Professional Documents
Culture Documents
Articulo de Administracion
Uploaded by
PaulaReyOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Articulo de Administracion
Uploaded by
PaulaReyCopyright:
Available Formats
M a r k e t Wat c h
M a r k e t Watc h
Colombia’s Universal Health Insurance System
The results of providing health insurance for all in a middle-income
country.
by Ursula Giedion and Manuela Villar Uribe
ABSTRACT: By insuring more than 80 percent of its population, Colombia provides a valu-
able opportunity to gather evidence on a hotly debated health policy issue. Results from
three studies evaluating the impact of universal health insurance in Colombia show that it
has greatly increased access to and use of health services, even those that are free for all,
and has reduced the incidence of catastrophic health spending. The impact has been more
dramatic among those most vulnerable to health shocks: those living in rural areas, the
poorest, and the self-employed. [Health Affairs 28, no. 3 (2009): 853–863; 10.1377/
hlthaff.28.3.853]
T
h e p o s i t i v e e f f e c t of health insur- datory payroll tax contributions (11 percent).
ance coverage on the use of medical The government uses national and local tax
care has been widely demonstrated revenues and a payroll tax (1.5 percent) as a
and is generally accepted in the developed “solidarity contribution” (that is, a subsidy
world.1 However, little evidence is available from those who pay into the CR to help pur-
on the impact of health insurance in the de- chase coverage for those in the SR).
veloping world. n Benefit packages. Members of both
Hoping to reap the benefits of health insur- schemes have access to a package of specified
ance for its population, in 1993 Colombia ap- benefits. The CR package, known as the POS
proved a universal health insurance scheme (Plan Obligatorio de Salud), includes all levels
(Law 100) whereby all citizens, irrespective of of care, while the SR package, known as the
their ability to pay, are entitled to a compre- POSS (Plan Obligatorio de Salud Subsidiado),
hensive health benefit package. In Colombia’s covers most low-complexity care and cata-
system of universal health insurance, people strophic illnesses but provides only limited
participate in one of two regimes depending coverage for most hospital care and provides
on income: the Contributory Regime (CR), no short-term disability coverage (Exhibit 1).
which covers workers and their families with To fill the gap, the POSS is complemented by
monthly incomes above a minimum monthly services provided by public hospitals, financed
amount (approximately US$170 per month), through direct payments to providers inde-
and the Subsidized Regime (SR), which covers pendent of what services they supply and of
those identified as being poor through a proxy patients’ insurance status. According to the
means test. health reform law of 1993, those so-called sup-
n Financing. The CR is financed by man- ply-side subsidies should be transformed into
Ursula Giedion (ugiedion@gmail.com) is a consultant with the Brookings Institution in Bogota, Colombia.
Manuela Villar Uribe is a consultant with the World Bank Group in Washington, D.C.
H E A L T H A F F A I R S ~ Vo l u m e 2 8 , N u m b e r 3 853
DOI 10.1377/hlthaff.28.3.853 ©2009 Project HOPE–The People-to-People Health Foundation, Inc.
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
Health Tr a c k i n g
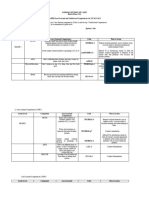
EXHIBIT 1
Characteristics Of The Contributory Regime (CR) And Subsidized Regime (SR) In
Colombia’s Universal Health Coverage Scheme, 2007
Characteristic CR SR
Population coverage
Target population Individuals and families with the ability to Eligible individuals as determined by a
pay: those employed earning at least one means test (Sistema de Identificación de
minimum salary; self-employed workers Beneficiarios, or SISBEN)
earning at least two minimum salaries
Number of enrollees, 2007a 21.5 million 18.2 million
Percentage of the total population 42% 50%
covered, 2007a
Contents of the benefit package
Family coverage Yes Yes
Public health education and outreach Full range of public health education Full range of public health education
and outreach services and outreach services
Preventive care, individual and family Full range of preventive services Full range of preventive services
Outpatient services (consultations, All All obstetric services, all pediatric
treatment, diagnostic tests, services for children under age one, low-
rehabilitation) complexity outpatient services, minor
trauma, glasses for children and the
aged, family planning
Dental care Basic care Basic care
Inpatient services All Hospitalization for low-complexity care;
all obstetric services; all pediatric
services for children under age one;
general surgery for herniorrhaphy,
appendectomy, cholecystectomy,
hysterectomy; orthopedic care
Medications All medications in national listing All medications in national listing
Catastrophic care Treatment with radiotherapy and Same as for CR
chemotherapy for cancer; dialysis and
organ transplant for renal failure; heart,
cerebrovascular, neurological, and
congenital surgeries; treatment of major
trauma; intensive care unit; hip and knee
replacement; major burns; treatment for
HIV/AIDS
Transportation For referrals, catastrophic care For referrals, catastrophic care
Excluded conditions Cosmetic surgery; fertility treatment; sleep Same as for CR plus all conditions not
disorder treatments; organ transplants listed above
(except renal, heart, corneal, and bone
marrow); long-term psychotherapy and
psychoanalysis; treatment for end-stage
renal disease
Maternity and sickness leaves Covered Not covered
SOURCE: Adapted from D. Pinto and W.C. Hsiao, “Colombia: Social Health Insurance with Managed Competition to Improve
Health Care Delivery,” in Social Health Insurance in Developing Nations, ed. W.C. Hsiao and P. Shaw (Washington: IBRD/World
Bank, 2007), 105–131.
a
National Health Survey 2007.
