You might also like
- Labor-Vaginal Delivery Anne Jones, 17 Years Old Case Study With Complete Solutions 2023Document13 pagesLabor-Vaginal Delivery Anne Jones, 17 Years Old Case Study With Complete Solutions 2023CHARLES MAINANo ratings yet
- Grand Case Presentation - GastroschisisDocument88 pagesGrand Case Presentation - Gastroschisisjoanevangelio100% (2)
- Maternity Case 3: Brenda Patton (Core) : Guided Reflection QuestionsDocument3 pagesMaternity Case 3: Brenda Patton (Core) : Guided Reflection QuestionsDai Nguyen100% (1)
- Vsim Case Sara Lin Virtual ClinicalDocument12 pagesVsim Case Sara Lin Virtual ClinicalLivan Martell100% (4)
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- Nursing Care Plan: Mrs Rajbr Kaur Lecturer OBGDocument20 pagesNursing Care Plan: Mrs Rajbr Kaur Lecturer OBGKavi rajput92% (24)
- Case Presentation Placenta PreviaDocument37 pagesCase Presentation Placenta PreviaJasmin Sabna100% (3)
- Iii. Textbook Discussion A. Definition: Predisposing Factors Precipitating FactorsDocument3 pagesIii. Textbook Discussion A. Definition: Predisposing Factors Precipitating FactorsVianne Arcenio100% (1)
- NCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care For High-Risk PregnancyDocument7 pagesNCM 107 Learning Packet On Related Learning Experience Rle Focus Unit: Care For High-Risk PregnancyMelinda Cariño BallonNo ratings yet
- Case Study On Ectopic PregnancyDocument15 pagesCase Study On Ectopic PregnancyNew Whatsapp Status Video100% (8)
- Kayla Flaskerud Vsim BP Concept Map, Isbar, ClincialDocument12 pagesKayla Flaskerud Vsim BP Concept Map, Isbar, ClincialCameron Janzen100% (1)
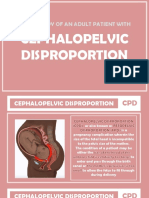
- Cephalopelvic DisproportionDocument93 pagesCephalopelvic Disproportionkyle cunanan100% (6)
- Discharge Plan: Patient'S Outcome Criteria Nursing OrderDocument2 pagesDischarge Plan: Patient'S Outcome Criteria Nursing OrdergaeLtorvzNo ratings yet
- DR - Nazira Sadique Final Obg Preterm NeonatesDocument58 pagesDR - Nazira Sadique Final Obg Preterm NeonatesSiddharth M.No ratings yet
- Discharge PlanDocument2 pagesDischarge PlanVraxx GrayNo ratings yet
- Cholecystitis-Nursinghealth History and PeDocument9 pagesCholecystitis-Nursinghealth History and PeBelen SoleroNo ratings yet
- Nursing: Ns. Ketut Lisnawati, S.Kep., M.Kep., SP - Kep.M.BDocument24 pagesNursing: Ns. Ketut Lisnawati, S.Kep., M.Kep., SP - Kep.M.BNi Made Ananda Candra Rahmitha Putri KepakisanNo ratings yet
- Scenario Cast 4Document6 pagesScenario Cast 4Ahmad AlbadawiNo ratings yet
- Nursing Case Study ApaleDocument14 pagesNursing Case Study ApaleAna LuisaNo ratings yet
- Prabhat KC Gye LogDocument9 pagesPrabhat KC Gye LogprabhatNo ratings yet
- 23219-Article Text-71141-1-10-20211130Document7 pages23219-Article Text-71141-1-10-20211130Vera Viviana Deo GraciaNo ratings yet
- Esteroides Canada 2019Document21 pagesEsteroides Canada 2019Ana Isabel Rincon GalvezNo ratings yet
- Quizzes SubsDocument36 pagesQuizzes SubsApril Mae Agomo-oNo ratings yet
- Aspirin For Evidence-Based Preeclampsia Prevention Trial: Effect of Aspirin On Length of Stay in The Neonatal Intensive Care UnitDocument6 pagesAspirin For Evidence-Based Preeclampsia Prevention Trial: Effect of Aspirin On Length of Stay in The Neonatal Intensive Care UnitAripin Ari AripinNo ratings yet
