You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- (GYNE) 2018 April Midterms Ratio (Pucca)Document31 pages(GYNE) 2018 April Midterms Ratio (Pucca)NoreenNo ratings yet
- Clinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzDocument31 pagesClinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzNoreenNo ratings yet
- (Gyne) Family Planning (Dra Ona - Dra Castro) Updated Version (2022)Document14 pages(Gyne) Family Planning (Dra Ona - Dra Castro) Updated Version (2022)NoreenNo ratings yet
- (Anes) 3 - Monitoring of Anesthetized Patient (Dra. Mendoza) ?Document4 pages(Anes) 3 - Monitoring of Anesthetized Patient (Dra. Mendoza) ?NoreenNo ratings yet
- (Cardio B) 1 - Acute Rheumatic Fever and Rheumatic Heart Disease (Dr. Antolin, 2019)Document4 pages(Cardio B) 1 - Acute Rheumatic Fever and Rheumatic Heart Disease (Dr. Antolin, 2019)NoreenNo ratings yet
- (Anes) 1 - Preanesthetic Evaluation (Dra. Luna-Gomez) ?Document5 pages(Anes) 1 - Preanesthetic Evaluation (Dra. Luna-Gomez) ?NoreenNo ratings yet
- (Anes) 5 - Local Anesthetics (Dra. Bonoan-Chan) ?Document5 pages(Anes) 5 - Local Anesthetics (Dra. Bonoan-Chan) ?NoreenNo ratings yet
- (IM A) (Com Dse) Typhoid Fever (Strawberry)Document4 pages(IM A) (Com Dse) Typhoid Fever (Strawberry)NoreenNo ratings yet
- (IM A) (Com Dse) Typhoid Fever-Dr. Salandanan, Dr. Tan (Trisha Oberio, Kristine Navarro, Aisle Paler)Document4 pages(IM A) (Com Dse) Typhoid Fever-Dr. Salandanan, Dr. Tan (Trisha Oberio, Kristine Navarro, Aisle Paler)NoreenNo ratings yet
- Case 9 Section EDocument12 pagesCase 9 Section ENoreenNo ratings yet
- (IM A) (Hema) IDA and Hypoproliferative Anemias-Dr. Perez 2 (Kim Villanueva)Document5 pages(IM A) (Hema) IDA and Hypoproliferative Anemias-Dr. Perez 2 (Kim Villanueva)NoreenNo ratings yet
- (IM A) (Com Dse) Rabies-Dr. Coronel (Vision)Document7 pages(IM A) (Com Dse) Rabies-Dr. Coronel (Vision)Noreen100% (1)
- (MED) 3.05 Approach To Edema, Chest Pain, & Palpitations - AzaresDocument18 pages(MED) 3.05 Approach To Edema, Chest Pain, & Palpitations - AzaresNoreenNo ratings yet
- (Pedia 3A) Immunology-Dr. de Jesus (Pinky Square)Document6 pages(Pedia 3A) Immunology-Dr. de Jesus (Pinky Square)NoreenNo ratings yet
- Clinical Therapeutics: Case 1Document17 pagesClinical Therapeutics: Case 1NoreenNo ratings yet
- Cardiology: Normal and Abnormal Myocardial Function: LendldeornmanDocument2 pagesCardiology: Normal and Abnormal Myocardial Function: LendldeornmanNoreenNo ratings yet
- (Pedia 3A) NEPHRO COMPILED PDFDocument40 pages(Pedia 3A) NEPHRO COMPILED PDFNoreenNo ratings yet
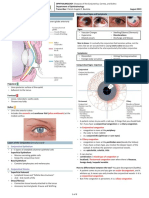
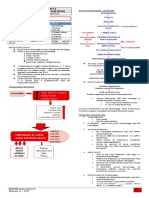
- (Ophtha) 7 - Diseases of The Conjunctiva, Cornea, and Sclera (2019)Document8 pages(Ophtha) 7 - Diseases of The Conjunctiva, Cornea, and Sclera (2019)NoreenNo ratings yet
- (MED1) 3.04 Approach To Hypertension (Dr. Bago-Azares)Document11 pages(MED1) 3.04 Approach To Hypertension (Dr. Bago-Azares)NoreenNo ratings yet
- Hypovolemic Shock & DIC (Bernabe)Document4 pagesHypovolemic Shock & DIC (Bernabe)NoreenNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Neuroanatómia Vizsgatételek A És B Csoport Képletekkel HZ ENDocument25 pagesNeuroanatómia Vizsgatételek A És B Csoport Képletekkel HZ ENTowan NguyenNo ratings yet
- Perdarahan Intra Dan Extra AxialDocument19 pagesPerdarahan Intra Dan Extra AxialFarmasi FKUNSNo ratings yet
- Gambaran CT SCAN: (Kasus: Edh, SDH, Ich, Sah, Infark Cerebri, IvhDocument44 pagesGambaran CT SCAN: (Kasus: Edh, SDH, Ich, Sah, Infark Cerebri, Ivhfahmi rosyadiNo ratings yet
