You might also like
- Ce 45Document5 pagesCe 45Aman AmanNo ratings yet
- 7db29e88characterization of HospitalDocument13 pages7db29e88characterization of HospitalDien NoelNo ratings yet
- Health Risk Assessments of Arsenic and Toxic Heavy Metal Exposure in Drinking Water in Northeast IranDocument17 pagesHealth Risk Assessments of Arsenic and Toxic Heavy Metal Exposure in Drinking Water in Northeast IranSiti khairuni taniahNo ratings yet
- Ijerph 16 01803Document15 pagesIjerph 16 01803VINAY B K ECENo ratings yet
- Chemistry and Water: The Science Behind Sustaining the World's Most Crucial ResourceFrom EverandChemistry and Water: The Science Behind Sustaining the World's Most Crucial ResourceNo ratings yet
- Sources of and Solutions To Toxic Metal and Metalloid Contamination in Small Rural Drinking Water Systems: A Rapid ReviewDocument18 pagesSources of and Solutions To Toxic Metal and Metalloid Contamination in Small Rural Drinking Water Systems: A Rapid ReviewEdukondalu BNo ratings yet
- Evaluating Water Quality to Prevent Future DisastersFrom EverandEvaluating Water Quality to Prevent Future DisastersNo ratings yet
- Case analysis of Cr pollution and health risksDocument4 pagesCase analysis of Cr pollution and health risksJenny Lorena BerrioNo ratings yet
- MVMJ - Volume 23 - Issue 2 - Pages 48-52Document5 pagesMVMJ - Volume 23 - Issue 2 - Pages 48-52HebaNo ratings yet
- STP REPORT by KhemrajDocument26 pagesSTP REPORT by Khemrajall rounder shanNo ratings yet
- Chromium Exposure Study in Chemical Based IndustryDocument4 pagesChromium Exposure Study in Chemical Based IndustryTaraNewleafNo ratings yet
- Synthesis of Calcite-Based Bio-Composite Biochar For Enhanced Biosorption and Detoxification of Chromium CR (VI) by Zhihengliuella Sp. ISTPL4Document8 pagesSynthesis of Calcite-Based Bio-Composite Biochar For Enhanced Biosorption and Detoxification of Chromium CR (VI) by Zhihengliuella Sp. ISTPL4Edilberto Murrieta LunaNo ratings yet
- Unidad 2 Task 4Document3 pagesUnidad 2 Task 4Yesica GarciaNo ratings yet
- Univeridad Nacional Abierta Y A Distancia UnadDocument3 pagesUniveridad Nacional Abierta Y A Distancia UnadYesica GarciaNo ratings yet
- Eloor Industrial Health Study - Research Adviser-Dr. Rajan R PatilDocument27 pagesEloor Industrial Health Study - Research Adviser-Dr. Rajan R PatilDr. Rajan R PatilNo ratings yet
- Iris PDFDocument33 pagesIris PDFmela firdaustNo ratings yet
- Presence of Coliform and Fecal Coliform and Evaluation of The Drinking Water Quality in Chittagong University CampusDocument6 pagesPresence of Coliform and Fecal Coliform and Evaluation of The Drinking Water Quality in Chittagong University CampusRohit KumarNo ratings yet
- Article1381156255 - Juneja and ChaudharyDocument6 pagesArticle1381156255 - Juneja and ChaudharyWijetunga SomasiriNo ratings yet
- Science of The Total EnvironmentDocument11 pagesScience of The Total EnvironmentUsman AliNo ratings yet
- Effectiveness of Wastewater Treatment Systems in Removing Microbial Agents: A Systematic ReviewDocument11 pagesEffectiveness of Wastewater Treatment Systems in Removing Microbial Agents: A Systematic ReviewPaulo PangilinanNo ratings yet
- Case Study Chromium Pollution Health Effects BangladeshDocument4 pagesCase Study Chromium Pollution Health Effects BangladeshJhon Alexander RivasNo ratings yet
- NOV162709Document5 pagesNOV162709Atheena AthiNo ratings yet
- A National Wastewater Monitoring Program For A Better Understanding ofDocument12 pagesA National Wastewater Monitoring Program For A Better Understanding ofValentina Rico BermudezNo ratings yet
- EASJNFS 22 33-38 8h8ItaLDocument6 pagesEASJNFS 22 33-38 8h8ItaLAndi FakhruddinNo ratings yet
- Ali Akbar MohammadiDocument10 pagesAli Akbar MohammadiElizabeth FigueroaNo ratings yet
