Professional Documents
Culture Documents
Popescu 2013
Popescu 2013
Uploaded by
jhidalgomdCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Popescu 2013
Popescu 2013
Uploaded by
jhidalgomdCopyright:
Available Formats
Review Article
Pathology of Multiple
Address correspondence to
Dr Claudia F. Lucchinetti,
Department of Neurology,
Mayo Clinic College of
Sclerosis: Where Do Medicine, 200 First St
Southwest, Rochester,
MN 55905,
We Stand? lucchinetti.claudia@mayo.edu.
Relationship Disclosure:
Dr Popescu has served as a
speaker for Teva Canada
Bogdan F. Gh. Popescu, MD, PhD; Istvan Pirko, MD, FAAN; Innovation and receives
Claudia F. Lucchinetti, MD, FAAN research support from the
Canada Research Chairs
program and the Saskatchewan
Health Research Foundation.
ABSTRACT Dr Pirko serves as the clinical
editor of Nanomedicine:
Purpose of Review: This article summarizes the pathologic features of multiple Nanotechnology, Biology and
sclerosis (MS) and other inflammatory demyelinating diseases and discusses neuro- Medicine and receives
pathologic studies that have yielded novel insights into potential mechanisms of research support from the NIH.
Dr Lucchinetti holds a patent
demyelination. for aquaporin-4Yassociated
Recent Findings: The pathologic hallmark of MS consists of focal demyelinated plaques antibodies for the diagnosis of
within the CNS, with variable degrees of inflammation, gliosis, and neurodegeneration. neuromyelitis optica; receives
royalties from Elsevier for the
Active MS lesions show a profound pathologic heterogeneity with four major pat- publication of Blue Books of
terns of immunopathology, suggesting that the targets of injury and mechanisms of Neurology: Multiple Sclerosis;
demyelination in MS may be different in different disease subgroups. Recent path- and receives research support
from Guthy-Jackson Charitable
ologic studies have suggested that the subarachnoid space and cortex may be initial Foundation, the National
sites and targets of the MS disease process, that inflammatory cortical demyelination Multiple Sclerosis Society,
is present early in MS, and that meningeal inflammation may drive cortical and white and the NIH.
matter injury in some MS patients. Unlabeled Use of
Products/Investigational
Summary: MS is heterogeneous with respect to clinical, genetic, radiographic, and Use Disclosure:
pathologic features; surrogate MRI, clinical, genetic, serologic, and/or CSF markers for Drs Popescu, Pirko, and
each of the four immunopatterns need to be developed in order to recognize them in Lucchinetti report no
disclosures.
the general nonbiopsied MS population. Inflammatory cortical demyelination is an
* 2013, American Academy
important early event in the pathogenesis of MS and may be driven by meningeal of Neurology.
inflammation. These observations stress the importance of developing imaging
techniques able to capture early inflammatory cortical demyelination in order to better
understand the disease pathogenesis and to determine the impact of potential disease-
modifying therapies on the cortex.
Continuum (Minneap Minn) 2013;19(4):901–921.
INTRODUCTION Although MS has historically been con-
The pathologic hallmark of multiple sidered a disease primarily affecting
sclerosis (MS) is multiple focal areas of the CNS white matter, recent patho-
myelin loss within the CNS called plaques logic and imaging studies have
or lesions (Figure 1-1A–C).1,2 Demyelin- established that demyelinated lesions
ation is accompanied by variable gliosis are also commonly found in the corti-
and inflammation and by relative axo- cal gray matter of MS patients.3Y6
nal preservation (Figure 1-1D–I). Le-
sions are disseminated throughout the NEUROPATHOLOGY OF WHITE
CNS but have a predilection for optic MATTER LESIONS
nerves, subpial spinal cord, brainstem, MS lesions evolve differently during
cerebellum, and juxtacortical and peri- early versus chronic disease phases,
ventricular white matter regions.1,2 and within each phase, different plaque
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 901
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
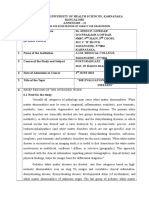
FIGURE 1-1 Immunopattern II multiple sclerosis lesion. A, Demyelination demonstrated as loss of immunohistochemical
(IHC) staining. The myelin protein proteolipid protein (PLP) (arrow indicates a perivascular inflammatory
infiltrate) (scale bar = 250 2m). B, The myelin protein myelin oligodendrocyte glycoprotein (scale bar = 250 2m).
C, The myelin protein myelin-associated glycoprotein (scale bar = 250 2m). D, Active demyelination evidenced by the presence
of myelin-laden macrophages (arrows) (PLP IHC, scale bar = 50 2m); E, Sea of macrophages (IHC for KiM1P, a panmacrophage
marker, scale bar = 100 2m). F, T-cell perivascular inflammatory infiltrate (arrow) (IHC for cluster of differentiation 3, a marker
common to all lymphocytes, scale bar = 50 2m). G, Complement activation on axons (black arrows) and phagocytosis of
complement-opsonized myelin debris by macrophages (white arrow) (IHC for neoepitope on the complement component C9
of the terminal lytic complex, scale bar = 50 2m). H, Reactive astrocyte (arrows) and Creutzfeldt-Peters cells (reactive astrocytes
with abundant cytoplasm and fragmented nuclear inclusions arranged in a circular pattern) (inset) (hematoxylin and eosin stain,
scale bar = 100 2m, inset scale bar = 50 2m). I, Relative axonal preservation within the multiple sclerosis lesion (arrows indicate
the lesion’s edge) (Bielschowsky stain, scale bar = 100 2m).
KEY POINT types and plaques in different stages of demyelinating lesions as consistent with
h The pathologic hallmark demyelinating activity are evident. His- MS: hematoxylin and eosin stain (dem-
of multiple sclerosis is tologically, several basic processes drive onstrates tissue and cell morphology),
multiple focal areas of
the formation of plaques: inflammation, myelin stains (Luxol fast blue/periodic
myelin loss within the
myelin breakdown, astrogliosis, oligo- acid-Schiff, Luxol fast blue/hematoxylin/
CNS called plaques or
lesions, accompanied
dendrocyte injury, neurodegeneration eosin, or immunohistochemistry for
by variable gliosis and and axonal loss, and remyelination. A myelin proteins), macrophage-specific
inflammation and by combination of histologic and/or immu- markers (immunohistochemistry for
relative axonal nohistochemical stains can be used to KiM1P or CD68), stains for axons
preservation. visualize these processes and to neuro- (Bielschowsky silver impregnation or im-
pathologically diagnose inflammatory munohistochemistry for neurofilament
902 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
protein), stains for astrocytes (hema- lesions are infiltrated by macrophages h Active multiple sclerosis
toxylin and eosin or immunohisto- that lack myelin debris, but may still lesions are infiltrated
chemistry for glial fibrillary acidic contain empty vacuoles or periodic by macrophages
protein), and stains for the different acid-SchiffYpositive degradation prod- containing myelin
lymphocyte subtypes (immunohisto- ucts, the result of the macrophage’s debris.
chemistry for CD3, CD4, CD8, CD20, inability to digest the myelin’s neutral h Lymphocytic
and/or CD138).7 lipid components that accumulate and inflammatory infiltrates
persist in macrophages. in multiple sclerosis are
Acute Active Plaques Perivascular and parenchymal in- composed mainly of
Acute active plaques are most frequent flammatory infiltrates are invariably CD8-positive cytotoxic
in acute and relapsing-remitting MS present, suggesting that demyelin- T lymphocytes, and
and represent the pathologic substrate ation and axonal degeneration are fewer CD4-positive
of clinical attacks.1,8,9 Acute active MS inflammatory in nature (Figure 1-1A, helper T cells, B cells,
lesions are hypercellular demyelinated Figure 1-1D–F).1,2,11,12 Besides acti- and plasma cells,
unlike experimental
plaques massively infiltrated by mac- vated macrophages/microglia, inflam-
autoimmune
rophages evenly distributed through- matory infiltrates are composed of
encephalomyelitis
out the lesion forming the classic ‘‘sea lymphocytes, the vast majority of which models in which
of macrophages’’ (Figure 1-1E). These are CD8-positive cytotoxic T lympho- inflammation starts
macrophages contain myelin debris, cytes, and fewer CD4-positive helper T with profound
an indication that they have taken up cells, B cells, and plasma cells. B cells infiltration of the tissue
and degraded the remnants of the and plasma cells tend to accumulate by CD4-positive T cells.
destroyed myelin sheaths (ie, active predominantly in the perivascular h Gadolinium
demyelination) (Figure 1-1D). The spaces.11 Gadolinium enhancement enhancement
progression of myelin fragment degra- characterizes lesions with damaged characterizes lesions
dation by macrophages is reflected in blood-brain barrier (BBB), which en- with a damaged
different rates of their disappearance. ables infiltration of inflammatory cells blood-brain barrier,
Therefore, a stringent definition of de- into the CNS. The inflammation to- which enables the
myelinating activity within a plaque can gether with the demyelination and infiltration of
be obtained on the basis of the pres- vasogenic edema present in early MS inflammatory cells
ence or absence of certain myelin lesions are responsible for their into the CNS.
degradation products within macro- pinkish-yellow, soft, and poorly demar-
phages.10 Degradation of minor myelin cated appearance on fresh slices of
proteins (2¶,3¶-cyclic nucleotide 3¶- brain and spinal cord.
phosphodiesterase [CNPase], myelin Astrocytes in active lesions prolifer-
oligodendrocyte glycoprotein, myelin- ate and become plump-shaped
associated glycoprotein [MAG]) occurs (gemistocytes) with homogeneous eo-
rapidly, within 1 to 3 days, and the sinophilic cytoplasm and numerous
presence of minor myelin protein deg- fibrillary processes (Figure 1-1H).1,2
radation products within macrophages Prominent uninucleated and multi-
denotes early active demyelination. nucleated reactive astrocytes with eo-
The larger, more abundant and hydro- sinophilic hypertrophic cell bodies
phobic major myelin proteins (pro- form a matrix in which the other cells
teolipid protein, myelin basic protein) are suspended. Mitotic astrocytes and
are digested more slowly and may per- astrocytes with fragmented nuclear
sist in lesions for up to 10 days. Thus, inclusions (granular mitoses and
the presence of major myelin protein Creutzfeldt-Peters cells) are also often
but not minor myelin protein degrada- found within early lesions (Figure 1-1H,
tion products within macrophages in- inset). While these cells may be
dicates a late active lesion. Inactive erroneously interpreted as a sign of
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 903
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
KEY POINT
h Active multiple sclerosis malignancy, their evenly spaced pat- (Figure 1-1A–C) associated with im-
lesions show a tern together with the presence of munoglobulin and complement depo-
profound pathologic macrophages should rule out the sition on myelin, as well as phagocytosis
heterogeneity and diagnosis of astrocytic neoplasm. of complement-opsonized myelin de-
can be classified into Some MS neuropathologic studies bris by macrophages (Figure 1-1G), on
four immunopatterns, suggest that oligodendrocytes are pref- an inflammatory background (Figure
suggesting that the erentially destroyed in early lesions.13 1-1E–F). Pattern II lesions also exhibit
targets of injury and However, oligodendroglial injury is a variable loss of oligodendrocytes at the
mechanisms of variable, with numerous oligodendro- active border, with their reappearance
demyelination in cytes present in some lesions, often in the inactive plaque center and a
multiple sclerosis are
displaying signs of concurrent early high incidence of remyelinated shadow
different in different
remyelination.10 plaques. These findings suggest that
disease subgroups.