854 May/ June 2009
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
M a r k e t Wat c h
demand-side subsides, where insurance is sub- crease was especially dramatic among the low-
sidized for beneficiaries and insurers pay pro- est quintile of the population, rising from 6
viders for services actually delivered to their percent before the reform to more than 70 per-
clients. The aim is to achieve universal cover- cent by 2007. Furthermore, the current admin-
age with the same benefits in both regimes. istration aims to achieve universal coverage by
n Choice of insurers. In both the CR and 2010 by mobilizing new resources for the SR,
the SR, the insured person chooses an in- including the approval of an increase of payroll
surer—known as an Entidad Promotora de taxes from 11.5 percent to 12.5 percent, to be
Salud (EPS, meaning health-promoting entity) channeled to the SR.
in the CR and an Administradora del Regimen Despite the extraordinary increase in cov-
Subsidiado (ARS, meaning administrator of erage, criticism of Law 100 is omnipresent in
the subsidized regime) in the SR—whose Colombia, and calls for its complete overhaul
ownership may be public, private, or mixed are not uncommon. Many argue that the bene-
and which may be run either for profit or not fits of the current health system are unclear
for profit. In the CR, twenty-one health insur- and that the transformation of supply to de-
ance entities are available; 82 percent of en- mand subsidies has not advanced quickly
rollees are affiliated with a private EPS, while enough, leading to inefficiencies in the alloca-
18 percent are affiliated with a public EPS.2 tion of resources.7 Some also doubt whether
Forty-three different health insurance entities the major fiscal effort involved in financing the
operate in the SR; 44 percent of enrollees are SR—approximately 1 percent of GDP in
affiliated with a private EPS, and 42 percent 2003—has been worthwhile.8 Also, there are
are affiliated with either a public community- concerns that increased labor taxes will make
based or indigenous health plan.3 a stagnant formal employment situation
n Competition and contracting. Because worse.9 Others argue that the system is highly
prices and benefits are both determined by the inequitable, given the differences in the benefit
government, any competition among insurers packages provided for the poor and the
would be expected to be on the basis of qual- nonpoor; these critics seem to have forgotten
ity. The insurer contracts for health services that before 1993, the poor had no right to any
with a network of public, private, or own- explicit benefit package and that fiscal restric-
service providers (providers that are owned by tions do not allow the country to provide “ev-
the insurers themselves). To protect the finan- erything to everybody, now” but rather call for
cial sustainability of public hospitals, insurers a gradual extension of insurance coverage.
in the SR are forced to contract with the pub- n International views. International ob-
lic provider network for at least 40 percent of servers also have expressed contrasting and, to
the premiums. a certain extent, opposing views on whether
n Premiums and risk adjustment. The the Colombian system has been a success or an
government sets a unique premium with risk outright failure, often without citing much ev-
adjustment by age, sex, and location, to be paid idence. For example, a group from the World
to all insurers for each beneficiary. This pre- Bank observed in 2006: “The 1993 health sec-
mium is about US$244 per person per year in tor reform in Colombia is a good example of a
the CR and US$137 in the SR.4 successful government initiative to extend so-
n More recent developments. Before the cial health insurance to the poor.”10 Tony De
1993 reform, 24 percent of the population had Groote and colleagues concluded, conversely,
health coverage; by 2007, more than 80 percent that “some ten years after the implementation
had it, according to recently released data from of ‘Law 100,’ a review of the literature shows
the 2007 National Health Survey (NHS).5 This that the proposed goals of universal coverage
places Colombia among the very few countries and equitable access to high-quality care have
in the developing world reaching near- not been reached.”11 The important question is,
universal health insurance coverage.6 The in- then, What does the evidence really show?
H E A L T H A F F A I R S ~ Vo l u m e 2 8 , N u m b e r 3 855
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
Health Tr a c k i n g
Debate on whether health insurance is a the final choice depends on the specific cir-
worthwhile strategy to improve access to cumstances and often requires testing several
health care is not limited to Colombia. For ex- methods. As Richard Blundell and Monica
ample, a World Health Organization (WHO) Dias indicate, “The appropriate methodology
resolution adopted in 2005 called on member for non-experimental data depends on three
states to ensure that health financing systems factors: i) the type of information available to
include a method for prepayment of financial the researcher, ii) the underlying model and iii)
contributions for health care.12 At the same the parameter of interest.”16 The parameters of
time, a recent Joint NGO Briefing Paper criti- interest of the studies presented here are re-
cizes health insurance as a financing mecha- lated to access and utilization, health status,
nism by lamenting the lack of evidence on and financial protection, and no single house-
whether health insurance can work in low- hold survey pulls together data for all of these
income countries.13 It is hardly surprising, dimensions.
then, that many countries and international Although the 1995 and 2005 Colombian
organizations have followed the implementa- DHS surveys provide household data on ac-
tion of the Colombian health reform with in- cess, utilization, and health status, concentrat-
terest. In this context of national and interna- ing mostly on small children and women of re-
tional debate, evidence of the impact of this productive age, the LSMS 2003 provides
scheme not only provides important informa- information on general use of health care, out-
tion for policy making in Colombia but also of-pocket spending, and respondents’ socio-
provides lessons to other countries envision- economic characteristics (including income
ing similar reforms. and employment). Also, unlike DHS surveys,
This paper is a synthesis of three recent im- previous rounds of the LSMS are not compara-
pact evaluation studies on universal health in- ble, thereby limiting their use as a repeated
surance in Colombia.14 The main goal of these cross-section data set. The implications are
studies was to analyze existing survey data to fourfold.
evaluate the following three questions: (1) Has (1) Only a cross-section analysis (LSMS
insurance improved access to and use of health 2003) was available to evaluate the impact of
services both for the poor insured under the health insurance on financial protection in
SR and the nonpoor insured through the CR? both the CR and the SR. In the CR, an instru-
(2) Has insurance reduced the risk of out-of- mental variable (IV) approach was used; in the
pocket health spending that destabilizes or SR, a propensity score matching (PSM) tech-
impoverishes households? (3) Has insurance nique was more appropriate.
been able to positively affect health outcomes (2) The gradual implementation and still
among enrollees in the SR? incomplete coverage of the SR among the poor,
together with the existence of a repeated
Study Data And Methods cross-section data set (DHS 1995 and 2005),
To answer these questions, the studies syn- provided the unique opportunity to apply an
thesized here used an array of available data array of semiparametric methods (PSM, differ-
sources and methods. No randomized trial ence-in-difference, and matched double differ-
data were available to evaluate the impact of ence, or MDD), to identify differences in ac-
health insurance in Colombia, so the analysts cess, utilization, and health status between
had to rely on retrospective, already available those with insurance and those without it.
household survey data—namely, two rounds (3) The key issue when trying to establish
of the Demographic and Health Survey (DHS, causal relations between health insurance and
1995 and 2005) and one Living Standards health outcomes is selection bias (that is, are
Measurement Survey (LSMS, 2003).15 When members systematically different from non-
there are no experimental data, no clearly su- members in ways that also affect outcomes?).
