You might also like
- OriginalarticleDocument10 pagesOriginalarticlemy accountNo ratings yet
- New England Journal Medicine: The ofDocument8 pagesNew England Journal Medicine: The ofAmrit KaurNo ratings yet
- A Study Oncytopenias and The Factors Associated With Cytopenias Among Hiv Infected Patients Admitted at A Tertiary Care HospitalDocument8 pagesA Study Oncytopenias and The Factors Associated With Cytopenias Among Hiv Infected Patients Admitted at A Tertiary Care HospitalIJAR JOURNALNo ratings yet
- Adherence To Nucleos (T) Ide Analogue PDFDocument8 pagesAdherence To Nucleos (T) Ide Analogue PDFVirgo WNo ratings yet
- Blood Transfusion Safety in Low-Resourced Countries: Aspiring To A Higher StandardDocument3 pagesBlood Transfusion Safety in Low-Resourced Countries: Aspiring To A Higher Standardvivekgupta58636No ratings yet
- Colorectal BundlesDocument16 pagesColorectal BundlesDamie ChaulaNo ratings yet
- Hospital-Acquired InfectionsDocument13 pagesHospital-Acquired InfectionsBolivar IseaNo ratings yet
- Glaser 2017Document7 pagesGlaser 2017Dicky StefanusNo ratings yet
- COVID-19 Anticoagulant 2Document15 pagesCOVID-19 Anticoagulant 2faris nagibNo ratings yet
- Walz 2015Document9 pagesWalz 2015Margarida ReisNo ratings yet
- Singer2014 PDFDocument5 pagesSinger2014 PDFMigs MedinaNo ratings yet
- Articulo NeumoniaDocument7 pagesArticulo NeumoniaEd BarajasNo ratings yet
- 10) Blood Culture Contaminants - S.dawsonDocument10 pages10) Blood Culture Contaminants - S.dawsonimaguestuserNo ratings yet
- Efficacy of Red Blood Cell Transfusion in The Critically Ill (Original Article)Document8 pagesEfficacy of Red Blood Cell Transfusion in The Critically Ill (Original Article)Rayhan OemarNo ratings yet
- Prevention of Infection in Patients With Cancer Evidence Based Nursing InterventionsDocument10 pagesPrevention of Infection in Patients With Cancer Evidence Based Nursing InterventionsAkshayNo ratings yet
- Sources of Variation - Patient, Provider, and Setting SourcesDocument20 pagesSources of Variation - Patient, Provider, and Setting SourcesAbacuc MendozaNo ratings yet
- Baugh Et Al-2017-Academic Emergency MedicineDocument9 pagesBaugh Et Al-2017-Academic Emergency MedicineRovanNo ratings yet
- Chakra - Factors Associated With Complications of C DiffDocument8 pagesChakra - Factors Associated With Complications of C DiffCherry SmileNo ratings yet
- Journal of Infection: SciencedirectDocument8 pagesJournal of Infection: SciencedirectKarina Dwi SwastikaNo ratings yet
- Catheter-Associated Urinary Tract Infections in Intensive Care Unit PatientsDocument7 pagesCatheter-Associated Urinary Tract Infections in Intensive Care Unit PatientsHaris AnsarNo ratings yet
- Severe Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerDocument8 pagesSevere Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerFaki D'pasnizerNo ratings yet
- Strategies To Prevent Central Line-Associated Bloodstream Infections in Acute Care - 1836 - 21-07-13-15-29-36Document20 pagesStrategies To Prevent Central Line-Associated Bloodstream Infections in Acute Care - 1836 - 21-07-13-15-29-36Marcela Rios HernandezNo ratings yet
- 01 CCM 0000119424 31648 1eDocument6 pages01 CCM 0000119424 31648 1eumi far ainNo ratings yet
- Ciz 1049Document9 pagesCiz 1049Justin WilliemNo ratings yet