On the basis of specific myelin pro- demyelination and tissue injury in pat-
tein loss, plaque extent and topography, tern II MS lesions may be induced by
oligodendrocyte destruction, presence antibody-mediated and complement-
or absence of remyelination, immuno- mediated mechanisms. Elevated immu-
globulin deposition, and complement noglobulins and activated complement
activation, early active white matter MS are present in the CSF of MS patients,
lesions show a profound pathologic and serum and CSF from MS patients
heterogeneity, and Lucchinetti and col- can cause demyelination in CNS or-
leagues have demonstrated that these ganotypic cultures in vitro. However,
lesions can be classified into four the specific target of these complement-
immunopatterns, suggesting that the activating antibodies has not yet been
targets of injury and mechanisms of identified.14 Myelin oligodendrocyte
demyelination in MS may differ between glycoprotein has been the prime candi-
patients.9 date target antigen because it is local-
Pattern I lesions, found in 15% of ized on the extracellular surface of the
MS patients who have been biopsied, myelin sheath and is accessible to
are sharply demarcated perivascular humoral immune reactions. However,
lesions characterized by active demy- autoantibodies that recognize myelin
elination with equal loss of all myelin oligodendrocyte glycoprotein in the
components, lack of immunoglobulin process of demyelination have been
deposition, and lack of complement detected only in a small subset of MS
activation on a T lymphocyte and patients, consisting of children with
activated macrophage/microglia in- atypical disease course.15 Moreover,
flammatory background. The destruc- by analogy with neuromyelitis optica
tion of myelin in pattern I MS may (NMO),16 it is possible that antibodies
therefore be mediated by toxic factors in MS patients may recognize other
produced by activated macrophages. nonmyelin targets,17 causing second-
Loss of oligodendrocytes is variable at ary demyelination.
the active lesional border, but numer- Pattern III lesions, found in 26% of
ous oligodendrocytes reappear in the biopsied MS patients, are ill-defined
inactive plaque center, and there is a lesions that show active demyelination
high incidence of remyelinated plaques. with oligodendrocyte apoptosis and
Pattern II lesions, found in about preferential loss of the periaxonal myelin
58% of MS biopsies, are sharply de- components (MAG and CNPase) on an
marcated lesions characterized by ac- inflammatory background (Figure 1-2).
tive demyelination (Figure 1-1D) with Loss of oligodendrocytes is pronounced
equal loss of all myelin components at the active plaque border and extends
904 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 1-2 Immunopattern III multiple sclerosis/Baló concentric sclerosis. Demyelination is characterized by A, a preferential
loss of the myelin protein myelin-associated glycoprotein (MAG) seen on MAG immunohistochemical (IHC)
staining (scale bar = 1.5 mm), while other myelin proteins such as B, proteolipid protein (PLP) (PLP IHC,
scale bar = 1.5 mm), and C, myelin oligodendrocyte glycoprotein (MOG) (MOG IHC, scale bar = 1.5 mm), are partially preserved.
into the apparently normal periplaque disturbance that renders them partic-
white matter. The inactive center is ularly vulnerable to the toxic action of
devoid of oligodendrocytes, and re- inflammatory mediators.
myelinated shadow plaques are ab- A small neuropathologic series by
sent. No evidence of immunoglobulin Barnett and Prineas of patients with MS
deposition and complement activation dying during or shortly after a relapse
has been reported. The early alter- challenged the concept of pathologic
ations affecting the most distal site heterogeneity.19 In these patients, the
from the oligodendrocyte cell body sug- earliest pathologic changes described
gest a dying-back oligodendrogliopathy. were prephagocytic lesions and con-
These changes have been observed in sisted of widespread oligodendrocyte
inflammatory demyelination induced apoptosis on a background of micro-
by viruses, damage of oligodendro- glial activation and myelin preservation.
cytes induced by toxicity (ie, cuprizone), Such regions had few lymphocytes and
and white matter injury caused by phagocytes. These changes were
acute ischemia and/or hypoxia; they followed by the disappearance of oligo-
may be driven by reactive oxygen dendrocytes and the formation of
and/or reactive nitrogen species, mi- intramyelinic edema. Finally, macro-
tochondrial dysfunction, or increased phages in the presence of inflammatory
expression of heme oxygenase 1, which T cells phagocytosed the fragmented
contributes to mitochondrial iron myelin. These macrophages were posi-
accumulation.9,18 tive for markers of complement. The
Pattern IV lesions, found in only 1% authors of this study interpreted this
of MS biopsies, are extremely rare and overlap of complement-containing
show a profound nonapoptotic death macrophages and oligodendrocyte ap-
of oligodendrocytes in the periplaque optosis within the same case as over-
white matter, suggesting a potential lap between MS patterns II and III,
primary metabolic oligodendrocyte suggesting that immunopathologic
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 905
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
KEY POINTS
h Axonal injury in multiple heterogeneity was dependent on the This damage is caused by the release of
sclerosis is most age of the lesions and not on the toxic inflammatory and nonspecific im-
pronounced during patient.19 However, recent neuropath- mune mediators in the lesion, such as
active inflammatory ologic findings have shown that patho- proteases, cytokines, excitotoxins, and
demyelination, and logic features resembling MS pattern II free radicals from the inflammatory
acute axonal injury and pattern III (ie, macrophages cells seen in close apposition to injured
occurring in early containing antibody or complement axons, which in turn causes mitochon-
multiple sclerosis lesions markers, and oligodendrocyte apopto- drial damage, increased oxidative stress,
likely contributes to sis with preferential loss of MAG, and energy deficiency.22,23
the relapse-related respectively) can be simultaneously
disability observed Chronic Plaques
found in a subset of active demyelinat-
predominantly during
ing NMO supraspinal lesions. These Chronic plaques are more frequently
the inflammatory
disease phases.
features strongly resemble the character- seen than active plaques in patients
istics of the stage-dependent heterogene- with progressive MS. Chronic active
h Inflammation is ity that Barnett and Prineas described in plaques are sharply demarcated
invariably present in
the prephagocytic/active demyelinating demyelinated lesions where numerous
all lesion types and
disease stages of
lesions and raise the possibility that the myelin-laden macrophages are concen-
multiple sclerosis, but its index case described by Barnett and trated at the centrifugally expanding
severity decreases with Prineas was NMO rather than MS.20 This edges of the plaque and diminish
patient age and disease is further supported by the aggressive toward its hypocellular inactive center,
duration. clinical course in their pediatric patient while smoldering plaques may contrib-
with relapse-related disability, includ- ute to progression1,8,24 and are charac-
ing an episode of myelitis as well as terized by a slowly expanding rim of
severe brainstem dysfunction, leading activated microglia (few of which con-
to death within 1 year of onset.19 tain myelin degradation products) sur-
Demyelination with relative axonal rounding their inactive center. Chronic
sparing (Figure 1-1I) is important for inactive plaques are completely demyelin-
the diagnosis of demyelinating lesions, ated, sharply circumscribed hypocellular
whereas an infarct is more likely if axons lesions characterized by substantial loss of
and myelin in lesions are depleted to the axons and oligodendrocytes, astrogliosis,
same extent.1,2,7 Despite relative axonal and minor infiltration by macrophages/
sparing, axonal injury does occur, microglia and lymphocytes.1,2
evidenced by the presence of axonal Inflammation is invariably present
swellings (irregularly swollen axons with in almost all lesion types and disease
a beaded appearance), accumulation of stages of MS. However, its severity
amyloid-" precursor protein (a marker decreases with the age of patients and
of focal accumulations of proteins that disease duration, and it may even
are typically moved along axons by fast decline to levels seen in age-matched
axonal transport), and mild axonal controls, but only in chronic inactive
loss.21 Axonal injury is most pro- lesions of aged patients at the very late
nounced during active inflammatory stage of the disease.11 Perivascular
demyelination. Acute axonal injury oc- inflammatory infiltrates are often en-
curring in early MS lesions likely con- countered in chronic lesions, but the
tributes to relapse-related disability BBB remains intact or its damage is
observed predominantly during the in- too limited to be visible by gadolinium
flammatory disease phases.1,8 The ex- enhancement on MRI.11 Lymphoid
tent of axonal damage in active lesions follicular structures are formed in
correlates significantly with the number large perivascular spaces, and plasma
of lymphocytes and activated microglia. cells accumulate in later disease stage
906 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
and persist within the CNS even when Remyelinated Plaques
h The neurodegeneration
T-cell and B-cell inflammation is Remyelinated plaques are characterized in all demyelinated
cleared.11 This dissociation between by the presence of thinly myelinated lesions is invariably
inflammation and BBB disturbance axons with short internodal distances. associated with
may be explained by inflammation in Extensive remyelination, indicated by the inflammation, and in
chronic progressive MS becoming presence of newly formed myelin sheaths chronic inactive lesions
trapped within the CNS behind a and oligodendrocyte precursor cells, is from aged patients
closed or repaired BBB. frequently encountered within active with long-standing
As the plaque progresses from acute plaques of early MS and may represent progressive multiple
active to chronic inactive, its edema an early phase of remyelination.1,2,10 sclerosis where the
inflammatory process
resolves, inflammation decreases, and Remyelinated lesions are present within
has died out, the
macrophages and microglia gradually active immunopattern I and II MS plaques:
neurodegeneration is
disappear. Astrocytes produce glial fi- oligodendrocytes are lost in the ex- also reduced to levels
bers, and ultimately a glial scar fills the panding actively demyelinating regions, seen in control patients.