- Necropsy Procedures and Basic Diagnostic Methods For Practicing VeterinariansDocument262 pagesNecropsy Procedures and Basic Diagnostic Methods For Practicing VeterinariansDenisa VescanNo ratings yet
- Imaging Anatomy Brain and Spine Anne G Osborn Full ChapterDocument67 pagesImaging Anatomy Brain and Spine Anne G Osborn Full Chaptervicki.wilson456100% (10)
- Introduction To NeuropsychologyDocument15 pagesIntroduction To NeuropsychologyPsychology Department Ilahia Arts CollegeNo ratings yet
- Nervous SystemDocument29 pagesNervous SystemMuhammed Aslam NVNo ratings yet
- 116 - Concept of Perception and CoordinationDocument3 pages116 - Concept of Perception and Coordinationalaisahmae02No ratings yet
- SPINAL CORD (External Features)Document39 pagesSPINAL CORD (External Features)Drravikumar BhandariNo ratings yet
- Imagerie Des TumeursDocument14 pagesImagerie Des TumeursOuma TaziNo ratings yet
- Ms - Angeline M.SC (N) Previous Year Psychiatric Nursing Choithram College of NursingDocument79 pagesMs - Angeline M.SC (N) Previous Year Psychiatric Nursing Choithram College of NursingPankaj TirkeyNo ratings yet
- Icd 9 CM (Tabulasi) 2012Document263 pagesIcd 9 CM (Tabulasi) 2012M Taufik Harahap100% (1)
- Epidural Space - Lies Between The Dura and The Vertebral BonesDocument4 pagesEpidural Space - Lies Between The Dura and The Vertebral BonesDaniel DanielNo ratings yet
- Robin Bhatia, Ian Sabin-Challenging Concepts in Neurosurgery - Cases With Expert Commentary-Oxford University Press (2015)Document253 pagesRobin Bhatia, Ian Sabin-Challenging Concepts in Neurosurgery - Cases With Expert Commentary-Oxford University Press (2015)rogeriotorres13100% (1)
- Gross Anatomy PDFDocument55 pagesGross Anatomy PDFDeborah RochaNo ratings yet
- 9th-10-11th May-2016 Papers (1650 MCQS) by Amlodipine Besylate PDFDocument161 pages9th-10-11th May-2016 Papers (1650 MCQS) by Amlodipine Besylate PDFAmlodipine BesylateNo ratings yet
- Lesson 3 Nervous SystemDocument11 pagesLesson 3 Nervous SystemMARY JANE ANGELICA SEVANo ratings yet
- The 12 Cranial NervesDocument11 pagesThe 12 Cranial Nervesapi-306342919No ratings yet
- Reconstruction of Skull Base Defects After Minimally Invasive Endoscopic Resection of Anterior Skull Base NeoplasmsDocument7 pagesReconstruction of Skull Base Defects After Minimally Invasive Endoscopic Resection of Anterior Skull Base NeoplasmsFemale calmNo ratings yet
- An Epidural Hemorrhage: Anatomy and Key ConceptsDocument14 pagesAn Epidural Hemorrhage: Anatomy and Key Concepts'Danang ヌグロホNo ratings yet
- Cervical Spine CYRIAXDocument16 pagesCervical Spine CYRIAXCarlos TavaresNo ratings yet
- ACNS Surgical Manual PDFDocument248 pagesACNS Surgical Manual PDFKevin EdroNo ratings yet
- Skullbase SurgeryDocument64 pagesSkullbase Surgeryzrated786100% (6)
- Chapter 3 Anatomical Organization of Cranial Nerves 2009 Manual Therapy For The Cranial NervesDocument4 pagesChapter 3 Anatomical Organization of Cranial Nerves 2009 Manual Therapy For The Cranial NervesDaniela Bustos PéndolaNo ratings yet
- Myelography in ChildrenDocument16 pagesMyelography in ChildrenFinna Tryasti Fidianti1BNo ratings yet
- EncehaDocument29 pagesEncehaToko RaMy Line100% (1)
- Ch. 12 & 13 Anaphy Reviewer (Long Quiz)Document12 pagesCh. 12 & 13 Anaphy Reviewer (Long Quiz)googlegirl18No ratings yet
- General Anatomy SyllabusDocument3 pagesGeneral Anatomy SyllabusPatricia patriciaNo ratings yet
- Nanda 2016Document15 pagesNanda 2016Novia AyuNo ratings yet
- Chapter 7 THE MENINGESDocument16 pagesChapter 7 THE MENINGESRoger Fernando Abril DiazNo ratings yet