- Reverse Osmosis Plant Maintenance and Efficacy in Chronic Kidney Disease Endemic Region in Sri LankaDocument6 pagesReverse Osmosis Plant Maintenance and Efficacy in Chronic Kidney Disease Endemic Region in Sri LankaChanna JayasumanaNo ratings yet
- Heavy Metals in Surface and GroundwaterDocument7 pagesHeavy Metals in Surface and GroundwaterZayeed Khalifa KithyNo ratings yet
- Environmental Health - SampleDocument4 pagesEnvironmental Health - SampleRich Lopez AlmarioNo ratings yet
- High-Risk Pollutants in WastewaterFrom EverandHigh-Risk Pollutants in WastewaterHongqiang RenNo ratings yet
- Permissible Limit of Drinking WaterDocument6 pagesPermissible Limit of Drinking WaterronitNo ratings yet
- Chromium (VI) CASRN 18540-29-9: Iris Assessment Development ProcessDocument33 pagesChromium (VI) CASRN 18540-29-9: Iris Assessment Development ProcessAngga SulistyoNo ratings yet
- IOSR JournalsDocument6 pagesIOSR JournalsInternational Organization of Scientific Research (IOSR)No ratings yet
- Fisika Dasar 1Document10 pagesFisika Dasar 1priskaNo ratings yet
- Journal of Cleaner ProductionDocument11 pagesJournal of Cleaner Production陳奕捷No ratings yet
- Paper-Based Biosensor For Early Detection of Oral CancerDocument8 pagesPaper-Based Biosensor For Early Detection of Oral CancerBIJCRNo ratings yet
- WaterqualityDocument9 pagesWaterqualityMoin PinjariNo ratings yet
- Relationship between cytokines and hazards in waste workersDocument8 pagesRelationship between cytokines and hazards in waste workersSalsa BilaNo ratings yet
- Chapter One 1.0 1.1 Background of The StudyDocument3 pagesChapter One 1.0 1.1 Background of The StudySamson DeCasparNo ratings yet
- ChromiumDocument11 pagesChromiumyanti permadiNo ratings yet
- Analysis of Some Pharmaceuticals in Municipal Wastewa - 2017 - Arabian Journal oDocument11 pagesAnalysis of Some Pharmaceuticals in Municipal Wastewa - 2017 - Arabian Journal olucian_lovNo ratings yet
- 182 PDFDocument10 pages182 PDFDEVA PRIYA ANIL 1861724No ratings yet
- Wolayita Sodo Hospital Waste Water EvaluationDocument9 pagesWolayita Sodo Hospital Waste Water EvaluationFasil GeberemeskelNo ratings yet
- Inorganic Contaminants and RadionuclidesFrom EverandInorganic Contaminants and RadionuclidesRavi NaiduNo ratings yet
- Evaluation of Drinking Water Quality in Urban Areas of Pakistan. A Case Study of Gulshan-e-Iqbal Karachi, PakistanDocument13 pagesEvaluation of Drinking Water Quality in Urban Areas of Pakistan. A Case Study of Gulshan-e-Iqbal Karachi, PakistanMd Ashikur RahmanNo ratings yet
- Changes in Cadmium Exposure Among Persons Living IDocument7 pagesChanges in Cadmium Exposure Among Persons Living Imelisa kurniaNo ratings yet
- Andrew y ColsDocument8 pagesAndrew y ColsRocio TerronesNo ratings yet
- Environmental Forensics for Persistent Organic PollutantsFrom EverandEnvironmental Forensics for Persistent Organic PollutantsGwen O'SullivanNo ratings yet
- PLOMODocument8 pagesPLOMODaniel ManriqueNo ratings yet
- Journal of Environmental Science and Engineering, Vol.7, No.1A, 2018Document53 pagesJournal of Environmental Science and Engineering, Vol.7, No.1A, 2018Anonymous 0K8PXYNo ratings yet
- Task 4 - Case Analysis of A DocumentDocument4 pagesTask 4 - Case Analysis of A DocumentzullyNo ratings yet
- Ge0-803 Academic Task-1 Research Paper OnDocument12 pagesGe0-803 Academic Task-1 Research Paper Onojaswi malikNo ratings yet
- Public Health Quality of Drinking Water Supply in Orangi Town, Karachi, PakistanDocument7 pagesPublic Health Quality of Drinking Water Supply in Orangi Town, Karachi, PakistanAaina OwaisNo ratings yet
- Waste Water Characteristics of HospitalsDocument5 pagesWaste Water Characteristics of HospitalsVelram ShanmugamNo ratings yet
- Filling Stations and Their Effects On Groundwater Quality in Ilorin MetropolisDocument12 pagesFilling Stations and Their Effects On Groundwater Quality in Ilorin MetropolisGramIQNo ratings yet
