You might also like
- Ijerph 19 09023 v2Document18 pagesIjerph 19 09023 v2princess Dela CruzNo ratings yet
- The Burden of Mental Illness, Alcohol Use Disorder, and Underage DrinkingFrom EverandThe Burden of Mental Illness, Alcohol Use Disorder, and Underage DrinkingNo ratings yet
- Faktor Risiko Kejadian Demensia Berdasarkan Studi LiteraturDocument5 pagesFaktor Risiko Kejadian Demensia Berdasarkan Studi LiteraturAisyah SyahidahNo ratings yet
- So Boka 2017Document7 pagesSo Boka 2017Kurnia pralisaNo ratings yet
- 3.the Relationship Between Different Dimensions of AlcoholDocument34 pages3.the Relationship Between Different Dimensions of AlcoholMariana Soto MontañoNo ratings yet
- INGLES Demencia Relacionada Con El Alcohol y Deterioro Neurocognitivo Un Estudio de RevisiónDocument9 pagesINGLES Demencia Relacionada Con El Alcohol y Deterioro Neurocognitivo Un Estudio de RevisiónandreaNo ratings yet
- Leshner, AI. (1998) - Addiction Is A Brain Disease, and It Matters.Document7 pagesLeshner, AI. (1998) - Addiction Is A Brain Disease, and It Matters.Sandy Cohen0% (1)
- An Assessment of The Demographic and Clinical CorrDocument11 pagesAn Assessment of The Demographic and Clinical CorrNataliaNo ratings yet
- RedditsDocument28 pagesRedditsBenjamin HeathNo ratings yet
- Mccambridge2011 PDFDocument14 pagesMccambridge2011 PDFDurga BalaNo ratings yet
- Yun Et Al (2022) The Impact of Heavy Alcohol ConsumptionDocument13 pagesYun Et Al (2022) The Impact of Heavy Alcohol ConsumptionRafael Camilo MayaNo ratings yet
- The Prevalence of Alcohol Use Disorders Among People Living With HIV/AIDS: A Systematic Review and Meta-AnalysisDocument9 pagesThe Prevalence of Alcohol Use Disorders Among People Living With HIV/AIDS: A Systematic Review and Meta-AnalysisClave T DanielsNo ratings yet
- Ahlin - Adults With Mild To Moderate DepressionDocument7 pagesAhlin - Adults With Mild To Moderate DepressionTriệu Văn NhậtNo ratings yet
- Effectiveness of Dynamic Homoeopathic Preparation of Dependent SubjectsDocument4 pagesEffectiveness of Dynamic Homoeopathic Preparation of Dependent SubjectsVarshaNo ratings yet
- Alcohol Use Disorder Severity and Reported Reasons Not To Seek Treatment: A Cross-Sectional Study in European Primary Care PracticesDocument10 pagesAlcohol Use Disorder Severity and Reported Reasons Not To Seek Treatment: A Cross-Sectional Study in European Primary Care PracticesPutri YingNo ratings yet
- Alcohol Related DisordersDocument27 pagesAlcohol Related DisordersAnonymous vnv6QFNo ratings yet
- Anxiety and Depressive Symptoms Associated To Alcohol Consumption in Health Care WorkersDocument17 pagesAnxiety and Depressive Symptoms Associated To Alcohol Consumption in Health Care WorkersTania MartinezNo ratings yet
- The Relationship Between Smoking and StrokeDocument8 pagesThe Relationship Between Smoking and StrokeaninditoNo ratings yet
- BMC Psychiatry: Five-Factor Model Personality Profiles of Drug UsersDocument10 pagesBMC Psychiatry: Five-Factor Model Personality Profiles of Drug UsersShana PokeerbuxNo ratings yet
- DINGAL Thesis c1-c5Document44 pagesDINGAL Thesis c1-c5Jonathan DingalNo ratings yet
- Epi DRG AbDocument13 pagesEpi DRG Abkbl27No ratings yet
- Comorbidity: Addiction and Other Mental IllnessesDocument12 pagesComorbidity: Addiction and Other Mental IllnessesnidaebooksNo ratings yet
- Change in Communities Resolving A Crisis 1Document21 pagesChange in Communities Resolving A Crisis 1api-410237738No ratings yet
- Concepts and Issues in COA Research: M W, P .DDocument7 pagesConcepts and Issues in COA Research: M W, P .DLakshit ManraoNo ratings yet
- Prevalence of Stroke in The Elderly A Systematic Review and Meta-AnalysisDocument10 pagesPrevalence of Stroke in The Elderly A Systematic Review and Meta-AnalysisMarian J. NietoNo ratings yet