demyelinated plaque (astrocytic fibrillary but oligodendrocyte precursor cells
h Extensive remyelination,
gliosis). These characteristics prompted are recruited and reappear in the in-
illustrated by the
Charcot to name the disease ‘‘sclerose active plaque center. Immunopattern presence of newly
en plaque’’ and are also responsible for III and IV MS lesions show massive formed myelin sheaths
the distinctly demarcated, firm, re- loss of oligodendrocytes, typically and oligodendrocyte
tracted, and brownish discoloration without signs of oligodendrocyte pre- precursor cells, is
of the long-standing chronic MS plaques cursor cell recruitment and remyelina- frequently encountered
on gross pathology. tion. The presence and extent of within active plaques of
Axonal damage and loss are also remyelination therefore depends in early multiple sclerosis.
apparent in chronic MS, where axonal part on the availability of oligoden-
density is reduced up to 80% within drocyte precursor cells and the pro-
the plaque.11,12 Neurodegeneration in or anti-inflammatory balance and
all demyelinated lesions is invariably varies among patients, possibly be-
associated with inflammation, and in cause of pathologic heterogeneity of
chronic inactive lesions from aged pa- oligodendrocyte damage.9
tients with long-standing progressive MS Complete remyelinated lesions, so-
where the inflammatory process has called shadow plaques, are sharply
died out, the neurodegeneration is also demarcated areas with reduced myelin
reduced to levels seen in non-MS control density and disproportionately thin my-
patients.11 Several mechanisms have elin sheaths, and reflect a late phase of
been proposed to account for chronic remyelination. Older remyelinated
axonal damage and neurodegeneration plaques show an almost normal thick-
in MS: (1) repeated demyelination within ness of myelin and are therefore diffi-
previously remyelinated lesions; (2) axo- cult to distinguish from normal white
nal degeneration due to the lack of matter. Shadow plaques are extensive
trophic support from myelin and oligo- in progressive MS cases as well as in
dendrocytes; (3) chronic mitochondrial patients with relapsing MS, as evidence
failure in the setting of increased energy for remyelination is seen in almost half
demands; (4) oxidative burst by activated of chronic MS lesions,27 and in some
microglia; (5) alterations in the expres- patients with MS almost all plaques are
sion or activity of axonal ion channels; shadow plaques.28 However, remyelin-
(6) oxidative stress caused by mito- ated plaques are more susceptible to a
chondrial dysfunction, inflammation, second-hit inflammatory demyelinat-
or dysregulation of iron homeostasis; ing attack than the normal-appearing
and (7) Wallerian degeneration.22,25,26 white matter.29 The mechanisms of
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 907
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
KEY POINTS
h Cortical demyelinated remyelination may progressively fail in sparing of the superficial cortical
lesions are present and patients with MS, and the failure to layers. Conventional MRI techniques
common in early remyelinate axons may be due to an are relatively insensitive in detecting
multiple sclerosis, are age-dependent loss of trophic support intracortical and subpial lesions. While
highly inflammatory, from microglia, oligodendrocyte pre- recent imaging protocols using double
and may represent the cursor cell exhaustion by repeated inversion recovery and high-field MRI
pathologic substrate of demyelinating insults, inappropriate in- have substantially improved their in
cognitive impairment teractions between axons and oligo- vivo detection, most cortical lesions
and epilepsy in dendrocytes, or the dense glial scar are still not visualized by any MRI
relapsing-remitting that may function as a barrier pre- technique.4,6,8,32 Patients with early
multiple sclerosis.
venting the migration of oligodendro- cortical involvement may have a worse
h The presence of cyte precursor cells into lesions. prognosis, and the accumulation of
inflammatory cortical cortical involvement is also linked with
demyelination in early NEUROPATHOLOGY OF disease progression and disability. Be-
multiple sclerosis argues CORTICAL LESIONS cause extensive cortical involvement
against a primary
The cortex in MS may be involved may be associated with more rapid
neurodegenerative
process at this stage of
either as neuronal loss and atrophy or progression, there is a pressing need
disease and suggests as classical cortical demyelinated le- to develop imaging techniques able to
that neuronal and sions. The former is the result of the reliably capture this pathology, both
axonal injury in early anterograde or retrograde degenera- to better understand the disease path-
cortical demyelination tion from lesions located in the white ogenesis and to determine the poten-
occur on a background matter, deep gray nuclei, or other tial impact of disease-modifying
of inflammation. areas of the cortex.30,31 However, therapies on the cortex.
classical cortical demyelination occurs
spatially and is anatomically indepen- Cortical Demyelinated Lesions
dent of white matter or deep gray in Early Multiple Sclerosis
pathology.12 Although the existence of Cortical demyelinated lesions in early
cortical lesions has been acknowl- MS are common and may represent
edged for a long time, their study has the pathologic substrate of cognitive
been largely disregarded because of impairment and epilepsy in relapsing-
their poor visualization when using remitting MS. Minimal cortical pathol-
classical myelin histochemical staining ogy has been associated with a benign
methods.5 Immunohistochemistry for MS course, and the cortical lesion load
myelin proteins is superior to Luxol correlates positively with clinical dis-
fast blue for detecting cortical demye- ability, white matter T2 lesion load,
linating lesions.5 Three cortical lesion and brain atrophy.3,4,33
types have been described based on The majority of all cortical lesion types
their location within the cortex: in early MS show evidence of active
subpial lesions extend from the pial demyelination as illustrated by the
surface to cortical layer three or four, presence of myelin-laden macrophages
or to the entire width of the cortex, (Figure 1-3A, B).34,35 Perivascular and
and may involve several gyri; intra- parenchymal inflammatory infiltrates
cortical lesions are small, perivascular are invariably present in early cortical
demyelinated lesions confined within lesions and are composed mainly of
the cortex with the sparing of both macrophages, T cells, and fewer B cells
superficial cortex and adjacent white and plasma cells (Figure 1-3C, D).34,35
matter; leukocortical lesions involve Breakdown of BBB is also present
both gray and white matter at the gray (Figure 1-4A).34,35 Inflammatory cells
matterYwhite matter junction with can be observed in close apposition to
908 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 1-3 Pathology of multiple sclerosis cortical onset. A, Subpial cortical lesion visualized as the absence of proteolipid
protein (PLP) immunohistochemical (IHC) staining; arrows indicate the border between the cortical lesion and
the normally myelinated gray matter and white matter (PLP IHC, scale bar = 500 2m). B, Active demyelination
(black arrows indicate myelin-laden macrophages) in the cortical lesion (white arrow indicates a neuron) (PLP IHC, scale bar =
50 2m). C, Macrophage infiltration (IHC for cluster of differentiation [CD] 68, a macrophage marker, scale bar = 100 2m).
D, Perivascular and parenchymal infiltration with T cells visible as CD3-positive brown-stained cells (CD3 IHC, scale bar = 100 2m).
E, Axonal injury evidenced by the presence of axonal swellings (arrows) in a lesional area with relative axonal preservation (IHC for
neurofilament protein, scale bar = 50 2m). F, Injured neurons (black arrows) scattered among normal-appearing neurons (white
arrows) (hematoxylin and eosin, scale bar = 50 2m). G, Macrophages/microglia (brown-stained cells) present in the upper cortex
and meninges (CD68 IHC, scale bar = 100 2m). H, Meningeal inflammation with T lymphocytes (brown-stained cells) (CD3 IHC,
scale bar = 50 2m). I, Most T cells are cytotoxic T cells as evidenced by their brown CD8 immunohistoreactivity (IHC for CD8,
a marker of cytotoxic lymphocytes, scale bar = 50 2m).
neurons and neurites in early cortical Some patients with MS may present
lesions34,35; the observed oligoden- with cortical lesions as their earliest
drocyte, axonal, and neuronal injury pathologic event. Therefore, inflam-
may be the result of the acute inflam- matory demyelinating disease should
matory damage (Figure 1-3E, F). be considered in the differential diag-
Thus, histopathologic evidence of in- nosis of patients presenting on MRI
flammatory cortical demyelination in with a solitary cortical enhancing le-
early MS suggests that neuronal and sion.35,36 Case 1-1 is an example of
axonal injury in early cortical demye- inflammatory cortical-onset MS.35
lination typically occurs on a back- Pathologic studies have established
ground of inflammation. that meningeal inflammation is prominent
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 909
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
FIGURE 1-4 MRI of multiple sclerosis cortical onset. A, Prebiopsy axial T1-weighted image with contrast showing
enhancement of the cortical lesion (arrow). Inset shows that contrast enhancement is within the cortical gray
matter (arrowheads indicate the gray/white matter junction). B, Axial T2-weighted image 69 months after
biopsy showing the appearance of new periventricular white matter lesions. C, Sagittal fluid-attenuated inversion recovery
(FLAIR) image 69 months after biopsy showing the appearance of multiple new white matter lesions, with two of the lesions
involving the corpus callosum.