- Association Between Outdoor Air Pollution and Cardiovascular Mortality in BangaloreDocument7 pagesAssociation Between Outdoor Air Pollution and Cardiovascular Mortality in BangaloreshamalaksNo ratings yet
- AfixedBe - CR VI 2020Document10 pagesAfixedBe - CR VI 2020Anonymous NSbxWMNo ratings yet
- Serum Organochlorine Pesticides Residues and Risk - 2018 - Saudi Journal of BiolDocument7 pagesSerum Organochlorine Pesticides Residues and Risk - 2018 - Saudi Journal of BiolErick Dario P ChNo ratings yet
- Total Dissolved Solids ELKENDocument8 pagesTotal Dissolved Solids ELKENLaurence MalanumNo ratings yet
- Assessment of Heavy Metals Content in Sewage Discharges From Health Structure in MauritaniaDocument5 pagesAssessment of Heavy Metals Content in Sewage Discharges From Health Structure in MauritaniaSabrina JonesNo ratings yet
- Ion Exchange&psuedo First Order ReactionDocument11 pagesIon Exchange&psuedo First Order ReactionMouna GuruNo ratings yet
- School of Architecture, Building and Civil Engineering Assessment BriefDocument2 pagesSchool of Architecture, Building and Civil Engineering Assessment BriefMouna GuruNo ratings yet
- BTCMDocument59 pagesBTCMMouna GuruNo ratings yet
- Assessing and Managing Environmental Impacts in Existing Dam ProjectsDocument250 pagesAssessing and Managing Environmental Impacts in Existing Dam ProjectsMouna GuruNo ratings yet
- Recruitment Revised+publish+spl+advertisment25.10.2020+-++ (1) 123c58e59d PDFDocument9 pagesRecruitment Revised+publish+spl+advertisment25.10.2020+-++ (1) 123c58e59d PDFAkhil AntonyNo ratings yet
- Strength of Materials by R.K.bansalDocument611 pagesStrength of Materials by R.K.bansalMouna GuruNo ratings yet
- Health Effects InformationDocument5 pagesHealth Effects InformationMouna GuruNo ratings yet
- OlympicDocument5 pagesOlympicMouna GuruNo ratings yet
- Steel Design by GuruDocument305 pagesSteel Design by GuruMouna GuruNo ratings yet
- Methods for Improving Anaerobic Lignocellulosic DegradationDocument11 pagesMethods for Improving Anaerobic Lignocellulosic DegradationMouna GuruNo ratings yet
- Chromium pollution threatens environmentDocument5 pagesChromium pollution threatens environmentMouna GuruNo ratings yet
- Data 1Document5 pagesData 1Mouna GuruNo ratings yet
- Mock Questions: ConciseDocument10 pagesMock Questions: ConcisePanchami Borpujari33% (3)
- Work PlanDocument2 pagesWork PlanMouna GuruNo ratings yet
- Recruitment of Assistants (Assistant Section Officier)Document2 pagesRecruitment of Assistants (Assistant Section Officier)Mouna GuruNo ratings yet
- Microbial Enzyme Production Using Lignocellulosic Food Industry Wastes As Feedstock: A ReviewDocument22 pagesMicrobial Enzyme Production Using Lignocellulosic Food Industry Wastes As Feedstock: A ReviewMouna GuruNo ratings yet
- Total Number of TanneriesDocument1 pageTotal Number of TanneriesMouna GuruNo ratings yet
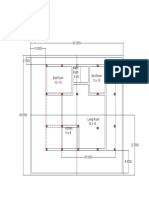
- Plan ModelDocument1 pagePlan ModelMouna GuruNo ratings yet
- Bromatological, Proximate and Ultimate Analysis of OFMSW For Di Collection SystemsDocument20 pagesBromatological, Proximate and Ultimate Analysis of OFMSW For Di Collection SystemsJessica Asitimbay ZuritaNo ratings yet
- Details NeededDocument2 pagesDetails NeededMouna GuruNo ratings yet
- Waste Management: K. Ziemin Ski, I. Romanowska, M. KowalskaDocument7 pagesWaste Management: K. Ziemin Ski, I. Romanowska, M. KowalskaMayra UlínNo ratings yet
- REFERENCESDocument2 pagesREFERENCESMouna GuruNo ratings yet
- Shan Mug Am 2009Document4 pagesShan Mug Am 2009Mouna GuruNo ratings yet
- REFERENCESDocument2 pagesREFERENCESMouna GuruNo ratings yet
- Question No - 5 Date - 15/06/2020 Ans 2Document1 pageQuestion No - 5 Date - 15/06/2020 Ans 2Mouna GuruNo ratings yet