perior impact evaluation method exists, and In the CR, membership is mainly determined
856 May/ June 2009
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
M a r k e t Wat c h
by employment status and income level. How- more important role. Also, insured children
ever, information on these determinants is who are coughing or suffering from diarrhea
available only in the LSMS, which does not are more likely than uninsured children to be
provide any health status variables that can be taken to a health care facility. This is impor-
expected to change as a consequence of bene- tant, because both acute respiratory infections
fits provided under the CR. Therefore, the and diarrheal diseases are still among the key
analysis of the CR did not look at the impact of causes of mortality among small children in
health insurance on health status. Colombia. Furthermore, insured women are
(4) The analysis of the impact of the CR somewhat more likely than uninsured women
was limited to a cross-sectional data set to give birth in a health facility and to be as-
(LSMS 2003), and the choice of methods was sisted by a doctor or other skilled health per-
restricted to either PSM or IV. Because a large sonnel, and they tend to receive more prenatal
majority of the target population of the CR is visits. Importantly, insured children are more
already insured, the construction of a suffi- likely than uninsured children to have their
ciently large control group using PSM was not immunization programs completed for their
possible, so the studies used IV.17 age and, therefore, are less likely to die from
PSM as well as double difference (DD) and vaccine-preventable diseases. The positive im-
MDD analyses were used to evaluate the im- pact of subsidized health insurance on mater-
pact of the SR on access, utilization, and nal care as well as on immunization coverage is
health status, while PSM was used to evaluate interesting, because these services are pro-
the impact of the SR on financial protection; vided free to everyone, irrespective of health
the IV approach was used to evaluate the im- insurance status. Health insurance affects uti-
pact of the CR on all outcome variables. In lization beyond affordability and may have an
each case, household-level data were com- effect on a provider’s way of interacting with
bined with administrative data at the munici- insured mothers (for example, by reminding
pal and departmental level and with block- them to immunize their children).
level census data related to the determinants One criticism of this analytic approach is
of membership and therefore used to control that it can only match individuals based on ob-
for potential selection bias.18 served variables. The results can be questioned
if there is reason to believe that there are sys-
Study Results tematic differences between the insured and
n SR: access and utilization. Using uninsured that are not accounted for by the
PSM, the average difference between matched matching process and that also influence out-
individuals is our estimate of the impact of the come variables. To test whether the analysis in
SR on selected outcome variables (Exhibit 2). Exhibit 2 can withstand this criticism, we im-
Regardless of the matching method used, the plemented an MDD analysis using data from
estimates confirm that the SR has improved the DHS 1995 and 2005 to correct for observ-
access for the poor. Those insured by the SR able and unobservable differences between the
are approximately 40 percent more likely to insured and the uninsured that did not change
have used outpatient visits in the past year (69 over time. The results largely confirm the pre-
percent of the insured versus 49 percent of the vious findings. For the smaller set of outcome
uninsured) and almost half as likely to have measures that were available in all three sur-
experienced barriers to access when needing veys, affiliation with the SR is consistently as-
care (25 percent and 42 percent, respectively). sociated with greater improvements in access
Insured people report problems with access for those it insures. Increases range from 42.0
resulting from limited supply more often than percentage points for prenatal visits to 10.7
the uninsured do, which is an indication that percentage points in the probability of taking
once health insurance reduces financial barri- children to a health care facility when they are
ers to access, other barriers begin to play a coughing (Exhibit 3). Even the probability of
H E A L T H A F F A I R S ~ Vo l u m e 2 8 , N u m b e r 3 857
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
Health Tr a c k i n g
EXHIBIT 2
Estimated Effect (Using Propensity Score Matching) Of Treatment On Treated People
For Access, Utilization, And Financial Protection Status, Colombia, 2005
Access and utilization Insured Uninsured
Had outpatient visit in past 12 months 0.687 0.488***
Not receiving medical care when needed 0.251 0.416***
Not receiving medical care when needed due to supply reasons 0.299 0.134***
Child taken to a health care facility when coughing 0.455 0.381***
Child taken to a health care facility when having diarrhea 0.365 0.296**
Birth in a health facility 0.865 0.815***
Birth attended by a doctor 0.809 0.755***
Birth attended by a skilled professional 0.855 0.801***
Child immunization complete 0.402 0.373**
Number of prenatal visits 5.513 5.177***
Financial protection
Catastrophic spending 0.3942 0.6080***
10% of capacity to pay 0.2783 0.4202***
20% of capacity to pay 0.2029 0.3136***
30% of capacity to pay 0.1594 0.1956*
40% of capacity to pay
Falls below endogenous poverty line 0.0609 0.0513
Falls below national poverty line 0.0638 0.1003*
Falls below national indigence line 0.0435 0.0414
Falls below endogenous or national poverty linea 0.0986 0.1407*
SOURCE: Authors’ calculations using data from the Demographic and Health Survey (DHS) 2005.
NOTES: Matching method: Kernel Eparechnikov (bandwidth 0.001). Other matching methods were implemented with very
similar results. Results from the use of these methods can be obtained from the authors upon request; send e-mail to Ursula
Giedion at ugiedion@gmail.com.
a
Endogenous (to the household) poverty line equals a basic household basket of goods and services.
*p < 0.10 **p < 0.05 ***p < 0.01
EXHIBIT 3
Estimates (Using Matched Double Difference) Of The Change In Health-Related
Outcome Variables In Colombia, Nationwide And By Urban/Rural Area, 1995–2005
Difference, 1995 to 2005
Access and utilization: outcome variables National Urban Rural
Child taken to a health care facility when coughing 0.107*** 0.090*** 0.078**
Child taken to a health care facility when having diarrhea 0.074** 0.099** 0.151**
Birth in a health facility 0.043*** 0.009 0.047**
Birth attended by a doctor 0.057*** 0.008 0.062**
Birth attended by a skilled professional 0.051*** 0.007 0.044**
Child immunization complete 0.061*** 0.041** 0.118***
Number of prenatal visits 0.420*** 0.172* 0.391**
SOURCE: Authors’ calculations using data from the Demographic and Health Survey (DHS) 2005.