- Influence of ADHD Especially Attention-Deficit ChaDocument13 pagesInfluence of ADHD Especially Attention-Deficit ChaDoina MafteiuNo ratings yet
- Peer Preessure Study of Alcohol Drinking in Tbe UkDocument13 pagesPeer Preessure Study of Alcohol Drinking in Tbe Uk2307702No ratings yet
- Politicas de Reducción de Consumo AlcoholDocument15 pagesPoliticas de Reducción de Consumo AlcoholLuisa FernandaNo ratings yet
- Nature 2011 Global Mental HealthDocument4 pagesNature 2011 Global Mental HealthcogidaNo ratings yet
- 2016 - IJBAMR - Other Psychiatric Comorbidities in Male Patients of Alcohol Dependence PDFDocument11 pages2016 - IJBAMR - Other Psychiatric Comorbidities in Male Patients of Alcohol Dependence PDFSantosh KumarNo ratings yet
- Acupuncture For Behavioral and Psychological.22Document6 pagesAcupuncture For Behavioral and Psychological.22Wendi ChinchayanNo ratings yet
- SPP 03 1 13Document10 pagesSPP 03 1 13Zenith xNo ratings yet
- Artículo Evidencia de Recaídas (Hardelveld)Document8 pagesArtículo Evidencia de Recaídas (Hardelveld)María CastilloNo ratings yet
- Medication Adherence Influencing Factors - An (Updated) Overview of Systematic ReviewsDocument17 pagesMedication Adherence Influencing Factors - An (Updated) Overview of Systematic ReviewsDewi AryantiNo ratings yet
- Alcohol Use Disorders 2016 LancetDocument11 pagesAlcohol Use Disorders 2016 Lancet簡凱倫No ratings yet
- Alcohol Related Problems Literature ReviewDocument7 pagesAlcohol Related Problems Literature Reviewafmzetkeybbaxa100% (1)
- 10 1155@2013@546342Document8 pages10 1155@2013@546342Tony StarkNo ratings yet
- Alcohol y CerebroDocument19 pagesAlcohol y CerebromdsgdNo ratings yet
- Studiu PsihoDocument42 pagesStudiu PsihoCarmenAlinaNo ratings yet
- A Risk-Benefit Assessment of Dementia Medications Systematic Review of The Evidence.Document15 pagesA Risk-Benefit Assessment of Dementia Medications Systematic Review of The Evidence.astrogliaNo ratings yet
- Cuantificación Del Consumo de Alcohol en AlemaniaDocument9 pagesCuantificación Del Consumo de Alcohol en AlemaniaJosé Luis Villadiego SilvaNo ratings yet
- Drug and Alcohol Abuse: A Clinical Guide to Diagnosis and TreatmentFrom EverandDrug and Alcohol Abuse: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Pharmacological Interventions For Challenging Behaviour in Children With Intellectual Disabilities: A Systematic Review and Meta-AnalysisDocument13 pagesPharmacological Interventions For Challenging Behaviour in Children With Intellectual Disabilities: A Systematic Review and Meta-AnalysisCristinaNo ratings yet
- Psychiatric Comorbidity in Alcohol Dependence: A Cross-Sectional Study in A Tertiary Care SettingDocument5 pagesPsychiatric Comorbidity in Alcohol Dependence: A Cross-Sectional Study in A Tertiary Care Settinggion.nandNo ratings yet
- s12888 019 2077 8Document9 pagess12888 019 2077 8baynaNo ratings yet
- The Sociopsychological Profile of Persons With Alcohol Anosognosia in The Context of Social Customer SupportDocument5 pagesThe Sociopsychological Profile of Persons With Alcohol Anosognosia in The Context of Social Customer SupportS. M.No ratings yet
- Big Data Application: Study and Archival of Mental Health Data, Using MongodbDocument5 pagesBig Data Application: Study and Archival of Mental Health Data, Using MongodbNay Chi Than HtunNo ratings yet
- Prevencion de Ulceras DiabeticasDocument10 pagesPrevencion de Ulceras DiabeticascarolvidaldonosoNo ratings yet
- SOCW 3004 Research ImplicationsDocument7 pagesSOCW 3004 Research ImplicationsTyler HemsworthNo ratings yet
- C4 Adjustment Disorder and Suicidal BehavioursDocument15 pagesC4 Adjustment Disorder and Suicidal BehavioursMilagros Saavedra RecharteNo ratings yet