- Effect of Procalcitonin-Guided AntibioticDocument11 pagesEffect of Procalcitonin-Guided AntibioticRaul ContrerasNo ratings yet
- Alok A. Khorana - Incidence and Predictors of Venous Thromboembolism (VTE) Among Ambulatory High-RiskDocument8 pagesAlok A. Khorana - Incidence and Predictors of Venous Thromboembolism (VTE) Among Ambulatory High-RiskFarid RakhmanNo ratings yet
- Seroprevalence of Human Immunodeficiency Virus InfDocument5 pagesSeroprevalence of Human Immunodeficiency Virus InfAbe AguiarNo ratings yet
- Clabsi Qi Martinez GibbsDocument11 pagesClabsi Qi Martinez Gibbsapi-437349589100% (1)
- Patel 1108 eDocument12 pagesPatel 1108 eIgnacia VergaraNo ratings yet
- Sepse TimmingDocument15 pagesSepse TimmingVictor Hugo SilveiraNo ratings yet
- Hepatology - 2019 - Ghany - Hepatitis C Guidance 2019 Update American Association For The Study of Liver DiseasesDocument36 pagesHepatology - 2019 - Ghany - Hepatitis C Guidance 2019 Update American Association For The Study of Liver DiseasesAndrei CemîrtanNo ratings yet
- GammaglobulinaDocument7 pagesGammaglobulinaIván Gustavo Magaña CeballosNo ratings yet
- Funding: Tracheal Intubation in COVID-19 Patients: Update On Recommendations. Response To BR J Anaesth 2020 125: E28e37Document3 pagesFunding: Tracheal Intubation in COVID-19 Patients: Update On Recommendations. Response To BR J Anaesth 2020 125: E28e37Muhammad RenaldiNo ratings yet
- 2023 - Epidemiology and Outcomes of Hospital Acquired Bloodstream Infections in Intensive Care Unit Patients The EUROBACT 2Document13 pages2023 - Epidemiology and Outcomes of Hospital Acquired Bloodstream Infections in Intensive Care Unit Patients The EUROBACT 2giseladlrNo ratings yet
- JVECC Consensus Antithrombotics Main DocumentDocument25 pagesJVECC Consensus Antithrombotics Main DocumentTzu YinNo ratings yet
- NIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisDocument23 pagesNIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisjaneNo ratings yet
- Catheter Related Infxts JANDocument20 pagesCatheter Related Infxts JANyvettejzNo ratings yet
- Guidelines For Viral Hepatitis Surveillance and Case ManagementDocument54 pagesGuidelines For Viral Hepatitis Surveillance and Case ManagementKinan BasalimNo ratings yet
- Jurnal TBC Inter 1Document5 pagesJurnal TBC Inter 1sekti lindaNo ratings yet
- Association of Vitamin D Status and Acute RhinosinusitisDocument6 pagesAssociation of Vitamin D Status and Acute RhinosinusitisnicloverNo ratings yet
- Covid-19 and Coagulation: Bleeding and Thrombotic Manifestations of Sars-Cov-2 InfectionDocument12 pagesCovid-19 and Coagulation: Bleeding and Thrombotic Manifestations of Sars-Cov-2 InfectionDavid Mamani CardenasNo ratings yet
- Multidrug-Resistant Bacterial Infections in U.S. Hospitalized Patients, 2012-2017Document11 pagesMultidrug-Resistant Bacterial Infections in U.S. Hospitalized Patients, 2012-2017sebastianNo ratings yet
- Title Authors:: Snarain@northwell - EduDocument17 pagesTitle Authors:: Snarain@northwell - EduPaola A. Zeña HuancasNo ratings yet
- Video 4 PDFDocument9 pagesVideo 4 PDFMirza RisqaNo ratings yet
- HIV Screening USPTFDocument21 pagesHIV Screening USPTFhivpolicyyesNo ratings yet
- 2020 Article 2138Document10 pages2020 Article 2138Andi Tiara S. AdamNo ratings yet