*p < 0.10 **p < 0.05 ***p < 0.01
858 May/ June 2009
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
M a r k e t Wat c h
having complete immunization schedules in- ral areas, compared to a slightly more modest
creased by 6.1 percentage points for those in- increase from 53 percent to 70 percent in ur-
sured during 1995–2005. These results con- ban areas. The more important impact in rural
firm what has been found using PSM: health areas might be explained by overall worse
insurance has improved access even for those health indicators in rural areas and, conse-
services that by law should be free for all. quently, more room for improvement. Simi-
Although a comparison of health indicators larly, impact is found to be more important
at the national, urban, and rural levels shows among the poorest of the poor (lowest quin-
that they are still worse in rural compared to tile) compared to their somewhat wealthier
urban areas (Exhibit 4), health insurance neighbors (quintile 2).19 This indicates that
seems to matter more in the disadvantaged ru- subsidized health insurance is reducing equity
ral areas. For example, the percentage of births gaps not only in insurance coverage but also in
attended by a doctor is above 90 percent for all access to services.
childbearing women in urban areas but below n SR: impact of health insurance on
70 percent in rural areas. However, in urban health status. Evaluating the impact of health
areas, the increased probability of bringing insurance on health status is extremely com-
coughing children with insurance to a health plex. Possibly the most challenging issue is to
facility is 33 percent in rural areas, compared find appropriate variables for measuring
to only 15 percent in urban areas. Similarly, the health status and to capture changes in under-
probability of ambulatory visits increases from lying quality of life that can reasonably be re-
44 percent to 66 percent with insurance in ru- lated to improved access to services covered
EXHIBIT 4
Estimated Effect (Using Propensity Score Matching) Of Treatment On Treated People
For Access And Utilization Comparing The Urban/Rural And Poorest/Poor Quintiles,
Colombia, 2005
Urban Rural Poorest Poor
Access and utilization Treated Control Treated Control Treated Control Treated Control
Had outpatient visit in past 12
months 0.702 0.530*** 0.657 0.440*** 0.652 0.433*** 0.701 0.516***
Not receiving medical care when
needed 0.208 0.352*** 0.324 0.498*** 0.341 0.502*** 0.219 0.384***
Not receiving medical care when
needed due to supply reasons 0.267 0.133*** 0.348 0.172*** 0.348 0.158*** 0.294 0.138***
Child taken to a health care
facility when coughing 0.477 0.414*** 0.404 0.303*** 0.405 0.300*** 0.492 0.390***
Child taken to a health care
facility when having diarrhea 0.362 0.326 0.324 0.235 0.368 0.228** 0.379 0.358
Birth in a health facility 0.942 0.927* 0.747 0.684*** 0.744 0.694* 0.925 0.914
Birth attended by a doctor 0.901 0.875*** 0.678 0.637** 0.675 0.653 0.884 0.859
Birth attended by a skilled
professional 0.933 0.914** 0.74 0.698** 0.736 0.720 0.919 0.909
Child immunization complete 0.450 0.421* 0.329 0.311 0.349 0.321 0.436 0.410
Number of prenatal visits 5.767 5.805*** 5.167 4.549*** 4.739 4.425* 5.932 5.632*
SOURCE: Authors’ calculations using data from the Demographic and Health Survey (DHS) 2005.
NOTES: Matching method: Kernel Eparechnikov (bandwidth 0.001). Other matching methods were implemented with very
similar results. Results from the use of these methods can be obtained from the authors upon request; send e-mail to Ursula
Giedion at ugiedion@gmail.com.
*p < 0.10 **p < 0.05 ***p < 0.01
H E A L T H A F F A I R S ~ Vo l u m e 2 8 , N u m b e r 3 859
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
Health Tr a c k i n g
under the benefit packages. Additionally, Exhibit 5 presents estimates of the impact of
without any real panel data, it is difficult to health insurance provided in the CR on access,
know whether observed differences in health utilization, and financial protection. Health
status variables are the result of health insur- insurance significantly reduces access barriers
ance or whether the determination to get for both the self-employed and the employed.22
health insurance is partly a result of observed Unmet need has been reduced by 2 percent
health status. Given these difficulties, it among both groups. More importantly, health
should not be surprising that no conclusive ev- insurance has reduced financial barriers to ac-
idence emerges on the impact of health insur- cess by 14 percent among the employed and by
ance on the health status variables that are 47 percent among the self-employed. As in the
available in the DHS surveys. SR, the more important impact among the
n SR: impact of health insurance on fi- self-employed may be related to their tendency
nancial protection. According to the 2000 to have worse health than the employed, pro-
WHO report, one of the three main objectives viding more room for improvement. Other
of any health system is to protect the popula- supply-side barriers in the CR also tend to be
tion from the financial consequences of ill- more important among the insured once finan-
ness.20 Likewise, the World Bank strategy for cial barriers are removed (note, however, that
health, nutrition, and population mentions the this result is only barely significant among the
prevention of poverty through improved finan- employed). Moreover, access to medications
cial protection as one of its four main strategic has greatly improved with health insurance.
objectives.21 Health insurance is meant to pro- Results show that insurance increases the
vide financial protection by spreading the fi- use of both formal curative health care and
nancial risk associated with illness across a preventive services.23 Insurance in the CR has
pool of individuals. Evaluating the perfor- increased the likelihood of members’ using for-
mance of health insurance with regard to fi- mal care when ill by 57 percent among the em-
nancial protection was therefore a key objec- ployed and by 26 percent among the self-em-
tive of the studies summarized in this paper. ployed (Exhibit 5). Self-medication as a way of
Following the WHO, health-related out-of- meeting unmet demand when ill was 28 per-
pocket spending is classified as being “cata- cent less likely among employed members and
strophic” if it exceeds a specified portion of 15 percent less likely among self-employed
household nonsubsistence income (Exhibit 2). members when compared to uninsured peers.
