediatric Cardiology II Lecture SummaryMedisina101No ratings yet
- Incident Investigation and Reporting ProcedureDocument6 pagesIncident Investigation and Reporting ProcedureSérgio CoutoNo ratings yet
- Carpal Tunnel Syndrome A Review of Literature PDFDocument9 pagesCarpal Tunnel Syndrome A Review of Literature PDFFabrizio PaglierucciNo ratings yet
- Drug Law Seminar PaperDocument70 pagesDrug Law Seminar PaperBapulNo ratings yet
- UNIT5 Technology of Bread MakingDocument12 pagesUNIT5 Technology of Bread MakingS ENo ratings yet
- Principles of Monitoring & Evaluation - NotesDocument113 pagesPrinciples of Monitoring & Evaluation - NotesKeith100% (2)
- Digital Citizenship vs. Global CitizenshipDocument20 pagesDigital Citizenship vs. Global CitizenshipMacasinag Jamie Anne M.No ratings yet
- The Kübler-Ross Change Curve: Emotional Response To ChangeDocument9 pagesThe Kübler-Ross Change Curve: Emotional Response To ChangeChanel PostelNo ratings yet
- A Case of Possible Hypersensitivity Reactions To Human InsulinDocument6 pagesA Case of Possible Hypersensitivity Reactions To Human Insulingandik danu pramigaNo ratings yet
- Being in The World Selected Pa Ludwig BinswangerDocument388 pagesBeing in The World Selected Pa Ludwig BinswangerRamazan ÇarkıNo ratings yet
- Participants List DDO's and Their Staff 25Document3 pagesParticipants List DDO's and Their Staff 25Manoj Digi LoansNo ratings yet
- Implementing Trauma-Informed Care in Primary Hamberger-2019-Medical Settings-Evidence-Based Rationale and Approaches PDFDocument22 pagesImplementing Trauma-Informed Care in Primary Hamberger-2019-Medical Settings-Evidence-Based Rationale and Approaches PDFMonica DyerNo ratings yet
- Carlton Turner StatementDocument1 pageCarlton Turner StatementNews-PressNo ratings yet
- Risk ManagementDocument15 pagesRisk ManagementABEGAIL MADLAONo ratings yet
- RCB Charcoal Catalog (PT Rajha CB) - CompressedDocument10 pagesRCB Charcoal Catalog (PT Rajha CB) - CompressedCepi OktavianNo ratings yet
- Reflective Practice JournalDocument5 pagesReflective Practice JournalReuben RussellNo ratings yet
- ReportingDocument4 pagesReportingMark CalimlimNo ratings yet
- Audiometer Impedqnce Audiometer AT235 - USER - MANUALDocument103 pagesAudiometer Impedqnce Audiometer AT235 - USER - MANUALKafina Multi SejahteraNo ratings yet
- Openhrt 2021 001732Document9 pagesOpenhrt 2021 001732benypermadiNo ratings yet
- HirsutismDocument10 pagesHirsutismMarielle VentulaNo ratings yet
- Fpsyg 12 601849Document16 pagesFpsyg 12 601849NOR BIBI MASLINA BINTI JUSOH MoeNo ratings yet
- Continuous Monitoring of Erns: Set of Ern Core IndicatorsDocument23 pagesContinuous Monitoring of Erns: Set of Ern Core IndicatorsElenaNo ratings yet
- Orthop J Sports Med 2021 9 7 23259671211013394Document6 pagesOrthop J Sports Med 2021 9 7 23259671211013394Fernando SousaNo ratings yet