You might also like
- The Patient History An Evidence-Based Approach To Differential DiagnosisDocument4 pagesThe Patient History An Evidence-Based Approach To Differential DiagnosisISAYK13% (8)
- Vaccine Science vs. Science FictionDocument16 pagesVaccine Science vs. Science FictionBright09100% (1)
- A Guide To Getting Started in TelemedicineDocument405 pagesA Guide To Getting Started in TelemedicineAnthony WilsonNo ratings yet
- NVBSP Form15Document6 pagesNVBSP Form15Rhodz Caballes RefuerzoNo ratings yet
- Risk For FallDocument3 pagesRisk For FallLesValenzuela100% (1)
- Paediatrica IndonesianaDocument8 pagesPaediatrica Indonesianachartreuse avonleaNo ratings yet
- Paediatrica IndonesianaDocument8 pagesPaediatrica Indonesianafkia2013No ratings yet
- 2.jurnal Kepkel4Document7 pages2.jurnal Kepkel4Himatul AliyahNo ratings yet
- Jurnal Indonesia 1Document11 pagesJurnal Indonesia 1Juli ArnithaNo ratings yet
- 1 s2.0 S2352013216300205 MainDocument9 pages1 s2.0 S2352013216300205 MainDendy FebriantNo ratings yet
- Analysis of Factors Affecting The Prevalence of Stunting On Children Under Five Years 8429Document11 pagesAnalysis of Factors Affecting The Prevalence of Stunting On Children Under Five Years 8429Demsa SimbolonNo ratings yet
- Pengaruh Stimulasi Terhadap Perkembangan Motorik Kasar Pada Anak Usia 1-3 Tahun Di Desa Renda Kecamatan Towea Kabupaten Muna Sulawesi TenggaraDocument7 pagesPengaruh Stimulasi Terhadap Perkembangan Motorik Kasar Pada Anak Usia 1-3 Tahun Di Desa Renda Kecamatan Towea Kabupaten Muna Sulawesi TenggaraHidayahNo ratings yet
- Paediatrica IndonesianaDocument8 pagesPaediatrica IndonesianaAnna ClarkNo ratings yet
- Jurnal KasmaDocument13 pagesJurnal KasmaAhmad ZahirNo ratings yet
- Prenatal Factors Associated With The Risk of Stunting: A Multilevel Analysis Evidence From Nganjuk, East JavaDocument7 pagesPrenatal Factors Associated With The Risk of Stunting: A Multilevel Analysis Evidence From Nganjuk, East JavaRido SaputraNo ratings yet
- 451 1378 1 PBDocument11 pages451 1378 1 PBprawira heroNo ratings yet
- Jurnal Stunting PDFDocument10 pagesJurnal Stunting PDFNanang SupriyantoNo ratings yet
- The Dominant Factors of Stunting Incidence in Toddlers (0 - 59 Months) in East Lombok Regency A Riskesdas Data Analysis 2018Document11 pagesThe Dominant Factors of Stunting Incidence in Toddlers (0 - 59 Months) in East Lombok Regency A Riskesdas Data Analysis 2018International Journal of Innovative Science and Research Technology100% (1)
- JPaediatrNursSci 3 3 73 761Document4 pagesJPaediatrNursSci 3 3 73 761vaideeswari kumarNo ratings yet
- Anastasia 2023Document17 pagesAnastasia 2023lalallili2No ratings yet
- Ana Riandari (152221039) Tugas Penelitian Kebidanan 2 (Dosen Isfaizah, S.si.T.,MPH)Document12 pagesAna Riandari (152221039) Tugas Penelitian Kebidanan 2 (Dosen Isfaizah, S.si.T.,MPH)Ana RiandariNo ratings yet
- Faktor - Faktor Yang Berhubungan Dengan Pertumbuhan Bayi 6-12 Bulan Di Puskesmas Simpang BaruDocument7 pagesFaktor - Faktor Yang Berhubungan Dengan Pertumbuhan Bayi 6-12 Bulan Di Puskesmas Simpang BaruWidhea novita putriNo ratings yet
- Rifda Azkiatus Salamah - 4411418014Document26 pagesRifda Azkiatus Salamah - 4411418014Rifda AzkiaNo ratings yet