- Mobile Psychiatry: Towards Improving The Care For Bipolar DisorderDocument10 pagesMobile Psychiatry: Towards Improving The Care For Bipolar DisorderGustavoNo ratings yet
- Jcad 12466Document14 pagesJcad 12466Kashyapi thakuriaNo ratings yet
- BMC Geriatrics: Smoking, Dementia and Cognitive Decline in The Elderly, A Systematic ReviewDocument7 pagesBMC Geriatrics: Smoking, Dementia and Cognitive Decline in The Elderly, A Systematic ReviewChristabella Natalia WijayaNo ratings yet
- Ashby-Mitchell 2017 ANU Prev PDFDocument8 pagesAshby-Mitchell 2017 ANU Prev PDFABC Four CornersNo ratings yet
- Seminar: Jason P Connor, Paul S Haber, Wayne D HallDocument11 pagesSeminar: Jason P Connor, Paul S Haber, Wayne D Hallapi-311409998No ratings yet
- Different Alcohol Types Trigger Specific EmotionsDocument14 pagesDifferent Alcohol Types Trigger Specific EmotionsTiziana de CarolisNo ratings yet
- A Pneumonia Outbreak Associated With ADocument20 pagesA Pneumonia Outbreak Associated With AandreaNo ratings yet
- A Pneumonia Outbreak Associated With ADocument20 pagesA Pneumonia Outbreak Associated With AandreaNo ratings yet
- Neurobiologia de La Distancia SocialDocument17 pagesNeurobiologia de La Distancia SocialandreaNo ratings yet
- The Neurological ManifestationsDocument13 pagesThe Neurological ManifestationsandreaNo ratings yet
- SARS-CoV-2 Emergency and Long-Term CognitiveDocument8 pagesSARS-CoV-2 Emergency and Long-Term CognitiveandreaNo ratings yet
- A Pneumonia Outbreak Associated With ADocument20 pagesA Pneumonia Outbreak Associated With AandreaNo ratings yet
- Deterioro Cognitivo Entre Individuos Con Antecedentes de Infección Leve Sintomática Por SARS CoV 2Document9 pagesDeterioro Cognitivo Entre Individuos Con Antecedentes de Infección Leve Sintomática Por SARS CoV 2andreaNo ratings yet
- Sistemas de Memoria R.historica PDFDocument9 pagesSistemas de Memoria R.historica PDFdilly castañoNo ratings yet
- Revision Hipocampo-InglesDocument3 pagesRevision Hipocampo-InglesandreaNo ratings yet
- Imagineria MotoraDocument22 pagesImagineria MotoraandreaNo ratings yet
- Hipocampo y Agmidala - InglesDocument44 pagesHipocampo y Agmidala - InglesandreaNo ratings yet
- Toma de Decisiones - Demencia Alcoholica XXXXDocument11 pagesToma de Decisiones - Demencia Alcoholica XXXXandreaNo ratings yet
- Aspectos Clinicos - EA - InglesDocument4 pagesAspectos Clinicos - EA - InglesandreaNo ratings yet
- INGLES Demencia Relacionada Con El Alcohol y Deterioro Neurocognitivo Un Estudio de RevisiónDocument9 pagesINGLES Demencia Relacionada Con El Alcohol y Deterioro Neurocognitivo Un Estudio de RevisiónandreaNo ratings yet
- Alcohol Consumption and Dementia Risk A Dose-Response Meta-Analysis of Prospective Studies.Document12 pagesAlcohol Consumption and Dementia Risk A Dose-Response Meta-Analysis of Prospective Studies.Saul MorenoNo ratings yet
- INGLES 2019 Consumo de Alcohol y Riesgo de Demencia y Deterioro Cognitivo Entre Adultos Mayores Con o Sin Deterioro Cognitivo LeveDocument13 pagesINGLES 2019 Consumo de Alcohol y Riesgo de Demencia y Deterioro Cognitivo Entre Adultos Mayores Con o Sin Deterioro Cognitivo LeveandreaNo ratings yet
- Magnetic Resonance Imaging in Alcoholic Korsakoff'sDocument8 pagesMagnetic Resonance Imaging in Alcoholic Korsakoff'sandreaNo ratings yet
- Frontal Dysfunction and Memory Deficits in The Alcoholic Korsako 1991Document22 pagesFrontal Dysfunction and Memory Deficits in The Alcoholic Korsako 1991andreaNo ratings yet
- Síndrome de Korsakoff Una Revisión Crítica.Document16 pagesSíndrome de Korsakoff Una Revisión Crítica.andreaNo ratings yet
- Demente AlcooliceDocument12 pagesDemente AlcooliceRoxana PascalNo ratings yet
- Kopelman 1995 SINDROME - KORSAKOFDocument21 pagesKopelman 1995 SINDROME - KORSAKOFandreaNo ratings yet