- Umapathy 2017Document11 pagesUmapathy 2017Karinaayu SerinNo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- Transfusion - 2019 - Vossoughi - Safety Incident Reports Associated With Blood TransfusionsDocument6 pagesTransfusion - 2019 - Vossoughi - Safety Incident Reports Associated With Blood Transfusionsvivekgupta58636No ratings yet
- Healthcare-Associated Infection in Developing CountriesDocument6 pagesHealthcare-Associated Infection in Developing Countriesmaryametouti01No ratings yet
- Jurnal RhinoDocument7 pagesJurnal RhinoElvienNo ratings yet
- Comparison of Medical Versus Surgical Management of Peritonsillar Abscess: A Retrospective Observational StudyDocument6 pagesComparison of Medical Versus Surgical Management of Peritonsillar Abscess: A Retrospective Observational Studycharoline gracetiani nataliaNo ratings yet
- AmbulasiDocument12 pagesAmbulasiRafii KhairuddinNo ratings yet
- Internal Medicine Journal - 2017 - Fernando - Healthcare Acquired Infections Prevention StrategiesDocument11 pagesInternal Medicine Journal - 2017 - Fernando - Healthcare Acquired Infections Prevention StrategiesMimi ElagoriNo ratings yet
- Journal Pone 0243782Document12 pagesJournal Pone 0243782wenyNo ratings yet
- MMF Si VHC TransplantDocument11 pagesMMF Si VHC TransplantdeliaNo ratings yet
- Journal Pmed 1003501Document28 pagesJournal Pmed 1003501Abi HinojosaNo ratings yet
- Strategies to Prevent Catheter-Associated Urinary Tract InfectionsDocument17 pagesStrategies to Prevent Catheter-Associated Urinary Tract InfectionsKiran SurageNo ratings yet
- Concepts and Methods in Infectious Disease SurveillanceFrom EverandConcepts and Methods in Infectious Disease SurveillanceNkuchia M. M'ikanathaNo ratings yet
- Decision Analytics and Optimization in Disease Prevention and TreatmentFrom EverandDecision Analytics and Optimization in Disease Prevention and TreatmentNan KongNo ratings yet
- Allergic Transfusion Reactions: William J. Savage, MD, PHDDocument4 pagesAllergic Transfusion Reactions: William J. Savage, MD, PHDNausheenNo ratings yet
- Ma Ramica 2019Document4 pagesMa Ramica 2019NausheenNo ratings yet
- Blood Transfusion Guideline PDFDocument26 pagesBlood Transfusion Guideline PDFEmhemed Amer TabibNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument19 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsNausheenNo ratings yet
- Clinical Transfusion Practice Guidelines For Medical Interns BangladeshDocument42 pagesClinical Transfusion Practice Guidelines For Medical Interns Bangladeshratriprimadiati100% (1)
- 2011 Blood TransfusionDocument6 pages2011 Blood TransfusionJeanne Mae Lee AfallaNo ratings yet
- Dissertation GuidelinesDocument56 pagesDissertation GuidelinesNayar RafiqueNo ratings yet
- Blood Transfusion Guideline PDFDocument26 pagesBlood Transfusion Guideline PDFEmhemed Amer TabibNo ratings yet
- Andreu 2002Document9 pagesAndreu 2002NausheenNo ratings yet
- Unified Glare Rating As A Measure of Visual ComfortDocument4 pagesUnified Glare Rating As A Measure of Visual ComforthoangacNo ratings yet
- The Difficult Patient' As Perceived by Family Physicians: Dov Steinmetz and Hava TabenkinDocument6 pagesThe Difficult Patient' As Perceived by Family Physicians: Dov Steinmetz and Hava TabenkinRomulo Vincent PerezNo ratings yet