- Investigating Minimum Acceptable Diet and Infant and Child Feeding Index As Indicators of Stunting in Children Aged 6-23 MonthsDocument10 pagesInvestigating Minimum Acceptable Diet and Infant and Child Feeding Index As Indicators of Stunting in Children Aged 6-23 MonthsAlif riadiNo ratings yet
- Determinants of Stunting in Children Aged 12-59 MonthsDocument10 pagesDeterminants of Stunting in Children Aged 12-59 MonthsMichimichi 78No ratings yet
- Wellness and Healthy Wellness and Healthy Magazine MagazineDocument10 pagesWellness and Healthy Wellness and Healthy Magazine MagazineGalih EkaNo ratings yet
- Naskah Publikasi P1337424415045Document9 pagesNaskah Publikasi P1337424415045rechybsNo ratings yet
- Association of Energy Intake and Physical Activity With OverweighDocument6 pagesAssociation of Energy Intake and Physical Activity With OverweighArdanNo ratings yet
- 2246-Article Text-8369-9706-10-20230606Document11 pages2246-Article Text-8369-9706-10-20230606Gek Sinta ManuabaNo ratings yet
- 247 767 1 PB PDFDocument10 pages247 767 1 PB PDFAnnisa Abdul AzisNo ratings yet
- Journal Determinants of Stunting and Child Development in Jombang District With Summary (Background Underlying The Occurrence of Stunting)Document27 pagesJournal Determinants of Stunting and Child Development in Jombang District With Summary (Background Underlying The Occurrence of Stunting)Alifia 123No ratings yet
- Pone 0233949Document13 pagesPone 0233949Shanya rahma AdrianiNo ratings yet
- A Determinant Analysis of Stunting Prevalence On Under 5-Year-Old Children To Establish Stunting Management PolicyDocument6 pagesA Determinant Analysis of Stunting Prevalence On Under 5-Year-Old Children To Establish Stunting Management PolicypuspitaNo ratings yet
- Jurnal Metodologi Penelitian (Afria Novita)Document24 pagesJurnal Metodologi Penelitian (Afria Novita)Afria NovitaNo ratings yet
- Esay Bahasa InggrisDocument6 pagesEsay Bahasa Inggrisni madeNo ratings yet
- Health Literacy and Health Promotion Behaviors of Adolescents in TurkeyDocument5 pagesHealth Literacy and Health Promotion Behaviors of Adolescents in Turkeyege fNo ratings yet
- Stunting Among Children Under Two Years in IndonesiaDocument12 pagesStunting Among Children Under Two Years in Indonesiarezky_tdNo ratings yet
- Correlation Between Non-Exclusive Breastfeeding and Low Birth Weight To Stunting in ChildrenDocument5 pagesCorrelation Between Non-Exclusive Breastfeeding and Low Birth Weight To Stunting in ChildrenAnonymous hETtEBkk7No ratings yet
- Sharma2011 Article GrowthAndNeurosensoryOutcomesODocument6 pagesSharma2011 Article GrowthAndNeurosensoryOutcomesOSayak ChowdhuryNo ratings yet
- Development of Stunting Early Detection Kit For Children Under Two Years: Validity and ReliabilityDocument8 pagesDevelopment of Stunting Early Detection Kit For Children Under Two Years: Validity and ReliabilityviharadewiNo ratings yet
- 35064-Article Text-104064-1-10-20200902Document8 pages35064-Article Text-104064-1-10-20200902kirito azumaNo ratings yet
- Perceived Susceptibility, Barriers, and Cues To Action As Determinant Factors of Reproductive Health BehaviorDocument9 pagesPerceived Susceptibility, Barriers, and Cues To Action As Determinant Factors of Reproductive Health BehaviorIJPHSNo ratings yet