Health insurance greatly reduces the probabil- Similarly, visiting a dentist or a general physi-
ity of incurring catastrophic expenditure. Re- cian for preventive reasons increased by 34
sults are statistically significant for different percent among the employed and by 46 per-
thresholds, but the statistical significance and cent among the self-employed.24
the size of the impact decreases as the percent- n CR: impact on financial protection.
age of income spent increases. This is probably Finally, as expected and consistent with the
related to the decreasing number of observa- reduction in financial access barriers, insur-
tions as the catastrophic spending amount ance has reduced the incidence of catastrophic
rises, which in turn mirrors the observation spending among both the self-employed and
that there are were few high-expenditure re- the employed. Results are statistically signifi-
spondents and many low-expenditure respon- cant for most thresholds of catastrophic
dents. This result may be related to the fact spending (Exhibit 5). For example, the inci-
that the SR covers mainly ambulatory care on dence of catastrophic spending drops by 61
the low end of health spending and cata- percent for the self-employed and by 13 per-
strophic illnesses such as AIDS and cancer at cent for the employed when considering all
the high end but provides only very limited households that had out-of-pocket health
coverage for tertiary care (Exhibit 1). spending that totaled 20 percent or more of
n CR: impact on access and utilization. their nonsubsistence income. The size of the
860 May/ June 2009
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
M a r k e t Wat c h
EXHIBIT 5
Results From Instrumental Variable (IV) Analysis: Estimated Treatment Effect On
Treated People For Access And Utilization In The Contributory Regime (CR), At The
National Level, Colombia, 2003
Difference
Self-employed and Formally employed and
Access and utilization their families their families
No health care use when having a health problem –0.021** –0.020*
Financial barrier to access –0.473** –0.144***
Supply-side barrier to access 0.090 –0.045*
Demand-side barrier to access –0.353* –0.210***
Access to medications (patient given all or any of the
prescribed medicines) 0.755*** 0.760***
Access to medications (patient given all of the
prescribed medicines) 0.516*** 0.568***
Timeliness of service for visit to general physician and dentist 1.525 –0.910*
Timeliness of service for visit to specialist –1.948 0.322
Formal health care services use 0.256*** 0.567***
Informal health care services use –0.052*** –0.027*
Preventive health care use (physician or dentist visit at least
once a year) 0.459*** 0.342***
Preventive health care use (physician and dentist visit at least
once a year) 0.152*** 0.272**
Self-medication when having a health problem –0.148*** –0.276***
Catastrophic spending
10% of capacity to pay –0.6227*** –0.2712***
20% of capacity to pay –0.6127*** –0.1310***
30% of capacity to pay –0.2720*** –0.0419
40% of capacity to pay –0.1394*** –0.0392***
Falls below endogenous poverty line –0.0127 –0.0287
Falls below national poverty line –0.4100 –0.0004***
Falls below national indigence line –0.0058 0
Falls below endogenous or national poverty linea –0.0599** –0.0004
SOURCE: Authors’ calculations.
a
Endogenous (to the household) poverty line equals a basic household basket of goods and services. Void cells indicate that
insufficient information was available for this variable and subsample.
*p < 0.10 **p < 0.05 ***p < 0.01
impact tends to be larger among the self-em- Concluding Comments
ployed than among the employed. Once again, Health insurance has introduced positive
this result is significant because the former changes in Colombia. Results presented here
tend to show worse health indicators than the indicate five important findings: (1) Insurance
latter, which makes improvements both more coverage not only has greatly increased for the
important and possibly easier to achieve. For general population but also has increased
example, 21 percent of all employed people among the poor and now reaches more than 80
needing health care experienced financial bar- percent of the population. (2) Health insur-
riers, compared to 35 percent among the self- ance in Colombia has improved access and uti-
employed. lization in both the SR and the CR. (3) Access
has improved even for services that are free for
all, regardless of insurance status. (4) Insur-
H E A L T H A F F A I R S ~ Vo l u m e 2 8 , N u m b e r 3 861
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
Health Tr a c k i n g
ance has reduced the incidence of catastrophic uating the impact of health insurance on
health spending. (5) The size of the impact health status using general household data has
tends to be larger among the more disadvan- many limitations. These limitations are dis-
taged groups; in the SR, those in rural areas cussed in greater detail in an online appen-
and those in the lowest income quintile benefit dix.27 Health insurance is a complex concept
more than those living in urban areas or the and encompasses many variables. It varies in
less poor. Moreover, although social health in- extent, duration, organization, and financing,
surance schemes are criticized for the diffi- and its impact will depend on the interplay be-
culty of attracting the self-employed, our re- tween all of these factors. Interesting opportu-
sults indicate that the benefits of insurance are nities for research exist for those wishing to
even more important among this group than understand the more complex implications of
for other insured people in the CR. health insurance on the provision of health
n Future agenda: policy. Colombia’s goal care and on health outcomes. Colombia’s expe-
of reaching universal coverage by 2010 seems rience can help other developing countries as
to be grounded on sufficient evidence. Despite they struggle with the same challenges in pro-
the positive impact of health insurance, viding equitable access to services for all.
though, much still remains to be done. First,
indicators of access and financial protection The authors thank Maria-Luisa Escobar for her
among the insured, such as the number of peo- constructive critique of earlier drafts of this paper.
ple not receiving care when in need and the They also thank Jacques van der Gaag, Paul Gertler,
percentage of women giving birth without the Mead Over, Alex Preker, and April Harding for their
assistance of a physician, still signify room for insightful and helpful comments. Preparation of this
improvement. Second, improving the quality synthesis paper was supported by the Global Health
of services should be a key objective now that Financing Initiative at the Brookings Institution. The
improvements in access and financial protec- opinions expressed herein are the authors’ and do not
tion have been obtained. Third, the more lim- necessarily reflect the views of Brookings.
ited extent of the benefit package in the SR
may explain why subsidized insurance does NOTES
not offer as much financial protection as does 1. See, for example, J. Hadley, “Sicker and Poorer—
the CR. This indicates the need to move in the The Consequences of Being Uninsured: A Re-
direction of equal coverage under both regimes view of the Research on the Relationship be-
while making certain not to jeopardize fiscal tween Health Insurance, Medical Care Use,
Health, Work, and Income,” Medical Care Research
sustainability. This issue is currently hotly de-
and Review 60, no. 2 Supp. (2003): 76S–112S.
bated in Colombia, as a recent ruling from the
2. Data for 2005 are from D. Pinto and W.C. Hsiao,
Constitutional Court has ordered the govern- “Colombia: Social Health Insurance with Man-
ment to provide full health coverage to the aged Competition to Improve Health Care Deliv-
population and unify the benefit packages of ery,” in Social Health Insurance in Developing Nations,
the CR and SR in the name of the fundamental ed. W.C. Hsiao and P. Shaw (Washington: IBRD/
human right to health and equity.25 Prelimi- World Bank, 2007), 105–131.
nary estimates indicate that this may cost 3. D. Pinto, “Colombia: Good Practices in Expand-
ing Health Care Coverage,” in Good Practices in
close to 20 percent of GDP at current levels.26 Health Financing, ed. P. Gottret et al. (Washington:
This situation clearly illustrates the tremen- World Bank, 2008), 137–182.
