You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- ISX15 E5 4954042 Wiring Diagram Rev 4Document3 pagesISX15 E5 4954042 Wiring Diagram Rev 4刘sir82% (17)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CIGRE Brochure348Document114 pagesCIGRE Brochure348christiansasso100% (5)
- Ethical TheoriesDocument18 pagesEthical TheoriesKlyde EvangelistaNo ratings yet
- Dissonant Loss: The Experiences of Donor Relatives: Social Science & Medicine December 1996Document13 pagesDissonant Loss: The Experiences of Donor Relatives: Social Science & Medicine December 1996royfockerNo ratings yet
- What Makes Protest Powerful? Reintroducing and Elaborating Charles Tilly'S Wunc ConceptDocument24 pagesWhat Makes Protest Powerful? Reintroducing and Elaborating Charles Tilly'S Wunc ConceptroyfockerNo ratings yet
- Qualitative Text AnalysisDocument5 pagesQualitative Text AnalysisroyfockerNo ratings yet
- The Statistics of Causal Inference: A View From Political MethodologyDocument23 pagesThe Statistics of Causal Inference: A View From Political MethodologyroyfockerNo ratings yet
- Essential Skills and Qualities of A Successful AcademicDocument7 pagesEssential Skills and Qualities of A Successful AcademicMagda GacparskaNo ratings yet
- Energía Solar La Creciente Solución Solar en Las Zonas Rurales de América LatinaDocument3 pagesEnergía Solar La Creciente Solución Solar en Las Zonas Rurales de América LatinawilderNo ratings yet
- Andrea Janine Lucina M4W4 Media and Information SourcesDocument3 pagesAndrea Janine Lucina M4W4 Media and Information SourcesJomein Aubrey BelmonteNo ratings yet
- Sample Fees Calculation Sheet For Mixed ProjectDocument6 pagesSample Fees Calculation Sheet For Mixed Projectssmorthy8053No ratings yet
- Super Star Group: Subject: Work Order For Supply of Switch With Box SingleDocument29 pagesSuper Star Group: Subject: Work Order For Supply of Switch With Box SingleAntora HoqueNo ratings yet
- V7 Host Implementation Guide v2.0.6 - LiquorDocument54 pagesV7 Host Implementation Guide v2.0.6 - LiquorShubham Namdev100% (1)
- Mayer+empl: Architectural Space InterventionDocument55 pagesMayer+empl: Architectural Space InterventionQuirin EmplNo ratings yet
- Program ATP EMTP in Overvoltage EducationDocument4 pagesProgram ATP EMTP in Overvoltage Educationrodrigoct88No ratings yet
- 4 - Classical Management 2Document64 pages4 - Classical Management 2Prof. Maseera PatelNo ratings yet
- Emotional Intelligence ExerciseDocument8 pagesEmotional Intelligence Exercisem.syedNo ratings yet
- Internal - External ReportsDocument2 pagesInternal - External ReportsSarahCariagaNo ratings yet
- Stevenson Hinde2007Document7 pagesStevenson Hinde2007Fuel45No ratings yet
- AI For Decision Making Wharton 10722Document18 pagesAI For Decision Making Wharton 10722Pra RNo ratings yet
- Ds AutoCADDocument2 pagesDs AutoCADfl_in1No ratings yet
- 04 Unit 03 Procedure-KCDocument19 pages04 Unit 03 Procedure-KCfitriNo ratings yet
- Xy-lanh-dien-loai-truot-SMC-LEFS-Series 29012018105735 PDFDocument183 pagesXy-lanh-dien-loai-truot-SMC-LEFS-Series 29012018105735 PDFĐặng HoàngNo ratings yet
- Practical Research RRLDocument6 pagesPractical Research RRLtriciaprivate000No ratings yet
- Monarch TT 30Document4 pagesMonarch TT 30Migue ToasaNo ratings yet
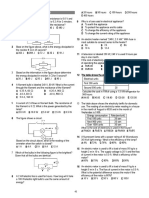
- Physics! Unit 03 MTM Packet 2013Document8 pagesPhysics! Unit 03 MTM Packet 2013Kelly O'SheaNo ratings yet
- Hi Focus f152 HBDocument4 pagesHi Focus f152 HBAna Bogdanovic GagiNo ratings yet
- JRVelasco - Lesson 21, Art AppreciationDocument4 pagesJRVelasco - Lesson 21, Art AppreciationJon Ruemer Pontawe VelascoNo ratings yet
- Lloyd'S Register Integrated Fatigue Design: Assessment SystemDocument17 pagesLloyd'S Register Integrated Fatigue Design: Assessment SystemAna TNo ratings yet
- Markets and DestinationDocument55 pagesMarkets and DestinationJorim Sumangid100% (1)
- Tutorial 7.5Document2 pagesTutorial 7.5sidNo ratings yet
- Uniaxial Loading: Design For Strength, Stiffness, and Stress ConcentrationsDocument11 pagesUniaxial Loading: Design For Strength, Stiffness, and Stress ConcentrationsDanishIqbalNo ratings yet
- The ABC's of Interviewing: A Is For AttitudeDocument5 pagesThe ABC's of Interviewing: A Is For AttitudeSnehal PatilNo ratings yet
- Group 14 Monitoring SystemDocument27 pagesGroup 14 Monitoring SystemAndrei 26No ratings yet