KEY POINTS in early MS (Figure 1-3G–I).34 Both inflammation and demyelination of the
h Meningeal inflammation focal perivascular meningeal inflam- deeper subcortical white matter.34
is present in early mation and diffuse meningeal in-
multiple sclerosis and flammation are topographically and Cortical Demyelinated Lesions
topographically in Chronic Multiple Sclerosis
strongly associated with cortical le-
associated with cortical
sions in early MS.34 The presence of Cortical demyelinated lesions in
lesions; it may drive the
cortical demyelination
diffuse meningeal inflammation in- chronic MS may be the pathologic
but also set the stage creases the odds of cortical demyelin- substrate of irreversible disability, pro-
for subsequent ation 45-fold, whereas perivascular gression, and cognitive deficits, 39
subcortical white meningeal inflammation increases the since they are prominent and exten-
matter inflammation odds of cortical demyelination 15-fold.34 sive in patients with progressive MS
and demyelination. Experimental autoimmune encephalo- and cognitive impairment. In progres-
h Profound meningeal myelitis models have emphasized the sive MS, extensive cortical demyelin-
inflammatory infiltrates importance of pathogenic T-lymphocyte ation has been detected in the frontal,
are composed of trafficking into the CSF in the subarach- temporal, insular, and cerebellar corti-
T cells, B cells, and noid space, where they are restimulated ces in addition to the cingulate gyrus
macrophages; by meningeal antigen-presenting cells, and hippocampus.39
topographically undergo clonal expansion, and produce Pathologically, in chronic progres-
associate with subpial cytokines.37 These events promote a sive MS, cortical lesions lack breakdown
lesions; and may second wave of T-cell infiltration across of the BBB, inflammatory infiltrates, and
drive the cortical
pia vessels and an upregulation of vas- complement deposition.5 Most phago-
demyelination and
cular adhesion molecules in the deeper cytes in cortical lesions are microglia
neurodegeneration in
patients with both
brain vasculature, followed by parenchy- located in close apposition to neurons
primary and secondary mal invasion and disease onset.38 These and neurites,5 with atrophy and apo-
progressive multiple observations support the hypothesis ptosis of neurons; oligodendrocytes
sclerosis. that production and release of inflam- are also damaged.5,40
matory cytokines in the subarachnoid Profound meningeal inflammatory
space in early MS may drive cortical infiltrates have been described and
demyelination and promote subsequent extensively characterized in late-stage
910 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Case 1-1
A 33-year-old white woman presented with sudden-onset headache
associated with right periorbital pain. Her medical history was notable only
for a history of migraine, a vaginal delivery 4 months ago, and an upper
respiratory tract infection 1 week ago. The neurologic examination was
normal. Brain MRI revealed a high signal intensity lesion on T2-weighted
imaging involving the left occipital cortex (visual association cortex) that
enhanced with gadolinium (Figure 1-4A). No other cortical or white matter
lesions were noted.
An open brain biopsy performed 1 month after symptom onset
to exclude neoplasm revealed a subpial cortical demyelinated lesion
(Figure 1-3A) heavily infiltrated by phagocytic macrophages involved in
active demyelination (Figure 1-3B). Parenchymal and perivascular cortical
inflammatory infiltrates were present and composed of macrophages,
microglia, CD3-positive and CD8-positive T cells, B lymphocytes, and
plasma cells (Figure 1-3C, D). Acute axonal injury was evidenced by axonal
swellings (Figure 1-3E), and neuronal injury was evidenced by the presence
of scattered pyknotic neurons (Figure 1-3F). Macrophages, microglia,
and T lymphocytes were found in close apposition to neurons as well
as concentrated subpially in the cortical molecular layer and in the
subarachnoid space (Figure 1-3G). Mild meningeal inflammation consisting
of CD3-positive T lymphocytes, CD8-positive T and B lymphocytes, and
plasma cells was present (Figure 1-3H, I).
Because of the patient’s persistent headaches, a CSF analysis was done
4 months after biopsy and demonstrated an elevated CSF IgG synthesis
rate with normal protein, glucose, and cell count and one oligoclonal
band. Lyme serology was negative. Six months after biopsy, the patient
complained of increasing left-sided chest numbness, and spine MRI
showed two subtle T2-weighted lesions at C4-5 and C6 levels. Eleven
months after biopsy, she developed burning dysesthesias in the lower
extremities. Brain MRI revealed new periventricular T2-weighted white
matter lesions. She fulfilled diagnostic criteria for multiple sclerosis (MS)
with a relapsing-remitting disease course. At the time of last follow-up
(69 months after biopsy), brain MRI demonstrated an interval increase
in the number of white matter lesions typical of MS (Figure 1-4B, C),
and she was started on glatiramer acetate after referral to the
authors’ clinic.
Comment. The first lesion detected in this case was a cortical lesion
with pathologic features typical for acute inflammatory demyelinating
lesions of MS.35 Subpial demyelinated lesions, as demonstrated in this
case, may occur early in MS.34 Gadolinium enhancement of the newly
forming cortical lesion is an uncommon observation; however, it was
observed in this case, which highlights that acute cortical lesion formation
is characterized by similar, albeit more transient MRI features compared
to white matter lesions in MS. Possible reasons for the paucity of this
phenomenon include the lack of symptoms associated with lesion
formation in small focal subpial cortical areas (therefore no MRI is
acquired during this stage), limited blood-brain barrier breakdown, and
more rapid resolution of inflammation in the cortex compared to the
white matter.
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 911
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
KEY POINTS
h Baló concentric sclerosis progressive MS. They are composed of are found at the periphery of pattern
is now believed to be a T cells, B cells, and macrophages; are III MS lesions. Active Baló lesions are
variant of pattern III topographically associated with subpial associated with preferential loss of
multiple sclerosis. lesions; and are found in patients with MAG9,45 and oligodendrocyte apopto-
h Clinical, neuroimaging, both primary and secondary progressive sis, suggesting that the oligodendro-
and neuropathologic MS.41Y43 The extent of meningeal in- cyte apoptosis in the demyelinated
criteriaVas well as flammation correlates with microglia rings is the main pathogenetic in-
serologic and CSF activation and the extent of demyelin- sult.45,46 Baló concentric sclerosis is
markers that distinguish ation and neurodegeneration in the now believed to be a variant of
neuromyelitis optica underlying cortex. Patients with exten- pattern III MS, although other mech-
from multiple sive meningeal inflammation show a anisms of demyelination have been
sclerosisVare available. more severe clinical course, shorter hypothesized.1,2
disease duration, and younger age at
death. Meningeal inflammatory infil- Neuromyelitis Optica
trates resembling ectopic B-cell follicu- NMO is an autoimmune astrocytopathy
lar structures have been described in that causes secondary demyelination
secondary progressive MS. They are (Figure 1-5B–D). The water channel
located in the deep sulci of the tempo- aquaporin-4 (AQP4), expressed on
ral, cingulate, insular, and frontal corti- astrocytes and highly concentrated in
ces of secondary progressive MS the astrocytic foot processes that abut
patients with accelerated clinical course capillaries and pia in the CNS, has
and topographically associated with been identified as the target antigen in
subpial lesions. 43 Such lymphoid NMO. AQP4 exists as two different hete-
follicle-like structures have not been rotetramers (M-1 and M-23 AQP4), that
identified in primary progressive MS.42 further assemble in various ratios into
Therefore, meningeal inflammatory ag- higher ordered structures named or-
gregates may drive cortical injury, and thogonal array of particles. Clinical,
soluble factors produced by meningeal serologic, CSF, neuroimaging, and neu-
activated lymphocytes may diffuse into ropathologic criteria that distinguish
the cortical tissue, causing demyelin- NMO from MS are now available.16,47Y52
ation and neurodegeneration either Case 1-2 is an example of NMO. The
directly or indirectly through microglia neuropathologic characteristic of all
activation. NMO lesions, irrespective of the stage
of demyelinating activity, is the striking
NEUROPATHOLOGY OF loss of AQP4 that extends beyond the
OTHER INFLAMMATORY demyelinated area (Figure 1-5E, J).
DEMYELINATING DISEASES This characteristic is unlike MS, in
Baló Concentric Sclerosis which AQP4 loss is stage dependent:
Baló concentric sclerosis is an MS MS active lesions show increased AQP4
variant with large concentric lesions expression on astrocytes within the
characterized by circumferential rings lesions (Figure 1-5L), while AQP4 is
of myelin loss alternating with rings of lost in MS lesions that are no longer
myelin preservation (Figure 1-2).1,2,44 active.50 Other important neuropatho-
Due to this spectacular concentric logic features of NMO lesions include a
arrangement, Baló MS lesions can be vasculocentric pattern of immunoglob-
occasionally recognized on MRI and ulin deposition and complement acti-
even on fresh pathologic specimens. vation in active NMO lesions; decrease
Concentric Baló-like alternating rims or complete loss of glial fibrillary acidic
of demyelinated and myelinated tissue protein (GFAP) immunoreactivity in
912 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 1-5 Pathology of a neuromyelitis optica (NMO) lesion located in the ventral medulla. A, Destructive
hypercellular lesion; arrows indicate the border between the lesion that shows atypical hematoxylin
and eosin (HE) staining (area below arrows) and normal-appearing white matter with preserved HE
staining (area above arrows) (HE, scale bar = 500 2m). B, Demyelinated lesion; arrows indicate the border between
lesion that shows loss of proteolipid protein (PLP) immunohistoreactivity (area below arrows) and normal-appearing
white matter with preserved PLP immunohistoreactivity (area above arrows) (PLP immunohistochemical [IHC]
staining, scale bar = 500 2m). C, Active demyelination (arrows indicate myelin-laden macrophages) (PLP, scale
bar = 50 2m). D, The lesion shows macrophage infiltration (KiM1P IHC, scale bar = 250 2m). E, Loss of aquaporin-4
(AQP4) is characteristic for active NMO lesions; arrows indicate the border between lesion that shows loss of AQP4
immunohistoreactivity (area below arrows) and increased AQP4 immunohistoreactivity seen at the lesion’s edge
(area above arrows) (AQP4 IHC, scale bar = 250 2m). F, Loss of glial fibrillary acidic protein (GFAP) is also frequently
encountered in NMO-active demyelinating lesions; arrows indicate the border between the lesion that shows loss of
GFAP immunohistoreactivity (area below arrows) and normal GFAP immunohistoreactivity of the normal-appearing
white matter surrounding the lesion (area above arrows) (GFAP IHC, scale bar = 500 2m). G, Loss of aquaporin
in the area postrema (arrow) (AQP4 IHC, scale bar = 250 2m). H, Macrophage/microglia infiltration in the area
postrema (KiM1P IHC, scale bar = 100 2m). I, Area postrema blood vessels (asterisks) with thickened and hyalinized
walls (HE; scale bar = 50 2m). J, Active NMO lesions with loss of AQP4 immunoreactivity seen as the disappearance
of the perivascular rim or rosette AQP4 pattern (asterisks) and loss of AQP4 outlining of the astrocytic surface
(arrows) (AQP4 IHC; scale bar = 50 2m). K, Increased AQP4 immunoreactivity outlining the cytoplasmic surface
of reactive astrocytes (arrows) with preservation of the typical perivascular distribution (asterisks) at the border of
the NMO lesion (AQP4 IHC; scale bar = 50 2m). L, Increased AQP4 immunoreactivity outlining the cytoplasmic
surface of reactive astrocytes (arrows) with preservation of the typical perivascular distribution (asterisks) within an
active multiple sclerosis lesion (AQP4 IHC; scale bar = 50 2m).
