You might also like
- Goldsmith 2000Document24 pagesGoldsmith 2000valeperoneNo ratings yet
- Langmore 1988 Fiberoptic Endoscopic Examination of Swallowing SafetyDocument4 pagesLangmore 1988 Fiberoptic Endoscopic Examination of Swallowing SafetyDesiré MagalhãesNo ratings yet
- Matsuo 2008Document8 pagesMatsuo 2008Yeimi ArdilaNo ratings yet
- Sek ResiDocument6 pagesSek ResiFadlan SeptiawanNo ratings yet
- Evaluation and Classification of Post-Extubation Dysphagia in CritDocument9 pagesEvaluation and Classification of Post-Extubation Dysphagia in CritNatalia Andrea RozoNo ratings yet
- Effectiveness of Apneic Oxygenatio During IntubationDocument23 pagesEffectiveness of Apneic Oxygenatio During IntubationDavid ParraNo ratings yet
- Tracheostomy and Intubation Related DysphagiaDocument25 pagesTracheostomy and Intubation Related DysphagiaVikashNo ratings yet
- Speech Therapy Rehabilitation After Laryngeal Cancer SurgeryDocument5 pagesSpeech Therapy Rehabilitation After Laryngeal Cancer SurgeryMian Imran IqbalNo ratings yet
- Efficacy of Myofunctional Therapy Associated With Voice Therapy in The Rehabilitation of Neurogenic Oropharyngeal Dysphagia: A Pilot StudyDocument6 pagesEfficacy of Myofunctional Therapy Associated With Voice Therapy in The Rehabilitation of Neurogenic Oropharyngeal Dysphagia: A Pilot StudyÁnyela H. Merchán MendozaNo ratings yet
- The Effect of Voluntary Pharyngeal Swallowing Maneuvers On Esophageal Swallowing PhysiologyDocument7 pagesThe Effect of Voluntary Pharyngeal Swallowing Maneuvers On Esophageal Swallowing PhysiologyAndressa AraújoNo ratings yet
- Continuous Positive Airway Pressure (CPAP) in The Treatment of HypernasalityDocument3 pagesContinuous Positive Airway Pressure (CPAP) in The Treatment of HypernasalitySulochna WeerasekaraNo ratings yet
- Speaking ValveDocument6 pagesSpeaking ValveJonssito Griffin Iglesias PerezNo ratings yet
- Criterios Para Avaliacao Clinica Fonoaudiologica dDocument12 pagesCriterios Para Avaliacao Clinica Fonoaudiologica dAngélica GarcíaNo ratings yet
- Sputum Rheology Changes in Cystic Fibrosis Lung Disease Following Two Different Types of PhysiotherapyDocument7 pagesSputum Rheology Changes in Cystic Fibrosis Lung Disease Following Two Different Types of PhysiotherapyConstanza Martinez ArancibiaNo ratings yet
- Effectiveness of Apneic Oxygenation During IntubationDocument23 pagesEffectiveness of Apneic Oxygenation During IntubationJpmspoonNo ratings yet
- Efectos Anestesia Bilateral Dentarioen Masticacióny DeglusDocument6 pagesEfectos Anestesia Bilateral Dentarioen Masticacióny DeglusMilton David Rios SerratoNo ratings yet
- Influence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientsDocument6 pagesInfluence of The Cuff Pressure On The Swallowing Reflex in Tracheostomized Intensive Care Unit PatientsÁNYELA H. MERCHÁN MENDOZANo ratings yet
- Correlation Between Laryngeal Sensitivity and Penetration/ Aspiration After StrokeDocument6 pagesCorrelation Between Laryngeal Sensitivity and Penetration/ Aspiration After StrokeRodrigo Felipe Toro MellaNo ratings yet
- CoughDocument8 pagesCoughEduardo Cantu GarzaNo ratings yet
- Video-Assisted Instruction Improves The Success Rate For Tracheal Intubation by NovicesDocument5 pagesVideo-Assisted Instruction Improves The Success Rate For Tracheal Intubation by Novicesjuanp.vasquezNo ratings yet