dous challenge of finding a balance between 4. In 2008, the premium was 430,488 Colombian
the guarantee of the fundamental right to pesos in the CR and 242,370 Colombian pesos in
health, the provision of comprehensive bene- the SR. The exchange rate in May 2008 was
fits, and the financial sustainability of health 1,767.4 Colombian pesos to one U.S. dollar.
systems not only in the developed world but 5. Although approved in December 1993, the SR did
not begin until 1996.
also increasingly in middle-income countries.
n Opportunity for further research. Eval- 6. See Hsiao and Shaw, eds., Social Health Insurance in
862 May/ June 2009
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
M a r k e t Wat c h
Developing Nations. 18. The administrative data included, among other
7. A. Gaviria et al., “Evaluating the Impact of Health indicators, the distance of the municipality from
Care Reform in Colombia: From Theory to Prac- the capital of the department, the level of politi-
tice,” Working Paper (Bogotá: Economic Devel- cal unrest as measured by the number of attacks
opment Research Center, 2006). by irregular armed forces, the average education
8. G. Barón, “Cuentas de salud de Colombia, 1993– level at the municipal level, the percentage of the
2003: El gasto nacional en salud y su financia- population with unmet basic needs, total re-
miento” (Bogotá: Ministerio de la Protección So- sources allocated to health, per capita income,
cial, 2007). and health insurance coverage at the municipal
level. Block-level census data from 1993 (prior to
9. Gaviria et al., “Evaluating the Impact.” the implementation of the health reform) in-
10. P.E Gottret et al., Health Financing Revisited: A Prac- cluded the following variables: percentage of
titioner’s Guide (Washington: World Bank, 2006). households with access to public services, pro-
11. T. De Groote, P. De Paepe, and J.P. Unger, “Co- portion of household members over age twelve,
lombia: In Vivo Test of Health Sector Privatiza- average number of household members, and per-
tion in the Developing World,” International Jour- centage of female-headed households.
nal of Health Services 31, no. 1 (2005): 125–141. 19. M.L. Escobar “Health Sector Reform in Colom-
12. WHO, “Achieving Universal Health Coverage: bia,” May 2005, http://www1.worldbank.org/
Developing the Health Financing System,” Tech- devoutreach/may05/article.asp?id=295 (accessed
nical Briefs for Policy-Makers no. 1 (Geneva: 1 June 2008).
WHO, 2005). 20. WHO, Health Systems: Improving Performance
13. Oxfam International, “Health Insurance in Low- (Geneva: WHO, 2000).
Income Countries,” Joint NGO Briefing paper no. 21. World Bank, Healthy Development: The World Bank
112, May 2008, http://www.oxfam.org/uk/ Strategy for Health, Nutrition, and Population Results,
resources/policy/health/downloads/bp112_ World Health Report (Washington: World
insurance.pdf (accessed 25 March 2009). Bank, 2007).
14. U. Giedion et al., “The Impact of Subsidized 22. An employed person works for a private com-
Health Insurance on Access, Utilization, and pany or government. A self-employed person is a
Health Status: The Case of Colombia” (Washing- day or unskilled laborer, an independent profes-
ton: World Bank, forthcoming); U. Giedion et al., sional, an independent worker of any other type,
“The Impact of Health Insurance in the Manda- an employer, or an independent farmer.
tory Contributory Regime on Access and Utili- 23. Services were deemed “formal” if a person having
zation: The Case of Colombia” (Washington: a health problem during the past month obtained
World Bank, forthcoming); and C.E Flórez et al., the services of a general physician, specialist,
“The Impact of Health Insurance in Colombia on dentist, health facility, nurse, or medical care-
Financial Protection” (Washington: World Bank, taker. Informal health care refers to respondents
forthcoming). who had a health problem during the past month
15. DHS surveys were carried out by PROFAMILIA and obtained the services of a pharmacist, apoth-
(a nongovernmental organization providing fam- ecary, traditional healer, and the like.
ily planning services) and jointly financed by 24. See Giedion et al., “The Impact of Subsidized In-
PROFAMILIA, the Instituto de Bienestar Famil- surance,” Annex Table 3.
iar (Institute for Family Welfare), the U.S.
Agency for International Development (USAID), 25. Constitutional Court Ruling no. T-760, J. Magis-
the Ministry of Social Protection, and the United ter Manuel Jose Cepeda Espinosa, Bogotá, 31 July
Nations Population Fund (UNFPA). The LSMS 2008.
was carried out and financed by the Departa- 26. J.C. Echeverry et al., “Monthly Report: Health
mento Nacional de Estadísticas (DANE, Na- System Crisis with Macro Consequences” (New
tional Department of Statistics). A table summa- York: Latin Source, 30 August 2008).
rizing the data sources and methods is available 27. See the online appendix, as in Note 15.
online at http://content.healthaffairs.org/cgi/
content/full/28/3/853/DC1.
16. R. Blundell and M.C. Dias, “Evaluation Methods
for Non-Experimental Data,” Fiscal Studies 21, no.
4 (2000): 427–446.
17. More details are provided in a technical appen-
dix, as in Note 15.
H E A L T H A F F A I R S ~ Vo l u m e 2 8 , N u m b e r 3 863
Downloaded from HealthAffairs.org on May 26, 2020.
Copyright Project HOPE—The People-to-People Health Foundation, Inc.
For personal use only. All rights reserved. Reuse permissions at HealthAffairs.org.
