You might also like
- High Utility WordsDocument17 pagesHigh Utility Wordstripathi.ankit557No ratings yet
- Bob Boyce - Inventor's Terminal Cancer Courtesy of Verichip - Targeted IndividualsDocument13 pagesBob Boyce - Inventor's Terminal Cancer Courtesy of Verichip - Targeted IndividualsTortured-Targeted-Individuals100% (2)
- Bruxism Hypnosis Script No. 2Document12 pagesBruxism Hypnosis Script No. 2Eva Jacinto100% (2)
- Obsessive Compulsive DisorderDocument54 pagesObsessive Compulsive DisorderMARIA STEPHANY DELA CRUZNo ratings yet
- Abpsych Barlow Reviewer 1 Abpsych Barlow Reviewer 1Document30 pagesAbpsych Barlow Reviewer 1 Abpsych Barlow Reviewer 1Sharemax Holdings, Inc.No ratings yet
- Guerilla DNA Recovery and Regeneration - Herbs and Energy RecalibrationFrom EverandGuerilla DNA Recovery and Regeneration - Herbs and Energy RecalibrationNo ratings yet
- Ulladu Narpadu - AnubandhamDocument18 pagesUlladu Narpadu - AnubandhamChris Bell100% (2)
- Anticipatory GrievingDocument2 pagesAnticipatory GrievingKM100% (5)
- Abhinavagupta Chatterjee Gautam TR Sri Tantraloka Chapter Two 242p PDFDocument242 pagesAbhinavagupta Chatterjee Gautam TR Sri Tantraloka Chapter Two 242p PDFMihai Bolinteanu100% (2)
- Defence Expo2022Document111 pagesDefence Expo2022Jyotsna Pandey50% (2)
- Maka - PCN 673 Sensory Processing Disorder Brochure 1Document2 pagesMaka - PCN 673 Sensory Processing Disorder Brochure 1api-643707075No ratings yet
- Bhrigu SutrasDocument56 pagesBhrigu Sutrasu_daveNo ratings yet
- Killing Demons - Working With The PhurbaDocument4 pagesKilling Demons - Working With The PhurbaFelipe Facklam100% (2)
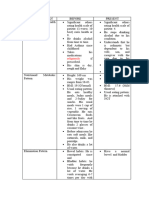
- Physical Assessment: Appeara Nce and Mental Status Actual Findings Normal Findings AnalysisDocument6 pagesPhysical Assessment: Appeara Nce and Mental Status Actual Findings Normal Findings AnalysisiammaiaNo ratings yet
- Orthodontic Space Closure After First Molar Extraction Without Skeletal AnchorageDocument10 pagesOrthodontic Space Closure After First Molar Extraction Without Skeletal AnchoragepatriciabdsNo ratings yet
- NCP Disturbed Thought Process Related To SchizophreniaDocument6 pagesNCP Disturbed Thought Process Related To Schizophrenianaishel0% (1)
- DocxDocument5 pagesDocxYuyun Purwita SariNo ratings yet
- Focused Diagnosis and Treatment Plan SOAP: NURS - 607Document2 pagesFocused Diagnosis and Treatment Plan SOAP: NURS - 607Ashley Constant McCammonNo ratings yet
- Focused Diagnosis and Treatment Plan SOAP: NURS - 607Document1 pageFocused Diagnosis and Treatment Plan SOAP: NURS - 607Ashley Constant McCammonNo ratings yet
- McCammon Focused Assessment #1Document2 pagesMcCammon Focused Assessment #1Ashley Constant McCammonNo ratings yet
- Vocabulary and Memorization IntroductionDocument54 pagesVocabulary and Memorization IntroductionMD. MAYEN HOSSAINNo ratings yet
- Progressive Supranuclear Palsy. Kam Newman, Saeed KahkeshaniDocument1 pageProgressive Supranuclear Palsy. Kam Newman, Saeed KahkeshanijingerbrunoNo ratings yet
- Letting GoDocument1 pageLetting GoshivaniNo ratings yet
- Observation of Students: APST Standard 1Document4 pagesObservation of Students: APST Standard 1api-525881488No ratings yet
- Q3-COT PPT - HEALTH7 - WEEK2 (Kinds of Stress)Document20 pagesQ3-COT PPT - HEALTH7 - WEEK2 (Kinds of Stress)Ronalyn RuizNo ratings yet
- October 2023Document4 pagesOctober 2023api-348082105No ratings yet
- Physical Assessment Part 1 AssignmentDocument11 pagesPhysical Assessment Part 1 AssignmentKyra Bianca R. FamacionNo ratings yet
- Dyspareunia in Women Jurnal TranslateDocument13 pagesDyspareunia in Women Jurnal TranslateYuni IHNo ratings yet
- Ajp 132 11 1222-bDocument2 pagesAjp 132 11 1222-bPoluteNo ratings yet
- Psychological ReportDocument4 pagesPsychological ReportEllouise SaramosingNo ratings yet
- Siete Pecados Capitales InglesDocument1 pageSiete Pecados Capitales InglesDamian GuilcapiNo ratings yet
- The Vocal Overdoer Syndrome: A Useful Concept From The Voice ClinicDocument3 pagesThe Vocal Overdoer Syndrome: A Useful Concept From The Voice ClinicChrisNo ratings yet
- Npi and ReadingDocument10 pagesNpi and ReadingCHARLEMAIGNE RECOMESNo ratings yet