- HHS Public Access: Effects of Chin-Up Posture On The Sequence of Swallowing EventsDocument30 pagesHHS Public Access: Effects of Chin-Up Posture On The Sequence of Swallowing EventsMarcia SantanaNo ratings yet
- ENDOTRACHEAL INTUBATIOn SandeepDocument17 pagesENDOTRACHEAL INTUBATIOn SandeepSimran JosanNo ratings yet
- (MO-CHILE) Willging J., Et Al. Pediatric FEESST Fiberoptic Endoscopic Evaluation of Swallowing With Sensory TestingDocument4 pages(MO-CHILE) Willging J., Et Al. Pediatric FEESST Fiberoptic Endoscopic Evaluation of Swallowing With Sensory TestingCamila CárcamoNo ratings yet
- PAPER (ENG) - Effect of A Tracheostomy Speaking Valve On Breathing-Swallowing InteractionDocument7 pagesPAPER (ENG) - Effect of A Tracheostomy Speaking Valve On Breathing-Swallowing InteractionAldo Hip NaranjoNo ratings yet
- Wang, CH Et Al (2016) Non-Invasive Assessment of Swallowing and Respiration Coordination For The OSA Patient.Document10 pagesWang, CH Et Al (2016) Non-Invasive Assessment of Swallowing and Respiration Coordination For The OSA Patient.Carla Francisca Rojas MerelloNo ratings yet
- Airway Management During Upper GI Endoscopic Procedures2016Document9 pagesAirway Management During Upper GI Endoscopic Procedures2016jcarl_20063003No ratings yet
- Tissue-Preserving Techniques for Tonsillectomy and PharyngoplastyDocument6 pagesTissue-Preserving Techniques for Tonsillectomy and Pharyngoplastylaljadeff12No ratings yet
- Managing Airway, Feeding and Hearing Challenges in Pierre Robin SequenceDocument4 pagesManaging Airway, Feeding and Hearing Challenges in Pierre Robin SequenceJaavyeraa' BelenNo ratings yet
- Laryngospasm in Paediatric Anaesthesia: Causes, Treatment and PreventionDocument7 pagesLaryngospasm in Paediatric Anaesthesia: Causes, Treatment and PreventionSebastian Castro TigheNo ratings yet
- LX Suspension and UES Myotomy Kos 2008Document7 pagesLX Suspension and UES Myotomy Kos 2008DEVNo ratings yet
- Oral Rehydration Therapy For Preoperative Fluid and Electrolyte Man-AgementDocument9 pagesOral Rehydration Therapy For Preoperative Fluid and Electrolyte Man-AgementSasmira JamalNo ratings yet
- FulltextDocument7 pagesFulltextNicolas CruzNo ratings yet
- HOUGH 2014_Lung recruitment and endotracheal suction in ventilated preterm infants measured with electrical impedance tomographyDocument7 pagesHOUGH 2014_Lung recruitment and endotracheal suction in ventilated preterm infants measured with electrical impedance tomographyRafael JustinoNo ratings yet
- Non-Invasive Assessment Determine The Swallowing and RespirationDocument6 pagesNon-Invasive Assessment Determine The Swallowing and RespirationDaniela OrtizNo ratings yet
- Induced SputumDocument6 pagesInduced Sputumnh2411No ratings yet
- Synosis Finl JDocument7 pagesSynosis Finl JPrasanna MarandiNo ratings yet
- Aspiration: Definition: The Passage of Secretions Beyond The V.CDocument5 pagesAspiration: Definition: The Passage of Secretions Beyond The V.Cadham bani younesNo ratings yet
- Assessing Palatal Mobility in Post-Tonsillectomy Patients: Egyptian Journal of Ear, Nose, Throat and Allied SciencesDocument3 pagesAssessing Palatal Mobility in Post-Tonsillectomy Patients: Egyptian Journal of Ear, Nose, Throat and Allied SciencesYessyParamitaNo ratings yet
- Operative Techniques in Otolaryngology (2015) 26, 78–84: The Uvulopalatal FlapDocument7 pagesOperative Techniques in Otolaryngology (2015) 26, 78–84: The Uvulopalatal FlapbarbiemeNo ratings yet