You might also like
- Family As A Unit of CareDocument59 pagesFamily As A Unit of Careabstabs83% (6)
- The Anatomy of The Philippine Health Care SystemDocument43 pagesThe Anatomy of The Philippine Health Care SystemMark Reynie Renz Silva100% (1)
- Fulvic Acid Minerals InformationDocument42 pagesFulvic Acid Minerals Informationdarlene918No ratings yet
- Comparative Models of Healthcare System: Canada: Group 6ADocument13 pagesComparative Models of Healthcare System: Canada: Group 6AAnonymouscat100% (1)
- Physiotherapy in DermatologyDocument18 pagesPhysiotherapy in DermatologyPraisy Roy67% (3)
- CASE 1 Lower Gastrointestinal BleedDocument9 pagesCASE 1 Lower Gastrointestinal BleedAzizan Hanny100% (1)
- Community Health NursingDocument91 pagesCommunity Health NursingJanelle Gift SenarloNo ratings yet
- Health Financing: Dr. Jamelah R. Usman-PasagiDocument27 pagesHealth Financing: Dr. Jamelah R. Usman-PasagiGada AbdulcaderNo ratings yet
- Presentation On Health Care System ModelsDocument37 pagesPresentation On Health Care System ModelsTashi Makpen100% (1)
- Detailed Lesson Plan in Physical EducationDocument7 pagesDetailed Lesson Plan in Physical EducationSherelyn RiveraNo ratings yet
- CHN Complete NotesDocument237 pagesCHN Complete NotesMelody B. Miguel100% (1)
- Healthcare, Actually: A Brief Review of International Healthcare, America's Challenges, and Steps Towards Universal HealthcareFrom EverandHealthcare, Actually: A Brief Review of International Healthcare, America's Challenges, and Steps Towards Universal HealthcareNo ratings yet
- Ukzn Mmed (Fammed) - Copc Module STUDY GUIDE 2007/8Document18 pagesUkzn Mmed (Fammed) - Copc Module STUDY GUIDE 2007/8Jardee DatsimaNo ratings yet
- Nursing AssistantDocument58 pagesNursing AssistantswarnaNo ratings yet
- Philippine Health Agenda - Dec1 - 1 PDFDocument26 pagesPhilippine Health Agenda - Dec1 - 1 PDFreyalene gallegosNo ratings yet
- Australia - International Health Care System ProfilesDocument10 pagesAustralia - International Health Care System ProfilesAboubacar SompareNo ratings yet
- 1b Nu710 International Health Systems 1Document11 pages1b Nu710 International Health Systems 1api-678571963No ratings yet
- A Layman's Guide To The U.S. Health Care System: OrganizationDocument19 pagesA Layman's Guide To The U.S. Health Care System: OrganizationFilip IonescuNo ratings yet
- Medical Health Insurance Systems in Europe, USA, Canada, and AustraliaDocument13 pagesMedical Health Insurance Systems in Europe, USA, Canada, and Australiaeko abiNo ratings yet
- Health Care SystemDocument8 pagesHealth Care Systemp6dzs6z4m9No ratings yet
- International Health SystemsDocument9 pagesInternational Health Systemsapi-643329064No ratings yet
- Community Health NursingDocument12 pagesCommunity Health NursingFatima Medriza DuranNo ratings yet
- Health Insurance: Awareness, Utilization, and Its Determinants Among The Urban Poor in Delhi, IndiaDocument8 pagesHealth Insurance: Awareness, Utilization, and Its Determinants Among The Urban Poor in Delhi, IndiaY S KusumaNo ratings yet
- Definitions and Abbreviations: Adequacy, A Private Health Insurer Must Have, and Comply With, A Written, BoardDocument2 pagesDefinitions and Abbreviations: Adequacy, A Private Health Insurer Must Have, and Comply With, A Written, BoardmcaNo ratings yet
- Colombia: A Healthcare System in CrisisDocument6 pagesColombia: A Healthcare System in CrisisMelissa SierraNo ratings yet
- Ess 5Document12 pagesEss 5api-582020074No ratings yet
- Philippine Health Agenda 2016 2022Document32 pagesPhilippine Health Agenda 2016 2022Caren Gelarzo50% (2)
- 3 Revised Presentation of Sec. Ubial 6 13 2017Document24 pages3 Revised Presentation of Sec. Ubial 6 13 2017Kristel Joy Verzon-BunaganNo ratings yet
- 6 Philippine Health Agenda Paulyn Rosell UbialDocument24 pages6 Philippine Health Agenda Paulyn Rosell UbialJoshNo ratings yet
- Unit Ii CHNDocument17 pagesUnit Ii CHNKryza CastilloNo ratings yet
- PHC Week1day1 Group2 - PPT-GHDocument21 pagesPHC Week1day1 Group2 - PPT-GHReichelle Reine LisingNo ratings yet
- Primary Health Care The BuildingDocument4 pagesPrimary Health Care The BuildingZurNo ratings yet
- Community Health Nursing Lecture 107-Pages-Pg.-116-222Document107 pagesCommunity Health Nursing Lecture 107-Pages-Pg.-116-222ShiraishiNo ratings yet
- Health Policy Brief: Telehealth Parity LawsDocument5 pagesHealth Policy Brief: Telehealth Parity Lawsnadia nuraniNo ratings yet
- 2.1. Definition of Health Care SystemDocument12 pages2.1. Definition of Health Care SystemSittie Aina MunderNo ratings yet
- Pmed.1001676 n2Document3 pagesPmed.1001676 n2jaime polancoNo ratings yet
- Social Security Health Model: The Four Essential Functions of A Health SystemDocument4 pagesSocial Security Health Model: The Four Essential Functions of A Health SystemChristian Shane BejeranoNo ratings yet
- HealthInsurance Ashortcasestudy RASDocument4 pagesHealthInsurance Ashortcasestudy RASRitesh KumarNo ratings yet
- Pembiayaan Kesehatan UHCDocument43 pagesPembiayaan Kesehatan UHCGenre PesselNo ratings yet
- PHC - 1 Copied LecturesDocument21 pagesPHC - 1 Copied Lectureshiraya789No ratings yet
- Critical Review of NITIDocument5 pagesCritical Review of NITIPiyush SinghNo ratings yet
- 19571Document30 pages19571Prasanjeet BhattacharjeeNo ratings yet
- UHC Country Support PDFDocument12 pagesUHC Country Support PDFdiah irfainiNo ratings yet
- Paulyn Jean B. Rosell-Ubial, MD, MPH, Ceso Ii: Secretary of HealthDocument32 pagesPaulyn Jean B. Rosell-Ubial, MD, MPH, Ceso Ii: Secretary of HealthAnonymous h2EnKyDbNo ratings yet