- Episodic and Working Memory Deficits in AlcoholicDocument13 pagesEpisodic and Working Memory Deficits in AlcoholicandreaNo ratings yet
- Episodic and Working Memory Deficits in AlcoholicDocument13 pagesEpisodic and Working Memory Deficits in AlcoholicandreaNo ratings yet
- Excellent Achievers Learning, Center, IncDocument5 pagesExcellent Achievers Learning, Center, IncJoyR.Alota100% (1)
- Planets in NakshatrasDocument6 pagesPlanets in Nakshatrasmurthyy55% (11)
- Science 10 Q3 - M2Document14 pagesScience 10 Q3 - M2Avha CortesNo ratings yet
- Carac Biogas FlamelessDocument7 pagesCarac Biogas FlamelessTaine EstevesNo ratings yet
- NURS FPX 6410 Assessment 2 Executive Summary To AdministrationDocument7 pagesNURS FPX 6410 Assessment 2 Executive Summary To Administrationzadem5266No ratings yet
- LinkageDocument47 pagesLinkageTony BernardNo ratings yet
- Eisenmenger SyndromeDocument6 pagesEisenmenger SyndromeWarkah SanjayaNo ratings yet
- 12 29 11editionDocument27 pages12 29 11editionSan Mateo Daily JournalNo ratings yet
- Cockerspaniel Pra CarriersDocument28 pagesCockerspaniel Pra CarriersJo M. ChangNo ratings yet
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document4 pagesInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDNo ratings yet
- Hitec 8888Z Atf C4 & To4 - TDSDocument2 pagesHitec 8888Z Atf C4 & To4 - TDSPranit More Arabian Petroleum LimitedNo ratings yet
- Brown Wolf ExerciseDocument8 pagesBrown Wolf ExerciseAarnav kumar0% (1)
- Climate Responsive ArchitectureDocument32 pagesClimate Responsive ArchitectureNikhila CherughattuNo ratings yet
- Invoice 0006-0827-Fnf: Invoice Date: Due Date: Source: Customer CodeDocument8 pagesInvoice 0006-0827-Fnf: Invoice Date: Due Date: Source: Customer CodeMini MiniNo ratings yet
- Zinc Silicate or Zinc Epoxy As The Preferred High Performance PrimerDocument10 pagesZinc Silicate or Zinc Epoxy As The Preferred High Performance Primerbabis1980100% (1)
- IR Beam LaunchingDocument2 pagesIR Beam LaunchingalfredoNo ratings yet
- Nath Bio-Genes at Inflection Point-2Document9 pagesNath Bio-Genes at Inflection Point-2vinodtiwari808754No ratings yet
- CHEM 333: Lab Experiment 5: Introduction To Chromatography : Thin Layer and High Performance Liquid ChromatographyDocument5 pagesCHEM 333: Lab Experiment 5: Introduction To Chromatography : Thin Layer and High Performance Liquid ChromatographymanurihimalshaNo ratings yet
- Lesson Plan Personality DisorderDocument7 pagesLesson Plan Personality DisorderRaj MeghwalNo ratings yet
- Directory of Acredited Medical Testing LaboratoriesDocument93 pagesDirectory of Acredited Medical Testing LaboratoriesCALIDAD METROMEDICA E.UNo ratings yet
- Ranitidine + OndansetronDocument7 pagesRanitidine + OndansetronAllicia PutriNo ratings yet
- Kaul Botanic AllopathyDocument7 pagesKaul Botanic AllopathyabhicwatNo ratings yet
- Structure of AtomDocument90 pagesStructure of Atomnazaatul aaklimaNo ratings yet
- ASTM C309: Do Liquid Hardeners Meet This Standard?Document2 pagesASTM C309: Do Liquid Hardeners Meet This Standard?Kishore Nayak kNo ratings yet
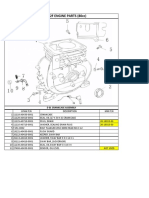
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- Nexgard For Dogs and Puppies Free 2 Day ShippingDocument1 pageNexgard For Dogs and Puppies Free 2 Day Shippinglyly23748No ratings yet
- Evolve Reach - Powered by HESIDocument7 pagesEvolve Reach - Powered by HESIangelsarerare14% (7)
- Reading ComprehensionDocument9 pagesReading Comprehensionxifres i lletres xifres i lletres100% (1)
- Aerobic ActivitiesExercises PDFDocument14 pagesAerobic ActivitiesExercises PDFPalma, Arrabela M.No ratings yet
- New Approaches To Cryopreservation of Cells, Tissues, and OrgansDocument19 pagesNew Approaches To Cryopreservation of Cells, Tissues, and OrgansLaura CursaruNo ratings yet