- Breast CancerDocument30 pagesBreast CancerLester Paul SivilaNo ratings yet
- ASGE 2012 Endoscopy in Pregnant and Lactating WomenDocument7 pagesASGE 2012 Endoscopy in Pregnant and Lactating WomenjordanNo ratings yet
- Maduracion Pulmonar Jurnal Obstetric CanadaDocument21 pagesMaduracion Pulmonar Jurnal Obstetric CanadaSoy PatoNo ratings yet
- Simulated-Learning Case StudyDocument6 pagesSimulated-Learning Case StudyChristopher jan LegaspiNo ratings yet
- Insidence of Fever in Labor and Risk of Neonatal SepsisDocument5 pagesInsidence of Fever in Labor and Risk of Neonatal SepsisSNFauziaNo ratings yet
- Dilation and CurettageDocument8 pagesDilation and CurettageIrish Eunice FelixNo ratings yet
- Final Case Study IndividualDocument38 pagesFinal Case Study IndividualAna LuisaNo ratings yet
- NEW Tugas Dr. Ahmad Ridwan, MO, MSC 2Document36 pagesNEW Tugas Dr. Ahmad Ridwan, MO, MSC 2dr.rinanovitriani94No ratings yet
- Gallery WalkDocument9 pagesGallery WalkCZAR VINCENT WAYNE SEVANDAL BAYLONNo ratings yet
- NCM116-LESSON3-RLE Pre-OperativeDocument6 pagesNCM116-LESSON3-RLE Pre-OperativeMilcah NuylesNo ratings yet
- Poster Anesthetic Management in For Emergency Caesarean Section in Pregnant Women With MeningiomaDocument1 pagePoster Anesthetic Management in For Emergency Caesarean Section in Pregnant Women With MeningiomapriNo ratings yet
- MATERNALDocument26 pagesMATERNALadisdjkfbNo ratings yet
- Acute PainDocument4 pagesAcute PainRuffy AbdulazisNo ratings yet
- National Board Examination - Kiki Dwi QoriDocument18 pagesNational Board Examination - Kiki Dwi QoriHendra WardhanaNo ratings yet
- Weekly Task at Pediatric Intensive Unite (Picu) 1Document9 pagesWeekly Task at Pediatric Intensive Unite (Picu) 1Reem ApadiNo ratings yet
- Apendicitis y Embarazo 2Document6 pagesApendicitis y Embarazo 2Bernardo RomeroNo ratings yet
- Case Analysis Medicine NursingDocument31 pagesCase Analysis Medicine NursingAleks MendozaNo ratings yet
- Ob Topic 3 - Multiple Pregnancy - NCPDocument2 pagesOb Topic 3 - Multiple Pregnancy - NCPThelly MargalloNo ratings yet
- A Case Series On Severe COVID 19 Infection in Antenatal PatientsDocument4 pagesA Case Series On Severe COVID 19 Infection in Antenatal PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- PIIS0002937820311923Document3 pagesPIIS0002937820311923FebbyNo ratings yet
- Respiratory Distress Syndrome of The Newborn JCG0086 v3Document17 pagesRespiratory Distress Syndrome of The Newborn JCG0086 v3meutia salsabilaNo ratings yet
- Sedation and Analgesia in Children Undergoing Invasive ProceduresDocument7 pagesSedation and Analgesia in Children Undergoing Invasive ProceduresSantosa TandiNo ratings yet
- Ectopic PregnancyDocument38 pagesEctopic PregnancyLovelyjade ReyesNo ratings yet
- Nifedipin Untuk PretermDocument31 pagesNifedipin Untuk PretermMonia Agni WiyatamiNo ratings yet
- DP Discharge Plan@@@@@@@@Document6 pagesDP Discharge Plan@@@@@@@@Maemae SumalinogNo ratings yet
- BSN 2-4 - 2V - MCN CASE STUDY (Final)Document100 pagesBSN 2-4 - 2V - MCN CASE STUDY (Final)Angeline ShackletonNo ratings yet
- OSCE Sp1 Feto Breech PresentationDocument7 pagesOSCE Sp1 Feto Breech PresentationobbyNo ratings yet
- Dada Chapter 3Document20 pagesDada Chapter 3jolayemi aanuNo ratings yet