- Recruitment of Probationary OfficersDocument4 pagesRecruitment of Probationary OfficersMouna GuruNo ratings yet
- Analytical LabDocument1 pageAnalytical LabMouna GuruNo ratings yet
- REFERENCESDocument2 pagesREFERENCESMouna GuruNo ratings yet
- Work Plan PDFDocument1 pageWork Plan PDFMouna GuruNo ratings yet
- Clinical Importance of Pittadhara KalaDocument61 pagesClinical Importance of Pittadhara KalaSwanand Avinash JoshiNo ratings yet
- Patient Care in Radiography 8th Edition Ehrlich Test BankDocument5 pagesPatient Care in Radiography 8th Edition Ehrlich Test Bankselinadu4in1100% (22)
- ROO-ALL-HS-PRO-0025 REV 10 Ground Disturbance and Excavation Procedure - ...Document25 pagesROO-ALL-HS-PRO-0025 REV 10 Ground Disturbance and Excavation Procedure - ...Murtadda MohammedNo ratings yet
- Introduction To Consumer Behaviour: Oxford University Press Sample ChapterDocument51 pagesIntroduction To Consumer Behaviour: Oxford University Press Sample ChapterMuhammad Imran AwanNo ratings yet
- Rusty Moore Visual Impact For WomenDocument34 pagesRusty Moore Visual Impact For Womenchrisie00757% (7)
- Konsep Kebidanan KomunitasDocument63 pagesKonsep Kebidanan Komunitasdewi susilawatiNo ratings yet
- DFGHDocument6 pagesDFGHManuelEduardoSanchezSotoNo ratings yet
- Navigating The Labyrinth of Love 2013cDocument15 pagesNavigating The Labyrinth of Love 2013cvictoriaNo ratings yet
- Adjuvant Analgesics (2015) PDFDocument177 pagesAdjuvant Analgesics (2015) PDFsatriomega100% (1)
- HerbicidesDocument28 pagesHerbicidesDr.KanamNo ratings yet
- Dental CariesDocument42 pagesDental Cariesyongky100% (1)
- Nutritious Philippine Herbs Combat MalnutritionDocument5 pagesNutritious Philippine Herbs Combat MalnutritionPeter Pantazia0% (1)
- Problems: 5: VancomycinDocument4 pagesProblems: 5: VancomycinSaul RuizNo ratings yet
- MELC-Based Health PresentationDocument17 pagesMELC-Based Health PresentationNelson Manalo88% (8)
- The Zone Issue 27Document16 pagesThe Zone Issue 27Jeff Clay GarciaNo ratings yet
- Chapter 6 - Adipose TissueDocument13 pagesChapter 6 - Adipose TissueREMAN ALINGASANo ratings yet
- Acute Pain Questions - LathaDocument5 pagesAcute Pain Questions - LathaNishanth yedavalliNo ratings yet
- Thesis PPT For VivaDocument62 pagesThesis PPT For VivaNamrata DahakeNo ratings yet
- RAPID Resources for Lowering Fertility and Achieving Sustainable Development in the PhilippinesDocument41 pagesRAPID Resources for Lowering Fertility and Achieving Sustainable Development in the PhilippinesLeyrra Paclibar DiduloNo ratings yet
- PR 2Document14 pagesPR 2Eduardo TalamanNo ratings yet
- CBT therapy overview: strengths, sessions, evidenceDocument1 pageCBT therapy overview: strengths, sessions, evidencezulkaberNo ratings yet
- Medication Booklet and TicketDocument3 pagesMedication Booklet and TicketCayanne ChuaNo ratings yet
- Test Bank For Essentials of Pediatric Nursing 1st Edition Theresa KyleDocument13 pagesTest Bank For Essentials of Pediatric Nursing 1st Edition Theresa KyleAnthonyRiveraqion100% (33)
- Pathophysiology of PneumoniaDocument2 pagesPathophysiology of PneumoniaJeffrey Ramos100% (1)
- DM-PH&SD-GU17-HCKS2 - Health Requirements For Kids SalonsDocument13 pagesDM-PH&SD-GU17-HCKS2 - Health Requirements For Kids SalonsPraveenKatkooriNo ratings yet
- Mapeh 10 Week 1 Week 2Document12 pagesMapeh 10 Week 1 Week 2Christian Paul YusiNo ratings yet
- Registrar:: Section 3C: ISO 14001 Audit Criteria (Significant Environmental Aspects)Document1 pageRegistrar:: Section 3C: ISO 14001 Audit Criteria (Significant Environmental Aspects)Tathiana GarcíaNo ratings yet
- Abc of Burns: Kanwal Khan Lecturer ZCPTDocument35 pagesAbc of Burns: Kanwal Khan Lecturer ZCPTKanwal KhanNo ratings yet
- What Is MindfulnessDocument4 pagesWhat Is MindfulnessPongal PunithaNo ratings yet
- The Six Killer DiseaseDocument26 pagesThe Six Killer DiseaseFrancis Luke63% (8)