- Sociocultural Transformation in Efforts To Reduce Mortality of Infants in Bone Regency IndonesiaDocument4 pagesSociocultural Transformation in Efforts To Reduce Mortality of Infants in Bone Regency IndonesiaidhaNo ratings yet
- Nusantara Hasana JournalDocument14 pagesNusantara Hasana JournalSiska Andariani RukmanaNo ratings yet
- Jurnal - Faktor Risiko Kejadian Stunting Pada Anak Usia 6-7 TahunDocument8 pagesJurnal - Faktor Risiko Kejadian Stunting Pada Anak Usia 6-7 TahunRezki Sari Anastasya TarmaniNo ratings yet
- Mentoring Program To Eradicate Malnutrition On Changes in The Nutritional Status of Stunting ToddlersDocument8 pagesMentoring Program To Eradicate Malnutrition On Changes in The Nutritional Status of Stunting ToddlersNIKENNo ratings yet
- Penelitian Pak Dodik Maternal Factor Ke Panjang LahirDocument4 pagesPenelitian Pak Dodik Maternal Factor Ke Panjang LahirRiri Amanda PratiwiNo ratings yet
- 1365-Article Text-4113-1-10-20220601Document6 pages1365-Article Text-4113-1-10-20220601hyunNo ratings yet
- Ejhs3203 0569Document10 pagesEjhs3203 0569ERNINo ratings yet
- Muhoozi 2017Document11 pagesMuhoozi 2017Dewi PrasetiaNo ratings yet
- Pertumbuhan Dan Perkembangan Anak Usia 3-6 TahunDocument8 pagesPertumbuhan Dan Perkembangan Anak Usia 3-6 TahunSilvi EkaNo ratings yet
- Hasriani PharmacognJ 15-5-833Document6 pagesHasriani PharmacognJ 15-5-833ardisukardi31No ratings yet
- PYMS Is A Reliable Malnutrition Screening ToolsDocument8 pagesPYMS Is A Reliable Malnutrition Screening ToolsRika LedyNo ratings yet
- Arindah Nur Sartika Prenatal and Postnatal Determinants of Stunting at Age 0-11 MonthsDocument14 pagesArindah Nur Sartika Prenatal and Postnatal Determinants of Stunting at Age 0-11 MonthsHanifa W PNo ratings yet
- Faktor-Faktor Yang Mempengaruhi Terjadinya Stunting Pada Balita Usia 24-59 BulanDocument8 pagesFaktor-Faktor Yang Mempengaruhi Terjadinya Stunting Pada Balita Usia 24-59 Bulansusi hendriyatiNo ratings yet
- Priyanka K P Synopsis-1Document18 pagesPriyanka K P Synopsis-1RAJESHWARI PNo ratings yet
- Survai Dasar Gizi Dan Kesehatan Di Wilayah Kerja World Vision Indonesia Dan Wahana Visi Indonesia Di Kabupaten MeraukeDocument8 pagesSurvai Dasar Gizi Dan Kesehatan Di Wilayah Kerja World Vision Indonesia Dan Wahana Visi Indonesia Di Kabupaten Meraukedwisuci91No ratings yet
- Kurva Pertumbuhan Anak Sehat Usia 3-18 Bulan Dari Keluarga Ekonomi Menengah Ke AtasDocument9 pagesKurva Pertumbuhan Anak Sehat Usia 3-18 Bulan Dari Keluarga Ekonomi Menengah Ke Atasracut_khansatraNo ratings yet
- STUNTINGDocument33 pagesSTUNTINGNini FarahNo ratings yet
- Etiologies and Early Diagnosis of Short Stature and Growth Failure in Children and AdolescentsDocument20 pagesEtiologies and Early Diagnosis of Short Stature and Growth Failure in Children and AdolescentsAnonymous 4N1GrDNo ratings yet
- Paper+21+ (2022 3 4) +The+Relationship+between+Family+Function+and+Emotional+Mental+ProblemsDocument6 pagesPaper+21+ (2022 3 4) +The+Relationship+between+Family+Function+and+Emotional+Mental+ProblemsWinonaNo ratings yet
- Neurodesarrollo PEG Japón 2015Document9 pagesNeurodesarrollo PEG Japón 2015Carlos Manuel Carranza VegaNo ratings yet
- Modelling Number of Stunting Binominal RegressionDocument16 pagesModelling Number of Stunting Binominal RegressionFikran Ahmad Ahmad Al-HadiNo ratings yet