- Case Analysis Medicine NursingDocument14 pagesCase Analysis Medicine NursingAleks MendozaNo ratings yet
- 266-Article Text-1026-1-10-20191108Document6 pages266-Article Text-1026-1-10-20191108Cecilia CabanagNo ratings yet
- Student Guide JaundiceDocument2 pagesStudent Guide JaundiceAnna StacyNo ratings yet
- Pre Test CA3 EPI IMCI Mother and Child With Rationale and Answer 2Document20 pagesPre Test CA3 EPI IMCI Mother and Child With Rationale and Answer 2Scarlet GrayNo ratings yet
- Bookshelf NBK550970Document17 pagesBookshelf NBK550970Lucas WillianNo ratings yet
- Intrauterine Fetal Death: College of Health SciencesDocument49 pagesIntrauterine Fetal Death: College of Health SciencesAce TabioloNo ratings yet
- Cancer Treatment and the Ovary: Clinical and Laboratory Analysis of Ovarian ToxicityFrom EverandCancer Treatment and the Ovary: Clinical and Laboratory Analysis of Ovarian ToxicityNo ratings yet
- Tantalizing Therapeutics in Bronchopulmonary DysplasiaFrom EverandTantalizing Therapeutics in Bronchopulmonary DysplasiaVineet BhandariNo ratings yet
- Answer:: Present A Table of The Following: 1.childhood Immunization TableDocument1 pageAnswer:: Present A Table of The Following: 1.childhood Immunization TableKristinelou Marie N. ReynaNo ratings yet
- Documents-To-Be-Attached-In-Folder-4sets 1Document19 pagesDocuments-To-Be-Attached-In-Folder-4sets 1Kristinelou Marie N. ReynaNo ratings yet
- Lesson Preview: Make Healthy Food ChoicesDocument2 pagesLesson Preview: Make Healthy Food ChoicesKristinelou Marie N. ReynaNo ratings yet
- Rle 4Document2 pagesRle 4Kristinelou Marie N. ReynaNo ratings yet
- Sas 1 HaDocument1 pageSas 1 HaKristinelou Marie N. ReynaNo ratings yet
- Lesson Preview: Checking For UnderstandingDocument2 pagesLesson Preview: Checking For UnderstandingKristinelou Marie N. ReynaNo ratings yet
- CN Nerve ScriptDocument4 pagesCN Nerve ScriptKristinelou Marie N. ReynaNo ratings yet
- Physical Examination: Name: REYNA, Kristinelou Marie N. Sas 4Document2 pagesPhysical Examination: Name: REYNA, Kristinelou Marie N. Sas 4Kristinelou Marie N. ReynaNo ratings yet
- Lesson Title: Assessing Older AdultsDocument8 pagesLesson Title: Assessing Older AdultsKristinelou Marie N. ReynaNo ratings yet
- MUSCULOSKELETAL Assessment ScripyDocument2 pagesMUSCULOSKELETAL Assessment ScripyKristinelou Marie N. ReynaNo ratings yet
- Physical Examination of A Pediatric Patient Patient: Name: REYNA, Kristinelou Marie N. Sas 5Document1 pagePhysical Examination of A Pediatric Patient Patient: Name: REYNA, Kristinelou Marie N. Sas 5Kristinelou Marie N. ReynaNo ratings yet
- Retdem Script NeuroDocument2 pagesRetdem Script NeuroKristinelou Marie N. ReynaNo ratings yet
- Interviewing and Communication: Name: REYNA, Kristinelou Marie N. Sas 3Document1 pageInterviewing and Communication: Name: REYNA, Kristinelou Marie N. Sas 3Kristinelou Marie N. ReynaNo ratings yet
- Sas 2 HaDocument1 pageSas 2 HaKristinelou Marie N. ReynaNo ratings yet
- Sas2 NDDocument9 pagesSas2 NDKristinelou Marie N. ReynaNo ratings yet
- Sas5 NDDocument4 pagesSas5 NDKristinelou Marie N. ReynaNo ratings yet
- Breastmilk Protective Factors: Lesson PreviewDocument2 pagesBreastmilk Protective Factors: Lesson PreviewKristinelou Marie N. ReynaNo ratings yet
- Sas24 ND LabDocument3 pagesSas24 ND LabKristinelou Marie N. ReynaNo ratings yet