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 913
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
Case 1-2
A 39-year-old woman of African, Hispanic, and Asian ancestry developed epigastric pain and right
foot numbness, followed by similar symptoms in the left foot a week later. Over the following 2
weeks she developed lower extremity upper motor neuron weakness and frequent tonic flexor
spasms. She spontaneously improved from this event.
Her second relapse 4 months later included left-sided weakness, diplopia, and spasticity. She
had a left Babinski sign and bilateral lower extremity hyperreflexia with loss of pinprick sensation up
to the right hip and left knee. She also experienced constipation and recurrent tonic flexor spasms.
Carbamazepine and 5 days of IV methylprednisolone were administered without improvement.
MRIs showed a longitudinally
extensive T2 lesion in the cervical
cord and medulla and no
hemispheric abnormalities.
CSF examination revealed
10 nucleated cells per 2L.
Her third relapseVless than a
month after the secondVincluded
left upper extremity pain and
dystonic movements in the
context of high fever, as well
as urinary incontinence, leading
to urinary retention and
quadriplegia. Repeat brain MRI
showed periventricular and
corpus callosum lesions,
along with brainstem lesions
(Figure 1-6A, B). Spinal cord MRI
showed lesions throughout the
cervical and thoracic cord. The
patient failed to respond to
repeat IV methylprednisolone
treatment. Worsening quadriplegia
and diplopia with new-onset
dysphagia was documented
2 years after her initial presentation
in the context of urosepsis.
Neuromyelitis optica (NMO)YIgG
screening was positive. MRI
revealed brain and spinal cord
atrophy with gadolinium
enhancement in the medulla
(Figure 1-6C, D).
FIGURE 1-6 MRI of neuromyelitis optica. A, Sagittal, and B, axial
Six months later she experienced fluid-attenuated inversion recovery (FLAIR) images
demonstrating heterogeneous T2-hyperintense corpus
progressive worsening of all callosum and periventricular lesions with poorly defined margins.
neurologic symptoms, new-onset C, 2 months later, and, D, 17 months later, sagittal T2-weighted images of
intractable hiccupping, and an the cervical spinal cord and posterior fossa. Note the longitudinally extensive
central T2-hyperintense lesion of the spinal cord on both images (arrows).
active urinary tract infection. Spinal cord atrophy is appreciated as a more narrow appearance of the cord
Within the following year she in panel D.
required a feeding tube. She had
Continued on page 915
914 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Continued from page 914
recurrent nausea and vomiting episodes. Progressively worsening dyspnea resulted in her death
1 month later.
Autopsy revealed the presence of hypercellular demyelinating lesions (Figure 1-5A, B) infiltrated
by macrophages/microglia involved in active demyelination (Figure 1-5C, D), as well as lymphocytes
and plasma cells. Lesional blood vessels had thickened and hyalinized walls (Figure 1-5I). These
active lesions exhibited aquaporin-4 (AQP4) and glial fibrillary acidic protein (GFAP) loss consistent
neuropathologically with NMO (Figure 1-5E, F, J). Inflammatory, nondestructive nondemyelinating
lesions with loss of AQP4 were noted in the area postrema (Figure 1-5G–I).
Comment. The pathologic diagnosis is strongly consistent with NMO in this case, highlighting
several key features of the disease, including the presence of nondemyelinated as well as destructive
demyelinating lesions, associated with AQP4 and GFAP loss.48Y50,53 The original spinal cord MRI
with a longitudinally extensive T2-hyperintense lesion and a ‘‘swollen cord’’ appearance is typical
for NMO.52 Intractable hiccups, nausea, and vomiting are common features of NMO, likely related
to area postrema involvement.53Y55 While a progressive course as demonstrated in this case is
uncommon in NMO, and frequent severe attacks are more typical, the presence of a progressive stage
does not exclude this diagnosis.52 NMO-IgG is a highly specific biomarker of NMO; however, in up
to 30% of cases this serum test may be negative.16,47 Respiratory involvement leading to death is
more common in fulminant NMO cases compared to MS.
This patient had not been treated at the authors’ institution, and her treatment predated current
discoveries related to NMO. Aggressive treatment of acute relapses and robust maintenance
therapies are now available and should be utilized in severe NMO cases.
parallel to the loss of AQP4 (Figure 1-5F) maturational differences in the ratio of
in destructive NMO lesions; the pres- the two AQP4 isoforms (M1 and M23) in
ence of perivascular and parenchymal the astrocytic membranes. A subset of
inflammatory infiltrates that contain active demyelinating supraspinal NMO
eosinophils and neutrophils in demye- brain lesions simultaneously show path-
linated and nondemyelinated areas; ologic features resembling MS pattern II
axonal loss, necrosis, and cavitation (antibody or complement deposition in
in destructive regions (Figure 1-5A); macrophages) and pattern III (prefer-
blood vessels with thickened and ential MAG loss and apoptosis of oligo-
hyalinized walls (Figure 1-5I); and dendrocytes).20 Misclassification of
intramyelinic edema.48,50,56 The affini- these cases as MS rather than NMO
ty of NMO-IgG binding to AQP4 is may erroneously support the concept of
influenced by the ratio M1:M23.53,57,58 intraindividual heterogeneity in MS.20
Furthermore, the binding of NMO-IgG Inflammatory but nondestructive
to AQP4 has isoform-specific out- and nondemyelinating lesions have
comes: M1 is completely internalized, also been described in NMO. These
whereas M23 resists internalization and lesions have been observed in the
is aggregated into larger-order orthog- area postrema, which lacks a BBB, sug-
onal arrays of particles that activate gesting that this and other circum-
complement more effectively than M1 ventricular organs could be sites of
when bound by NMO-IgG.56 Therefore, initial NMO-IgG access to the CNS
differences in the nature and anatomical (Figure 1-5G–I). Area postrema lesions
distribution of NMO lesions and in the in NMO are believed to be the patho-
clinical and imaging manifestations of logic substrate for the intractable but
NMO may be influenced by regional and reversible nausea and vomiting that
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 915
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
Case 1-3
A 24-year-old white woman with a 1-year history of IV drug abuse
developed intermittent headache with occasional blurry vision. One
month later she experienced right fronto-occipital headache with right
eye blurred vision and right arm and left leg paresthesias in the context of
an upper respiratory infection with right ear pain, sore throat, cough,
fever, and chills. Three days later she noted severe photophobia with
worsening neurologic symptoms, leading to hospitalization. Examination
was notable for Kernig sign, right Babinski sign, meningismus, right visual
field cut, an unsteady gait, and a left pupillary dilation. Brain CT was
normal. Lumbar puncture revealed a protein level of 86 mg/dL, glucose
level of 54 mg/dL, and 37 nucleated cells per 2L, with 97% lymphocytes.
Bacterial, viral, and fungal CSF cultures were negative, as were HIV,
monospot, Venereal Disease Research Laboratory (VDRL), and purified
protein derivative (PPD) tests. Ophthalmologic evaluation, cerebral
angiogram, and nerve conduction studies were unrevealing. EEG showed
diffuse generalized slowing. Serology studies revealed IgM seropositivity
for Legionella and Mycoplasma.
Over the course of 3 days, the patient became quadriparetic with
multiple brainstem/cranial nerve signs and worsening mental status,
eventually becoming completely unresponsive and requiring mechanical
ventilation. MRI showed extensive signal abnormalities in the brainstem
and medulla. The patient remained comatose and continued to decline
despite high-dose IV methylprednisolone treatment and supportive care
in the intensive care unit. She died after support was withdrawn.
Autopsy revealed the presence of ‘‘sleeves’’ of demyelination
surrounding small, engorged venules (Figure 1-7A, B), associated
with significant inflammatory infiltrates dominated by macrophages,
T and B lymphocytes, and granulocytes (Figure 1-7C, D). Findings were
consistent with the neuropathologic diagnosis of acute disseminated
encephalomyelitis (ADEM). Multifocal cortical microglial aggregates, not
associated with cortical demyelination, were scattered throughout the
cortex (Figure 1-7E, F).
Comment. A monophasic course over several weeks with signs and
symptoms of systemic infections are characteristic for fulminant ADEM, as
highlighted in this case.2,65 Headache, meningismus, and encephalopathy
are uncommon in multiple sclerosis (MS) but may accompany ADEM, and
overall a polysymptomatic onset is also more typical of ADEM.2,65 While
ADEM is more common among pediatric populations, adult cases do
occur.2,65 When tissue is available, ADEM can be diagnosed
neuropathologically; its most typical features include perivenular sheets
of demyelination with variable inflammatory infiltrates consisting of
macrophages, lymphocytes, and granulocytes.2,7,64 This is in contrast
with MS, where confluent demyelination with sheets of macrophage
infiltration admixed with reactive astrocytes are more typical. In
addition, a distinct pattern of cortical microglial activation and
aggregation without demyelination may be observed in ADEM,
especially in cases with depressed levels of consciousness.63
Continued on page 917
916 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Continued from page 916
FIGURE 1-7 Pathology of acute disseminated encephalomyelitis. A, Sleeves of perivascular demyelination
(Luxol fast blue/periodic acidYSchiff staining) seen as the disappearance of the normal blue
staining of the myelin conferred by the Luxol fast blue (several blood vessels with perivascular
demyelination are marked with asterisks) (scale bar = 500 2m). B, Sleeves of perivascular demyelination (asterisks
mark several blood vessels with perivascular loss of proteolipid protein [PLP]) (PLP, scale bar = 500 2m).
C, Infiltration with macrophages (KiM1P, scale bar = 500 2m). D, Perivascular inflammatory infiltrate with
neutrophils (arrows) (hematoxylin and eosin, scale bar = 50 2m); E, Cortical microglial aggregate (arrows) (KiM1P,
scale bar = 100 2m). F, The cortex in the region of the microglial aggregate does not show cortical demyelination
(PLP, scale bar = 500 2m).