- A Review of Child Stunting Determinants in IndonesiaDocument10 pagesA Review of Child Stunting Determinants in IndonesiaPutri SaripaneNo ratings yet
- Social Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsFrom EverandSocial Determinants of Health and Knowledge About Hiv/Aids Transmission Among AdolescentsNo ratings yet
- Kebabs With A Side of SalmonellaDocument8 pagesKebabs With A Side of SalmonellaAlana TindaleNo ratings yet
- Cancer EpidemiologyDocument18 pagesCancer EpidemiologyMariaLisseth MoralesNo ratings yet
- AZOL 100 & AZOL 200: Azolnew Zealand Data SheetDocument11 pagesAZOL 100 & AZOL 200: Azolnew Zealand Data SheetSwempi Melchiadi AbollaNo ratings yet
- Ortho CaseDocument26 pagesOrtho CaseYusra ShaukatNo ratings yet
- GN RH AnaloguesDocument8 pagesGN RH Analoguesmahesh bhosaleNo ratings yet
- Service Annotated BibliographyDocument6 pagesService Annotated Bibliographyapi-355966257No ratings yet
- Alexandra Charrow: Implicit in What You're Asking Is The: MedicineDocument4 pagesAlexandra Charrow: Implicit in What You're Asking Is The: MedicineAletheia LaiNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainPrincess Alane MorenoNo ratings yet
- Resume' of AnreiDocument3 pagesResume' of AnreianreilegardeNo ratings yet
- "Dr. Pam" Gumbs Recognized As A Professional of The Year For Two Consecutive Years by Strathmore's Who's Who WorldwideDocument2 pages"Dr. Pam" Gumbs Recognized As A Professional of The Year For Two Consecutive Years by Strathmore's Who's Who WorldwidePR.comNo ratings yet
- Form Etik RevisiDocument12 pagesForm Etik RevisiRoma WestNo ratings yet
- Pit Fissure Sealants The Added Link in Preventative DentistryDocument1 pagePit Fissure Sealants The Added Link in Preventative Dentistryapi-348271404No ratings yet
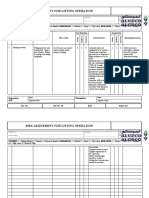
- Risk Assessment For Lifting OperationDocument2 pagesRisk Assessment For Lifting OperationdsadasNo ratings yet
- Ebright Testimony UpdatedDocument28 pagesEbright Testimony UpdatedDeborah WeismanNo ratings yet
- Employee Benefits Program by Etiqa Life Insurance BerhadDocument23 pagesEmployee Benefits Program by Etiqa Life Insurance BerhadNurain SarinaNo ratings yet
- Biểu Đồ Không Có Tiêu Đề.drawioDocument46 pagesBiểu Đồ Không Có Tiêu Đề.drawioha thong thuongNo ratings yet
- Essentials of Nursing Leadership and Management 6th Edition Weiss Test Bank DownloadDocument4 pagesEssentials of Nursing Leadership and Management 6th Edition Weiss Test Bank Downloademmanuelmabelnjt7nn100% (32)
- Geria LecturetteDocument64 pagesGeria LecturetteSVPSNo ratings yet
- Viva Questions For MFD Part 2 ConsolidatedDocument34 pagesViva Questions For MFD Part 2 ConsolidatedEnea Nastri100% (1)
- Autohemotherapy - Treatment of SclerodermaDocument7 pagesAutohemotherapy - Treatment of SclerodermaOlivarNo ratings yet
- Law & Medicine Unit - 1Document4 pagesLaw & Medicine Unit - 1RosylaNo ratings yet
- ANM-Manual HIVAIDS PDFDocument203 pagesANM-Manual HIVAIDS PDFhemihemaNo ratings yet
- UlcerativecolitisDocument27 pagesUlcerativecolitisMohamed Abdulrazaq100% (1)
- Clinical Solid Waste Management Practices and Its Impact On Human Health and EnvironmentDocument13 pagesClinical Solid Waste Management Practices and Its Impact On Human Health and EnvironmentLi NearNo ratings yet
- Meningitis - 2018Document55 pagesMeningitis - 2018Abraham Anaely100% (1)