- B. How Are Health Services Organized?: Debit Bagas Kamal Gumilang 1506735181Document5 pagesB. How Are Health Services Organized?: Debit Bagas Kamal Gumilang 1506735181Debit Bagas Kamal GumilangNo ratings yet
- PHC CasestudyDocument13 pagesPHC CasestudyVia Kristel ZapantaNo ratings yet
- Kakoloti - Key Issues Facing The Health Sector in The Next Five Years (2007)Document19 pagesKakoloti - Key Issues Facing The Health Sector in The Next Five Years (2007)Dinesh PatelNo ratings yet
- Philippine Health Agenda 2016-2022Document32 pagesPhilippine Health Agenda 2016-2022Alyssa NicoleNo ratings yet
- Midterm Reviewer in POLGOVDocument16 pagesMidterm Reviewer in POLGOVJam AlindadaNo ratings yet
- Community Health NursingDocument5 pagesCommunity Health NursingJayne VenturanzaNo ratings yet
- Stjernsward WHO Public Health Appr To PC JPSM 0705Document8 pagesStjernsward WHO Public Health Appr To PC JPSM 0705fatmawatiNo ratings yet
- 2CNN - Uhc - Final Na FinalDocument67 pages2CNN - Uhc - Final Na FinalPhi SalvadorNo ratings yet
- Nhip & Uhca (7875)Document29 pagesNhip & Uhca (7875)Mae Joan AbanNo ratings yet
- medical english作業 PDFDocument10 pagesmedical english作業 PDFeric483460No ratings yet
- Some Key Messages On NhiDocument10 pagesSome Key Messages On NhiJonathan BorleyNo ratings yet
- Unit 2Document14 pagesUnit 2Moumita MondalNo ratings yet
- All Pregnant Women at Risk of Such Complication.: Yakap As It Is Necessarily Safe and Provides QualityDocument3 pagesAll Pregnant Women at Risk of Such Complication.: Yakap As It Is Necessarily Safe and Provides QualityNathalie kate petallarNo ratings yet
- Group B Presentation 2Document40 pagesGroup B Presentation 2Doaa AwadNo ratings yet
- Primary Health Care 2021Document43 pagesPrimary Health Care 2021Mohammad AyyashNo ratings yet
- Pages From IJPHRD February - 2020-3Document5 pagesPages From IJPHRD February - 2020-3Tengiz VerulavaNo ratings yet
- National Health Policy 2017newDocument29 pagesNational Health Policy 2017newDayana CheriyanNo ratings yet
- ICTM111 PDF 02 - Healthcare System, Health System Framework & PH Health SystemDocument4 pagesICTM111 PDF 02 - Healthcare System, Health System Framework & PH Health SystemJamNo ratings yet
- IPC in L0ng Term Care FacilitiesDocument26 pagesIPC in L0ng Term Care FacilitieskusnilaNo ratings yet
- National Health Policies and Community HealthcareDocument14 pagesNational Health Policies and Community Healthcareatharva sawantNo ratings yet
- CHN Notes2Document12 pagesCHN Notes2PAOLA LUZ CRUZNo ratings yet
- Achieving the Human Right to a Caring Society in an Aging AmericaFrom EverandAchieving the Human Right to a Caring Society in an Aging AmericaNo ratings yet
- Least Learned Skills in MapehDocument6 pagesLeast Learned Skills in MapehDiana ValienteNo ratings yet
- 5 Asphyxia NeonetrumDocument27 pages5 Asphyxia NeonetrumRana VandanaNo ratings yet
- NG Pháp Trang 8Document4 pagesNG Pháp Trang 8Thithanhkieu TranNo ratings yet
- Human Rights and HIV - Need of A Law For PLHAsDocument11 pagesHuman Rights and HIV - Need of A Law For PLHAsbatuksidNo ratings yet
- Case Study 2Document29 pagesCase Study 2drnasim20088171No ratings yet
- Walia 2018Document56 pagesWalia 2018Andre Arcondo LopezNo ratings yet
- NCM 33 Framework For Maternal and Child Health Nursing: ST ST RD ND TH TH RD TH TH THDocument5 pagesNCM 33 Framework For Maternal and Child Health Nursing: ST ST RD ND TH TH RD TH TH THSherika Mariz Moreno GuarinNo ratings yet
- The Medical TranscriptionistDocument22 pagesThe Medical TranscriptionistrimeoznekNo ratings yet
- Comparative Analysis of Health Policy ImplementationDocument9 pagesComparative Analysis of Health Policy ImplementationGabriel da RochaNo ratings yet
- Alcohol Abstinence in Drinkers With Atrial FibrillationDocument16 pagesAlcohol Abstinence in Drinkers With Atrial FibrillationDaniela PopNo ratings yet
- Algorithm EVALI Nov 2019Document1 pageAlgorithm EVALI Nov 2019ALBERTUS ANDIKA WONGJAYANo ratings yet
- Care ReportDocument23 pagesCare ReportSindi Muthiah UtamiNo ratings yet
- BPKM English Term 1 - Primary Healthcare System - 2019-2020Document95 pagesBPKM English Term 1 - Primary Healthcare System - 2019-2020Melati ArienaNo ratings yet
- Managementof Ardhavabhedaka Through PanchakarmaDocument7 pagesManagementof Ardhavabhedaka Through PanchakarmaPNo ratings yet
- RCT+Appraisal+sheets. TherapyDocument2 pagesRCT+Appraisal+sheets. Therapydian_c87No ratings yet
- Analysis of The Factors Responsible For Water Pollution in Rural CommunitiesDocument57 pagesAnalysis of The Factors Responsible For Water Pollution in Rural CommunitiesUsman Ahmad TijjaniNo ratings yet
- FDA警告信(中国)中英文对照20220106Document16 pagesFDA警告信(中国)中英文对照20220106lewis liNo ratings yet
- Digitalization in Nursing ServicesDocument4 pagesDigitalization in Nursing ServicesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Superwarfarin:: A Wifes Means To An Evil EndDocument14 pagesSuperwarfarin:: A Wifes Means To An Evil EndgarciamattNo ratings yet
- MSDS NaphtholDocument2 pagesMSDS NaphtholEarl CielNo ratings yet
- AWARUN, Tunde M&E ResuméDocument2 pagesAWARUN, Tunde M&E ResuméSurgeGrid LogisticNo ratings yet
- Expomed Eurasia 2020 BrochureDocument8 pagesExpomed Eurasia 2020 BrochurectyvteNo ratings yet
- Dwnload Full Introduction To Abnormal Child and Adolescent Psychology 2nd Edition Weis Test Bank PDFDocument36 pagesDwnload Full Introduction To Abnormal Child and Adolescent Psychology 2nd Edition Weis Test Bank PDFeffusiveflooder936r8o100% (15)