- SuctioningDocument7 pagesSuctioningKat AlaNo ratings yet
- Grand Rounds Index UTMB Otolaryngology Home PageDocument12 pagesGrand Rounds Index UTMB Otolaryngology Home Pagegdudex118811No ratings yet
- Layryngeal Mask Airway Placement: A Comparison Between Propofol and Thiopentone Sodium in The Day Case SurgeryDocument5 pagesLayryngeal Mask Airway Placement: A Comparison Between Propofol and Thiopentone Sodium in The Day Case SurgeryAzzam Saqr100% (1)
- Recurrent Postoperative Laryngospasm ManagementDocument2 pagesRecurrent Postoperative Laryngospasm Managementbalab2311No ratings yet
- Otic Solution Ke Sistemik PDFDocument6 pagesOtic Solution Ke Sistemik PDFdenaNo ratings yet
- J Ijporl 2012 07 023Document3 pagesJ Ijporl 2012 07 023Nida Fariza MaulanisaNo ratings yet
- Nasoendoscopy of Velopharynx Before and During Diagnostic TherapyDocument8 pagesNasoendoscopy of Velopharynx Before and During Diagnostic TherapyValentina SalasNo ratings yet
- Journal English AsliDocument19 pagesJournal English AslidenokkosasiNo ratings yet
- 118 Reignier2010Document7 pages118 Reignier2010tereNo ratings yet
- 1678 4219 Ag s0004280320200000028 PDFDocument4 pages1678 4219 Ag s0004280320200000028 PDFTOMOKO TERUYANo ratings yet
- 2017 Whats New in Cleft Palate and VelopharyngealDocument13 pages2017 Whats New in Cleft Palate and VelopharyngealDimitris RodriguezNo ratings yet
- Swallowing Disorders in Tracheostomised Patients: A Multidisciplinary/multiprofessional Approach in Decannulation ProtocolsDocument10 pagesSwallowing Disorders in Tracheostomised Patients: A Multidisciplinary/multiprofessional Approach in Decannulation ProtocolsCarolina Andrea Vasquez HenriquezNo ratings yet
- RetrieveDocument11 pagesRetrieveSantiago PortillaNo ratings yet
- Guide to Nasojejunal Tube Placement TechniquesDocument12 pagesGuide to Nasojejunal Tube Placement TechniquesIssa AbuzeidNo ratings yet
- Von Goedecke Et Al 2004 Positive Pressure Versus Pressure Support Ventilation at Different Levels of Peep Using TheDocument5 pagesVon Goedecke Et Al 2004 Positive Pressure Versus Pressure Support Ventilation at Different Levels of Peep Using TheDr MunawarNo ratings yet
- Endoscopically Guided Nasojejunal Tube Placement in Dogs For Short-Term Postduodenal FeedingDocument10 pagesEndoscopically Guided Nasojejunal Tube Placement in Dogs For Short-Term Postduodenal FeedingsoledadDC329No ratings yet
- Changes and Recovery of Voice Quality After Sinonasal SurgeryDocument7 pagesChanges and Recovery of Voice Quality After Sinonasal SurgeryEunike KaramoyNo ratings yet
- Original Articles: Proton Pump Inhibitor Therapy For Chronic Laryngo-Pharyngitis: A Randomized Placebo-Control TrialDocument9 pagesOriginal Articles: Proton Pump Inhibitor Therapy For Chronic Laryngo-Pharyngitis: A Randomized Placebo-Control TrialAnonymous iM2totBrNo ratings yet
- Signs and Symptoms of Abnormal Swallow: Aspiration (Coughing, Choking)Document2 pagesSigns and Symptoms of Abnormal Swallow: Aspiration (Coughing, Choking)Anda DorofteiNo ratings yet
- Factors On Thesis Writing Anxiety Among Science, Technology, Engineering, and Mathematics StudentsDocument9 pagesFactors On Thesis Writing Anxiety Among Science, Technology, Engineering, and Mathematics StudentsPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Myths and Facts About Guidance and CounsellingDocument4 pagesMyths and Facts About Guidance and CounsellingEfren Jonicel DomingoNo ratings yet