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 917
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
KEY POINT
h In acute disseminated sometimes precede episodes of optic cytic meningitis is frequent in ADEM.63
encephalomyelitis, neuritis and transverse myelitis; they Cortical microglial aggregates that are
multifocal cortical may even represent the initial heralding not associated with cortical demye-
microglial aggregates NMO symptom.53,54 linated lesions may be found dispersed
not associated with While the normal human cortex is throughout the cortex (Figure 1-7E, F).63
cortical demyelination rich in AQP4, in NMO, the cortical This patternVof multifocal cortical mic-
are scattered distribution of AQP4 is preserved with roglial aggregates scattered throughout
throughout the cortex no pathologic or MRI evidence of the cortex, not associated with cortical
or are concentrated cortical demyelinated lesions. 59Y61 demyelinationVis unique to ADEM and
adjacent to neurons in The absence of cortical demyelination, may reflect the pathologic substrate of
the external pyramidal
which is another neuropathologic fea- the depressed level of consciousness
layer and may represent
ture distinguishing NMO from MS, seen in this disorder.63
the pathologic
substrate of the
may explain the typical absence of a
secondary progressive clinical course Acute Hemorrhagic
depressed level of
consciousness in these in NMO.59,62 Regional differences in Leukoencephalitis
patients. the permeability of the BBB or differ- Acute hemorrhagic leukoencephalitis,
ential expression of the two AQP4 or Hurst disease, is considered a
isoforms may be responsible for the hyperacute variant of ADEM. It consists
absence of cortical lesions in NMO. histologically of hemorrhagic demye-
linating lesions around blood vessels
Acute Disseminated that are small and often necrotic, with
Encephalomyelitis prominent edema and axonal injury.64
Acute disseminated encephalomyelitis Mononuclear cells and neutrophils
(ADEM) lesions are often bilateral, comprise perivascular and meningeal
affecting the cerebral white matter, inflammatory infiltrates. The presence
brainstem, cerebellum, and spinal cord. of perivascular hemorrhage and the
ADEM may also involve the peripheral extent of microvascular damage serve
ganglia and roots of the spinal and to distinguish acute hemorrhagic
cranial nerves. Case 1-3 is an example leukoencephalitis from ADEM lesions.
of ADEM. Pathologically, ADEM con-
sists of ‘‘sleeves’’ of demyelination CONCLUSIONS
centered on small, engorged venules. Recent neuropathologic studies have
Significant inflammatory infiltrates are provided new fundamental insights
present and consist of myelin-laden into the pathogenesis of MS and have
macrophages, variable T and B lympho- helped to distinguish MS from other
cytes, and occasional plasma cells and inflammatory demyelinating diseases.
granulocytes (Figure 1-7A–D).2,7,63,64 MS is heterogeneous, and each immu-
Despite relative axonal preservation, ax- nopattern needs surrogate MRI, clinical,
onal injury may be present. Many genetic, serologic, or CSF markers to be
perivenous demyelinating lesions may developed that would allow their differ-
coalescence to form larger areas of de- entiation in the nonbiopsied MS popu-
myelination, but the MS-characteristic lation, and a specifically tailored
joint areas of demyelination, macrophage therapeutic strategy to each. Cortical
infiltration, and reactive astrocytes are lesions are common in early MS, where
not typically seen in ADEM, although they may even represent the earliest
transitional cases have been described. pathologic event in some MS patients
Cortical pathology evidenced by the and are inflammatory and topographi-
presence of subpial and intracortical cally associated with meningeal inflam-
demyelinated lesions with mild lympho- mation. These new observations set the
918 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
stage for a new ‘‘outside-in’’ view of MS findings in multiple sclerosis. Lancet Neurol
2012;11(4):349Y360.
pathogenesis: the extension of the
inflammatory process from the menin- 9. Lucchinetti C, Bruck W, Parisi J, et al.
Heterogeneity of multiple sclerosis lesions:
ges and the subarachnoid space, where implications for the pathogenesis of
the CNS immune surveillance takes demyelination. Ann Neurol 2000;47(6):
place, to the cortex, and then further 707Y717.
to the deep white matter with subse- 10. Bruck W, Porada P, Poser S, et al. Monocyte/
quent demyelination and neuro- macrophage differentiation in early
multiple sclerosis lesions. Ann Neurol 1995;
degeneration. These new concepts 38(5):788Y796.
may help identify novel inflammatory 11. Frischer JM, Bramow S, Dal-Bianco A, et al.
targets for the treatment of MS. The relation between inflammation and
neurodegeneration in multiple sclerosis
ACKNOWLEDGMENTS brains. Brain 2009;132(pt 5):1175Y1189.
The authors have been supported by 12. Kutzelnigg A, Lucchinetti CF, Stadelmann C,
et al. Cortical demyelination and diffuse
grants from the Saskatchewan Health white matter injury in multiple sclerosis.
Research Foundation (2633, to Dr Brain 2005;128(pt 11):2705Y2712.
Popescu), the Canada Research Chairs 13. Prineas JW, McDonald WI. Demyelinating
program (to Dr Popescu), the National diseases. In: Graham DI, Lantos PL,
Multiple Sclerosis Society (NMSS editors. Greenfield’s neuropathology,
6th ed. London, England: Arnold, 1997:
RG3185-B-3, to Dr Lucchinetti), and 813Y896.
the NIH (NIH 1R01NS058698, to Dr Pirko;
14. Burgoon MP, Gilden DH, Owens GP. B cells
and NIH 1R01NS049577, to Dr Lucchinetti). in multiple sclerosis. Front Biosci 2004;9:
786Y796.
REFERENCES 15. Brilot F, Dale RC, Selter RC, et al. Antibodies
to native myelin oligodendrocyte glycoprotein
1. Popescu BF, Lucchinetti CF. Pathology of
in children with inflammatory demyelinating
demyelinating diseases. Ann Rev Pathol
central nervous system disease. Ann Neurol
2012;7:185Y217.
2009;66(6):833Y842.
2. Sobel RA, Moore GRW. Demyelinating
16. Lennon VA, Kryzer TJ, Pittock SJ, et al. IgG
diseases. In: Love S, Louis DN, Ellison DW,
marker of optic-spinal multiple sclerosis
editors. Greenfield’s neuropathology, 8th
binds to the aquaporin-4 water channel.
ed. London, England: Oxford University
J Exp Med 2005;202(4):473Y477.
Press, 2008:1513Y1608.
17. Srivastava R, Aslam M, Kalluri SR, et al.
3. Calabrese M, Filippi M, Gallo P. Cortical
Potassium channel KIR4.1 as an immune
lesions in multiple sclerosis. Nat Rev Neurol
target in multiple sclerosis. N Engl J Med
2010;6(8):438Y444.
2012;367(2):115Y123.
4. Geurts JJ, Barkhof F. Grey matter pathology
18. Aboul-Enein F, Lassmann H. Mitochondrial
in multiple sclerosis. Lancet Neurol 2008;
damage and histotoxic hypoxia: a pathway
7(9):841Y851.
of tissue injury in inflammatory brain
5. Peterson JW, Bo L, Mork S, et al. Transected disease? Acta Neuropathol 2005;109(1):
neurites, apoptotic neurons, and reduced 49Y55.
inflammation in cortical multiple sclerosis
19. Barnett MH, Prineas JW. Relapsing and
lesions. Ann Neurol 2001;50(3):389Y400.
remitting multiple sclerosis: pathology of
6. Pirko I, Lucchinetti CF, Sriram S, Bakshi R. the newly forming lesion. Ann Neurol
Gray matter involvement in multiple 2004;55(4):458Y468.
sclerosis. Neurology 2007;68(9):634Y642.
20. Bruck W, Popescu B, Lucchinetti CF, et al.
7. Kuhlmann T, Lassmann H, Bruck W. Neuromyelitis optica lesions may inform
Diagnosis of inflammatory demyelination multiple sclerosis heterogeneity debate.
in biopsy specimens: a practical approach. Ann Neurol 2012;72(3):385Y394.
Acta Neuropathol 2008;115(3):275Y287.
21. Bjartmar C, Wujek JR, Trapp BD. Axonal
8. Filippi M, Rocca MA, Barkhof F, et al. loss in the pathology of MS: consequences
Association between pathological and MRI for understanding the progressive phase of
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 919
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Pathology of Multiple Sclerosis
the disease. J Neurol Sci 2003;206(2): 36. Calabrese M, Gallo P. Magnetic resonance
165Y171. evidence of cortical onset of multiple
sclerosis. Mult Scler 2009;15(8):933Y941.
22. Dutta R, Trapp BD. Mechanisms of
neuronal dysfunction and degeneration in 37. Reboldi A, Coisne C, Baumjohann D,
multiple sclerosis. Prog Neurobiol 2011; et al. C-C chemokine receptor 6-regulated
93(1):1Y12. entry of TH-17 cells into the CNS through
the choroid plexus is required for the
23. Fischer MT, Sharma R, Lim JL, et al. NADPH
initiation of EAE. Nat Immunol 2009;10(5):
oxidase expression in active multiple
514Y523.
sclerosis lesions in relation to oxidative
tissue damage and mitochondrial injury. 38. Bartholomaus I, Kawakami N, Odoardi F,
Brain 2012;135(pt 3):886Y899. et al. Effector T cell interactions with
meningeal vascular structures in nascent
24. Prineas JW, Kwon EE, Cho ES, et al.
autoimmune CNS lesions. Nature
Immunopathology of secondary-progressive
2009;462(7269):94Y98.
multiple sclerosis. Ann Neurol 2001;50(5):
646Y657. 39. Kutzelnigg A, Lassmann H. Cortical
demyelination in multiple sclerosis: a
25. Coleman M. Axon degeneration
substrate for cognitive deficits? J Neurol Sci
mechanisms: commonality amid diversity.
2006;245(1Y2):123Y126.
Nat Rev Neurosci 2005;6(11):889Y898.
40. Wegner C, Esiri MM, Chance SA, et al.
26. Raff MC, Whitmore AV, Finn JT. Axonal
Neocortical neuronal, synaptic, and glial loss
self-destruction and neurodegeneration.
in multiple sclerosis. Neurology 2006;67(6):
Science 2002;296(5569):868Y871.
960Y967.
27. Barkhof F, Bruck W, De Groot CJ, et al.
41. Magliozzi R, Howell O, Vora A, et al.
Remyelinated lesions in multiple sclerosis:
Meningeal B-cell follicles in secondary
magnetic resonance image appearance.
progressive multiple sclerosis associate with
Arch Neurol 2003;60(8):1073Y1081.
early onset of disease and severe cortical
28. Patrikios P, Stadelmann C, Kutzelnigg A, pathology. Brain 2007;130(pt 4):1089Y1104.
et al. Remyelination is extensive in a subset
42. Choi SR, Howell OW, Carassiti D, et al.
of multiple sclerosis patients. Brain 2006;
Meningeal inflammation plays a role in
129(pt 12):3165Y3172.
the pathology of primary progressive
29. Bramow S, Frischer JM, Lassmann H, et al. multiple sclerosis. Brain 2012;135(pt 10):
Demyelination versus remyelination in 2925Y2937.
progressive multiple sclerosis. Brain
43. Howell OW, Reeves CA, Nicholas R, et al.
2010;133(10):2983Y2998.