- Group Assignment For Quantitative: Analysis For Decisions MakingDocument45 pagesGroup Assignment For Quantitative: Analysis For Decisions Makingsemetegna she zemen 8ተኛው ሺ zemen ዘመንNo ratings yet
- Human Behavior in OrganizationsDocument5 pagesHuman Behavior in OrganizationsJennybabe Peta100% (1)
- Advance Corporate StrategyDocument2 pagesAdvance Corporate StrategyPassionate_to_LearnNo ratings yet
- COVID-19 Impact on Philippine ExportsDocument5 pagesCOVID-19 Impact on Philippine ExportsHazel BorboNo ratings yet
- Law On Sales: Perfection Stage Forms of Sale When Sale Is SimulatedDocument21 pagesLaw On Sales: Perfection Stage Forms of Sale When Sale Is SimulatedRalph ManuelNo ratings yet
- Uti MF v. Ito 345 Itr 71 - (2012) 019taxmann - Com00250 (Bom)Document8 pagesUti MF v. Ito 345 Itr 71 - (2012) 019taxmann - Com00250 (Bom)bharath289No ratings yet
- Hydrogen Plant For The New MillenniumDocument21 pagesHydrogen Plant For The New Millenniumapi-3799861100% (2)
- Psychrometrics Drying Problems SEODocument5 pagesPsychrometrics Drying Problems SEOStephanie Torrecampo Delima100% (2)
- Auditing Theory - Audit ReportDocument26 pagesAuditing Theory - Audit ReportCarina Espallardo-RelucioNo ratings yet
- Haukongo Nursing 2020Document86 pagesHaukongo Nursing 2020Vicky Torina ShilohNo ratings yet
- DAA UNIT-3 (Updated)Document33 pagesDAA UNIT-3 (Updated)pilli maheshchandraNo ratings yet
- Sensory Marketing: How Toothpaste Brands Appeal to the SensesDocument17 pagesSensory Marketing: How Toothpaste Brands Appeal to the SensesNavodi RathnasingheNo ratings yet
- A Teacher Education ModelDocument128 pagesA Teacher Education ModelMelinda LabianoNo ratings yet
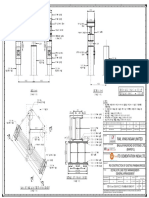
- Routine Pile Load Test-Ga-13.04.2021Document1 pageRoutine Pile Load Test-Ga-13.04.2021Digambar JadhavNo ratings yet
- SQL Server Management Studio Database Engine Query Editor Window - Microsoft DocsDocument6 pagesSQL Server Management Studio Database Engine Query Editor Window - Microsoft DocsAchamyeleh TamiruNo ratings yet
- 2021 Subsector OutlooksDocument24 pages2021 Subsector OutlooksHungNo ratings yet
- WheelHorse Power Take Off Manual 8-3411Document4 pagesWheelHorse Power Take Off Manual 8-3411Kevins Small Engine and Tractor ServiceNo ratings yet
- The Effect of Multicollinearity in Nonlinear Regression ModelsDocument4 pagesThe Effect of Multicollinearity in Nonlinear Regression ModelsKeshav PoolaNo ratings yet
- New Product Introduction Process: August 16, 2016Document30 pagesNew Product Introduction Process: August 16, 2016JuliaChenNo ratings yet
- Coal Petroleum: Crude OilDocument25 pagesCoal Petroleum: Crude Oiljojo basenNo ratings yet
- ExcelDocument1 pageExcelJosh KempNo ratings yet
- Compound Sentences FANBOYS WorksheetDocument7 pagesCompound Sentences FANBOYS WorksheetVerenice SuarezNo ratings yet
- Plastic PackagingDocument47 pagesPlastic PackagingRajaSekarsajja100% (1)
- Tutorial MagIC Net 2.XDocument99 pagesTutorial MagIC Net 2.XJuan Diego Aznar Fernández100% (1)
- Service Driven Logistics System - Basic Service CapabilityDocument12 pagesService Driven Logistics System - Basic Service CapabilityAnusha Sunkara80% (5)
- Comments PRAG FinalDocument13 pagesComments PRAG FinalcristiancaluianNo ratings yet
- What is Cultural Heritage and Why it's ImportantDocument3 pagesWhat is Cultural Heritage and Why it's ImportantMiguel A. González LópezNo ratings yet