- Womens Basketball Spring Strength Training-2Document1 pageWomens Basketball Spring Strength Training-2api-548848665No ratings yet
- Practical Research OrigDocument37 pagesPractical Research OrigKillua ZoldyckNo ratings yet
- Growth and Development of Feedlot CattleDocument21 pagesGrowth and Development of Feedlot CattleHenry JoséNo ratings yet
- Mind MappingDocument23 pagesMind MappingVIMAL NAIR SURESHNo ratings yet
- Orthotropics: Building Great Faces One Bite at A TimeDocument21 pagesOrthotropics: Building Great Faces One Bite at A TimeДаша ХмызоваNo ratings yet
- Expat Insider 2019 - The InterNations Survey - 0Document116 pagesExpat Insider 2019 - The InterNations Survey - 0tarmiricmyNo ratings yet
- Lutz, Nutrition and Diet Therapy 6e ETBDocument15 pagesLutz, Nutrition and Diet Therapy 6e ETBShelly-ann Richards-FrancisNo ratings yet
- Philippine National Philippine National Philippine National Philippine National Standard Standard Standard StandardDocument14 pagesPhilippine National Philippine National Philippine National Philippine National Standard Standard Standard StandardGaily HontiverosNo ratings yet
- Case Study Orientation SlidesDocument88 pagesCase Study Orientation SlidesJoseph Emmanuel CandaNo ratings yet
- SDTM Paired View 2020-12-18Document2,732 pagesSDTM Paired View 2020-12-18pathuri rangaNo ratings yet
- GED0004, Physical Education 1Document4 pagesGED0004, Physical Education 1Gheoff RicareNo ratings yet
- Teaching Demonstration Activity Guide Template PDFDocument3 pagesTeaching Demonstration Activity Guide Template PDFRosarioEsperManisanNo ratings yet
- Aplus Compendium PharmaDocument147 pagesAplus Compendium PharmaRhosalie G. Cruz100% (1)
- ReviewerDocument6 pagesReviewerChay ChayNo ratings yet
- CHCCCS025 Support Relationships With Carers and Families EKDocument67 pagesCHCCCS025 Support Relationships With Carers and Families EKIkhsan Misbahuddin75% (8)
- Academic style nominalisationDocument2 pagesAcademic style nominalisationJamie Leigh McGeorgeNo ratings yet
- Application LetterDocument1 pageApplication LetterWetzell PornelNo ratings yet
- SHS Student Handbook 2023 Ed v2Document154 pagesSHS Student Handbook 2023 Ed v2Alvin Xtian NucumNo ratings yet
- Ida InfographicDocument2 pagesIda InfographicErica Lim MagtuloyNo ratings yet
- Jacm 37 1 2013 10 15 Azam 1 sdc1Document2 pagesJacm 37 1 2013 10 15 Azam 1 sdc1Mohamed ElshahidiNo ratings yet
- Peh 11 FidpDocument15 pagesPeh 11 FidpCris SimonNo ratings yet
- CBTDocument2 pagesCBTTanvi ManjrekarNo ratings yet
- Assessing Agricultural Innovation SystemsDocument106 pagesAssessing Agricultural Innovation SystemsAndre RDNo ratings yet
- How Do You Assess Biopure's Potential in The Human Market? The Animal Market? Human MarketDocument8 pagesHow Do You Assess Biopure's Potential in The Human Market? The Animal Market? Human MarketYilei RenNo ratings yet
- Lecture 5 Brachytherapy Implantation - 6-18 FinalDocument10 pagesLecture 5 Brachytherapy Implantation - 6-18 FinalArcrije JerezNo ratings yet
- The Hold Me Tight Workbook - Dr. Sue JohnsonDocument187 pagesThe Hold Me Tight Workbook - Dr. Sue JohnsonMoh100% (8)
- Ceylon Cinnamon ReviewDocument11 pagesCeylon Cinnamon ReviewSuresh KumarNo ratings yet
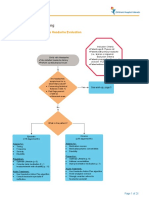
- Headache Clinical PathwayDocument25 pagesHeadache Clinical PathwayKoushik Mazumder ShuvoNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)