Meningeal inflammation is widespread and
30. Cifelli A, Arridge M, Jezzard P, et al. linked to cortical pathology in multiple
Thalamic neurodegeneration in multiple sclerosis. Brain 2011;134(pt 9):2755Y2771.
sclerosis. Ann Neurol 2002;52(5):650Y653.
44. Moore GR, Neumann PE, Suzuki K, et al.
31. Kolasinski J, Stagg CJ, Chance SA, et al. A Balo’s concentric sclerosis: new observations
combined post-mortem magnetic resonance on lesion development. Ann Neurol
imaging and quantitative histological study 1985;17(6):604Y611.
of multiple sclerosis pathology. Brain
45. Stadelmann C, Ludwin S, Tabira T, et al.
2012;135(pt 10):2938Y2951.
Tissue preconditioning may explain
32. Seewann A, Kooi EJ, Roosendaal SD, et al. concentric lesions in Balo’s type of multiple
Postmortem verification of MS cortical lesion sclerosis. Brain 2005;128(pt 5):979Y987.
detection with 3D DIR. Neurology 2012;
46. Yao DL, Webster HD, Hudson LD, et al.
78(5):302Y308.
Concentric sclerosis (Balo): morphometric
33. Popescu BF, Lucchinetti CF. Meningeal and and in situ hybridization study of lesions
cortical grey matter pathology in multiple in six patients. Ann Neurol 1994;35(1):18Y30.
sclerosis. BMC Neurol 2012;12:11.
47. Lennon VA, Wingerchuk DM, Kryzer TJ,
34. Lucchinetti CF, Popescu BFG, Bunyan RF, et al. A serum autoantibody marker of
et al. Inflammatory cortical demyelination neuromyelitis optica: distinction from
in early multiple sclerosis. N Engl J Med multiple sclerosis. Lancet 2004;364(9451):
2011;365(23):2188Y2197. 2106Y2112.
35. Popescu BF, Bunyan RF, Parisi JE, et al. 48. Lucchinetti CF, Mandler RN, McGavern D,
A case of multiple sclerosis presenting et al. A role for humoral mechanisms in the
with inflammatory cortical demyelination. pathogenesis of Devic’s neuromyelitis
Neurology 2011;76(20):1705Y1710. optica. Brain 2002;125(pt 7):1450Y1461.
920 www.ContinuumJournal.com August 2013
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
49. Misu T, Fujihara K, Kakita A, et al. Loss of 58. Crane JM, Lam C, Rossi A, et al. Binding
aquaporin 4 in lesions of neuromyelitis affinity and specificity of neuromyelitis
optica: distinction from multiple sclerosis. optica autoantibodies to aquaporin-4
Brain 2007;130(pt 5):1224Y1234. M1/M23 isoforms and orthogonal
arrays. J Biol Chem 2011;286(18):
50. Roemer SF, Parisi JE, Lennon VA, et al.
16516Y16524.
Pattern-specific loss of aquaporin-4
immunoreactivity distinguishes 59. Popescu BF, Parisi JE, Cabrera-Gomez JA,
neuromyelitis optica from multiple et al. Absence of cortical demyelination
sclerosis. Brain 2007;130(pt 5):1194Y1205. in neuromyelitis optica. Neurology 2010;
75(23):2103Y2109.
51. Takano R, Misu T, Takahashi T, et al.
Astrocytic damage is far more severe 60. Sinnecker T, Dorr J, Pfueller CF, et al.
than demyelination in NMO: a clinical CSF Distinct lesion morphology at 7-T MRI
biomarker study. Neurology 2010;75(3): differentiates neuromyelitis optica from
200Y201. multiple sclerosis. Neurology 2012;79(7):
708Y714.
52. Wingerchuk DM, Lennon VA, Pittock SJ, et al.
Revised diagnostic criteria for neuromyelitis 61. Calabrese M, Oh MS, Favaretto A, et al.
optica. Neurology 2006;66(10):1485Y1489. No MRI evidence of cortical lesions in
53. Popescu BF, Lennon VA, Parisi JE, et al. neuromyelitis optica. Neurology 2012;
Neuromyelitis optica unique area postrema 79(16):1671Y1676.
lesions: nausea, vomiting and pathogenic 62. Wingerchuk DM, Pittock SJ, Lucchinetti CF,
implications. Neurology 2011;76(14):1229Y1237. et al. A secondary progressive clinical
54. Apiwattanakul M, Popescu BF, Matiello M, course is uncommon in neuromyelitis
et al. Intractable vomiting as the initial optica. Neurology 2007;68(8):603Y605.
presentation of neuromyelitis optica. Ann 63. Young NP, Weinshenker BG, Parisi JE,
Neurol 2010;68(5):757Y761. et al. Perivenous demyelination:
55. Rodriguez M, Scheithauer B. Ultrastructure association with clinically defined acute
of multiple sclerosis. Ultrastruct Pathol disseminated encephalomyelitis and
1994;18(1Y2):3Y13. comparison with pathologically confirmed
multiple sclerosis. Brain 2010;133(pt 2):
56. Hinson SR, Romero MF, Popescu BF, et al. 333Y348.
Molecular outcomes of neuromyelitis
optica (NMO)-IgG binding to aquaporin-4 in 64. Hart MN, Earle KM. Haemorrhagic and
astrocytes. Proc Natl Acad Sci U S A 2012; perivenous encephalitis: a clinical-pathological
109(4):1245Y1250. review of 38 cases. J Neurol Neurosurg
Psychiatry 1975;38(6):585Y591.
57. Fenton RA, Moeller HB, Zelenina M, et al.
Differential water permeability and 65. Wingerchuk DM. The clinical course of
regulation of three aquaporin 4 isoforms. acute disseminated encephalomyelitis.
Cell Mol Life Sci 2010;67(5):829Y840. Neurol Res 2006;28(3):341Y347.
Continuum (Minneap Minn) 2013;19(4):901–921 www.ContinuumJournal.com 921
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
You might also like
- 1.psychiatric Neuroscience - Incorporating Pathophysiology Into Clinical Case Formulation - ClinicalKeyDocument43 pages1.psychiatric Neuroscience - Incorporating Pathophysiology Into Clinical Case Formulation - ClinicalKeyClaudia0% (1)
- Wilson - Cranial NervesDocument243 pagesWilson - Cranial NervesBiblioteca CSNT100% (13)
- Midterm NEUROLOGYDocument122 pagesMidterm NEUROLOGYAhmad SobihNo ratings yet
- Jarvis Neurological Assessment SummaryDocument11 pagesJarvis Neurological Assessment Summaryaderonke bello100% (2)
- Afifi, Adel K. - Bergman, Ronald Arly - Functional Neuroanatomy Text and Atlas-McGraw Hill Professional (2011)Document506 pagesAfifi, Adel K. - Bergman, Ronald Arly - Functional Neuroanatomy Text and Atlas-McGraw Hill Professional (2011)Junior MichaelNo ratings yet
- Sinelnikov Vol IIIDocument395 pagesSinelnikov Vol IIIOana Musteaţǎ100% (12)
- Multiple Sclerosis Progression Time For A New Mechanism-Driven FrameworkDocument11 pagesMultiple Sclerosis Progression Time For A New Mechanism-Driven FrameworkasasakopNo ratings yet
- Effect of Photobiomodulation in MultiplesclerosisDocument4 pagesEffect of Photobiomodulation in MultiplesclerosisMuhammad Imam NoorNo ratings yet
- Optical Coherence Tomography A Window Into The Mechanisms of Multiple SclerosisDocument12 pagesOptical Coherence Tomography A Window Into The Mechanisms of Multiple SclerosisSara BkrNo ratings yet
- Pathology of Multiple Sclerosis: CNS & Neurological Disorders Drug Targets May 2012Document13 pagesPathology of Multiple Sclerosis: CNS & Neurological Disorders Drug Targets May 2012jhidalgomdNo ratings yet
- Frohman 2006Document11 pagesFrohman 2006Alfredo Enrique Marin AliagaNo ratings yet
- Research Paper Outline On Multiple SclerosisDocument5 pagesResearch Paper Outline On Multiple Sclerosisfznn7hzd100% (1)
- Therapeutic Approaches in BruxismDocument9 pagesTherapeutic Approaches in BruxismIlinca LupuNo ratings yet
- Conversion of Optic Neuritis To Relapsing Remitting Multiple Sclerosis: A Retrospective Comorbidity Cohort StudyDocument6 pagesConversion of Optic Neuritis To Relapsing Remitting Multiple Sclerosis: A Retrospective Comorbidity Cohort StudymesrurekoseogluNo ratings yet
- 668 FullDocument10 pages668 FullfranciscoNo ratings yet
- 15 Höglinger Et Al 2024 RosiDocument14 pages15 Höglinger Et Al 2024 RosiROSIANE RONCHI NASCIMENTONo ratings yet
- Fmed 10 1200427Document3 pagesFmed 10 1200427SOFIA POBLETE CACERESNo ratings yet
- tmp4D8B TMPDocument2 pagestmp4D8B TMPFrontiersNo ratings yet
- Pocd 2Document21 pagesPocd 2fulgentius juliNo ratings yet
- Enfermedad MitocondrialDocument12 pagesEnfermedad MitocondrialOsvaldo CortésNo ratings yet
- Journal Reading - Progressive Multiple SclerosisDocument20 pagesJournal Reading - Progressive Multiple SclerosisMuhammad Imam NoorNo ratings yet
- Neuromodulation TechniquesDocument23 pagesNeuromodulation TechniquesAlexandra BuenoNo ratings yet
- Craddock 2014 World PsychiatryDocument2 pagesCraddock 2014 World PsychiatryPrateekGandhiNo ratings yet
- Differential Diagnosis of Suspected Multiple Sclerosis - An Updated Consensus ApproachDocument15 pagesDifferential Diagnosis of Suspected Multiple Sclerosis - An Updated Consensus ApproachInthe MOON youNo ratings yet
- SeminarDocument20 pagesSeminarricardojosesotofontalvoNo ratings yet
- Mol Med Clin PsychDocument9 pagesMol Med Clin PsychalondraNo ratings yet
- The Spectrum of Neuromyelitis Optica: ReviewDocument11 pagesThe Spectrum of Neuromyelitis Optica: ReviewRiccardo TroiaNo ratings yet
- Classification, Diagnosis, and Differential Diagnosis of Multiple SclerosisDocument13 pagesClassification, Diagnosis, and Differential Diagnosis of Multiple Sclerosisrasha elkapanyNo ratings yet
- Reich DS - MSDocument17 pagesReich DS - MSinesNo ratings yet
- Terminología y Clasificación de Las Displasias (2004) PDFDocument7 pagesTerminología y Clasificación de Las Displasias (2004) PDFlucasher35No ratings yet
- Brainsci 12 00885Document14 pagesBrainsci 12 00885José Ernesto AlonsoNo ratings yet
- Part C - Multiple SclerosisDocument4 pagesPart C - Multiple SclerosisStaph AureusNo ratings yet
- Preprints202304 0108 v1Document25 pagesPreprints202304 0108 v1Henrique OliveiraNo ratings yet
- Diagnostico, Pronostico y Tratamiento de Las Leucodistrofias.Document11 pagesDiagnostico, Pronostico y Tratamiento de Las Leucodistrofias.carmenNo ratings yet
- Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesFrom EverandNeuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesAmanda L. PiquetNo ratings yet
- Biosensing Technologies For Neuroinflammatory Disease.1Document13 pagesBiosensing Technologies For Neuroinflammatory Disease.1MARIA DE FATIMA TEIXEIRA GORDILLONo ratings yet
- Proforma For Registration of Subject For Dissertation: TH RDDocument10 pagesProforma For Registration of Subject For Dissertation: TH RDHariNo ratings yet
- Revisión de Instrumentos 2016Document13 pagesRevisión de Instrumentos 2016juanpaNo ratings yet
- Multiple Sclerosis Lancet 2018Document15 pagesMultiple Sclerosis Lancet 2018Sarah Miryam CoffanoNo ratings yet
- Neurobiological Principles in The Etiopathogenesis of Disease When Diseases Have A HeadDocument11 pagesNeurobiological Principles in The Etiopathogenesis of Disease When Diseases Have A HeadSaurabh Gayali100% (2)
- Profile of and Risk Factors For Poststroke CognitiveDocument16 pagesProfile of and Risk Factors For Poststroke CognitiveFera EyFeraNo ratings yet
- 14 MsDocument18 pages14 MsMendila FerryNo ratings yet
- Diagnosis of Multiple Sclerosis - 2017 Revisions of McDonald PDFDocument13 pagesDiagnosis of Multiple Sclerosis - 2017 Revisions of McDonald PDFricky rdnNo ratings yet
- Terminology and Classification of The Cortical Dysplasias PalminiDocument9 pagesTerminology and Classification of The Cortical Dysplasias PalminiAyhan BölükNo ratings yet
- Pediatric DemyelinationDocument19 pagesPediatric DemyelinationPERLITA NEGRANo ratings yet
- JURNALDocument10 pagesJURNALLuses Shantia HaryantoNo ratings yet
- DX y TtoDocument13 pagesDX y TtoIvi HidalgoNo ratings yet
- Journal Neurologi 2Document10 pagesJournal Neurologi 2fatya azaraNo ratings yet
- 人工智能在神经病理学中的应用:基于深度学习的tau蛋白病变评估Document23 pages人工智能在神经病理学中的应用:基于深度学习的tau蛋白病变评估meiwanlanjunNo ratings yet
- The Spectrum of Neuromyelitis Optica: ReviewDocument11 pagesThe Spectrum of Neuromyelitis Optica: ReviewMonica Aleja FernándezNo ratings yet
- How Certain Are You When Making The Diagnosis of Multiple System Atrophy?Document2 pagesHow Certain Are You When Making The Diagnosis of Multiple System Atrophy?Carlos Hernan Castañeda RuizNo ratings yet
- Revisions Defining The Clinical Course of Multiple Sclerosis: The 2013Document11 pagesRevisions Defining The Clinical Course of Multiple Sclerosis: The 2013Fernando Dueñas MoralesNo ratings yet
- Jamapsychiatry Mccutcheon 2019 SchizophreniaDocument10 pagesJamapsychiatry Mccutcheon 2019 Schizophreniavaleria.correa1No ratings yet
- Different Subtypes of DyskineticDocument8 pagesDifferent Subtypes of DyskineticMariana CarneiroNo ratings yet
- Blue Light and The EyeDocument16 pagesBlue Light and The EyeHussein Abo aliNo ratings yet
- Brain SciencesDocument20 pagesBrain SciencesCarolina MuñozNo ratings yet
- Brainsci 11 00301 v3Document20 pagesBrainsci 11 00301 v3Carolina MuñozNo ratings yet
- Diagnosis of Multiple Sclerosis Progress and ChallengesDocument11 pagesDiagnosis of Multiple Sclerosis Progress and Challengessarawu9911No ratings yet
- Kuhle Et Al 2019 Neurofilament Light Levels Are Associated With Long Term Outcomes in Multiple SclerosisDocument9 pagesKuhle Et Al 2019 Neurofilament Light Levels Are Associated With Long Term Outcomes in Multiple SclerosisAlin CiubotaruNo ratings yet
- Shirazi Et Al 2015 - Vitamin D and AstrocytesDocument15 pagesShirazi Et Al 2015 - Vitamin D and Astrocytesdr. RiyanNo ratings yet
- Nihms 899459Document35 pagesNihms 899459Gerson RamírezNo ratings yet
- Diagnostico Valoracion Neuropsicologica en DemenciaDocument19 pagesDiagnostico Valoracion Neuropsicologica en Demenciajhoel cruzNo ratings yet
- Revisao Sistematica de Diagnostico Do Tea 2015Document15 pagesRevisao Sistematica de Diagnostico Do Tea 2015Anuska ErikaNo ratings yet
- Role of Microglia in MSDocument7 pagesRole of Microglia in MSpreedtooneNo ratings yet
- Clinical Neuroimmunology: Multiple Sclerosis and Related DisordersFrom EverandClinical Neuroimmunology: Multiple Sclerosis and Related DisordersNo ratings yet
- @million Medical Books Island ofDocument290 pages@million Medical Books Island ofHj AbuNo ratings yet
- Write The Name of The Cranial Nerve of Your Answer On The Blank Provided Before The NumberDocument2 pagesWrite The Name of The Cranial Nerve of Your Answer On The Blank Provided Before The NumberSHARMAINE ANNE POLICIOSNo ratings yet
- Nervous SystemDocument79 pagesNervous SystemAffan ElahiNo ratings yet
- K8a Anatomi Sistem Saraf PusatDocument87 pagesK8a Anatomi Sistem Saraf Pusathartinissa vaniaNo ratings yet
- The Human Nervous System: Second EditionDocument13 pagesThe Human Nervous System: Second EditionThiruvenkata ManiNo ratings yet
- Nervous SystemDocument109 pagesNervous SystemHirpâsà MămoNo ratings yet
- Food Deprivation: A Neuroscientific Perspective: Harald T. Schupp and Britta RennerDocument19 pagesFood Deprivation: A Neuroscientific Perspective: Harald T. Schupp and Britta RennerJohnny AtmanNo ratings yet
- Human-Anatomy-Kenneth-S-Saladin-2008 (1) - Halaman-424-450 PDFDocument27 pagesHuman-Anatomy-Kenneth-S-Saladin-2008 (1) - Halaman-424-450 PDFBelva EdinaNo ratings yet
- Pain and Central Perceptual Mechanisms: Iris Edith Casillas MartinezDocument22 pagesPain and Central Perceptual Mechanisms: Iris Edith Casillas MartinezDaniela SodeNo ratings yet
- Emailing 31-05-2023-05-38-46 - All - EncounterMedantaReport1685534924331Document3 pagesEmailing 31-05-2023-05-38-46 - All - EncounterMedantaReport1685534924331driftekharalam24No ratings yet
- Ch.3 Quiz BDocument22 pagesCh.3 Quiz BSultan AlghamdiNo ratings yet
- Lecture 1: NeuroembryologyDocument13 pagesLecture 1: NeuroembryologyRaul Docto100% (1)
- Endoscopic Telovelar Approach To The Fourth Ventricle - Anatomic StudyDocument9 pagesEndoscopic Telovelar Approach To The Fourth Ventricle - Anatomic StudyfrancsicovillegaslopezNo ratings yet
- Gate Control Theory of PainDocument3 pagesGate Control Theory of Paincarmo-netoNo ratings yet
- An Algorithm For The Evaluation of Peripheral Neuropathy - American Family PhysicianDocument9 pagesAn Algorithm For The Evaluation of Peripheral Neuropathy - American Family PhysicianAnonymous vnv6QFNo ratings yet
- The CerebrumDocument27 pagesThe Cerebrumapi-19916399No ratings yet
- Internal Capsule and Horizontal Slices of ForebrainDocument5 pagesInternal Capsule and Horizontal Slices of ForebrainDenis QosjaNo ratings yet
- Bahan BrainDocument7 pagesBahan BrainArwina Syazwani Binti GhazaliNo ratings yet
- 7.reflex Regulation of Physiological Function PDFDocument2 pages7.reflex Regulation of Physiological Function PDFNektarios TsakalosNo ratings yet
- Corticospinal Tract Practice QuestionsDocument2 pagesCorticospinal Tract Practice QuestionsAlexaNo ratings yet
- Cutaneous Silent Periods - Part 2 - Update On Pathophysiology and Clinical UtilityDocument12 pagesCutaneous Silent Periods - Part 2 - Update On Pathophysiology and Clinical UtilityGogy MarkNo ratings yet
- Nervous System Module 1 PDFDocument10 pagesNervous System Module 1 PDFMrittika MitraNo ratings yet
- Biological Basis of BehaviorDocument17 pagesBiological Basis of BehaviorAasma IsmailNo ratings yet
- Pupil Evaluation: Walter Huang, OD Yuanpei University Department of OptometryDocument54 pagesPupil Evaluation: Walter Huang, OD Yuanpei University Department of OptometryRatri Wulandari SusilaningrumNo ratings yet
- Autonomic Nervous Syste and Neurohumoral Transmission-Dr - Jibachha Sah, M.V.SC, LecturerDocument32 pagesAutonomic Nervous Syste and Neurohumoral Transmission-Dr - Jibachha Sah, M.V.SC, Lecturerjibachha sahNo ratings yet