- Week 3 PerdevDocument3 pagesWeek 3 PerdevJeff PasiaNo ratings yet
- Gordon's Functional Pattern Pattern Prior To Hospitalization During Hospitalization Analysis/ InterpretationDocument15 pagesGordon's Functional Pattern Pattern Prior To Hospitalization During Hospitalization Analysis/ InterpretationMitchelle Mé Frances CamilonNo ratings yet
- Smoke Buddy!: By: Subhojit Dhar Vishesh Soni Sujal Bansal Uday Bhaskar Gajavalli Tejaditya SankranthiDocument14 pagesSmoke Buddy!: By: Subhojit Dhar Vishesh Soni Sujal Bansal Uday Bhaskar Gajavalli Tejaditya SankranthiVishesh SoniNo ratings yet
- Gordon ERDocument3 pagesGordon ERJaica marie Dela rosaNo ratings yet
- Exceptionality Significants or Key Features Causes / Etiology CharacteristicsDocument3 pagesExceptionality Significants or Key Features Causes / Etiology CharacteristicsMelanie AplacaNo ratings yet
- Group B - Process RecordingDocument5 pagesGroup B - Process RecordingMa. Sofia Andrei AlcabazaNo ratings yet
- Case PresentationDocument15 pagesCase PresentationJohn PaciaNo ratings yet
- Eob Osce Class of 2016Document4 pagesEob Osce Class of 2016HongMingNo ratings yet
- ПрезентаціяанглійськааDocument3 pagesПрезентаціяанглійськааМаряна КухарNo ratings yet
- Physical AssessmentDocument3 pagesPhysical AssessmentallyssaNo ratings yet
- Gordon'S 11 Functional Health PatternDocument6 pagesGordon'S 11 Functional Health Patternkathcute15No ratings yet
- Nursesteachingppt 090506092047 Phpapp02Document19 pagesNursesteachingppt 090506092047 Phpapp02Gerome ManantanNo ratings yet
- Nursing Care PlanDocument1 pageNursing Care PlandaleascabanoNo ratings yet
- Perumal Murugan's Hall of MirrorsDocument1 pagePerumal Murugan's Hall of MirrorsLuis A. GómezNo ratings yet
- Health AssessmentDocument9 pagesHealth AssessmentJane MartinNo ratings yet
- Remegia Family Genogram: 303315toledocitysceincehs@deped - Gov.phDocument3 pagesRemegia Family Genogram: 303315toledocitysceincehs@deped - Gov.phJonrheym RemegiaNo ratings yet
- Participle ClauseDocument6 pagesParticiple ClausemohammadNo ratings yet
- ASSESMENTFINALFINALDocument4 pagesASSESMENTFINALFINALlovelove DayoNo ratings yet
- Child With Develotmental DelayDocument2 pagesChild With Develotmental DelayDwi TyoNo ratings yet
- ORSOLINO - Process Recording - Working PhaseDocument8 pagesORSOLINO - Process Recording - Working PhaseEkay OrsolinoNo ratings yet
- Understanding Change Fatigue and Change ResistanceDocument11 pagesUnderstanding Change Fatigue and Change ResistanceFlo ChikoworeNo ratings yet
- Psychological Complexities of Visual RestorationDocument4 pagesPsychological Complexities of Visual RestorationDewi NofiantiNo ratings yet
- Anxiety NCPDocument2 pagesAnxiety NCPkuro hanabusaNo ratings yet
- Observe Level of Consciousness: P CostureDocument5 pagesObserve Level of Consciousness: P CostureMarshannette Dela CernaNo ratings yet
- Idiom - IdiomsDocument13 pagesIdiom - IdiomsNguyễn Ý VyNo ratings yet
- Q3 - M2 - Use Cohesive Devices AppropriatelyDocument6 pagesQ3 - M2 - Use Cohesive Devices AppropriatelyKarina PiosNo ratings yet
- Camouflaged Shame (Uncensored): A Path to Redemption After Military Sexual TraumaFrom EverandCamouflaged Shame (Uncensored): A Path to Redemption After Military Sexual TraumaNo ratings yet
- Shell of Soul: Secrets Revealed - The Consequences of Past Life Influences and HealthFrom EverandShell of Soul: Secrets Revealed - The Consequences of Past Life Influences and HealthNo ratings yet
- Van de Ven, Explaining Development and Change 1995Document31 pagesVan de Ven, Explaining Development and Change 1995Alejandra Calderón DíazNo ratings yet
- Project Management Plan Template WsDocument2 pagesProject Management Plan Template WsAbdel bakiNo ratings yet
- KLS Gogte Institute of Technology, Belagavi.: "F Distribution"Document15 pagesKLS Gogte Institute of Technology, Belagavi.: "F Distribution"2GI20MCA87Sushma MerawadeNo ratings yet
- Logic Circuits IndiabixDocument59 pagesLogic Circuits IndiabixAlexander Fabros SolivenNo ratings yet
- SALT TriageDocument2 pagesSALT TriageThe DoctorNo ratings yet
- Specific Module 2Document16 pagesSpecific Module 2Johnsel PansoyNo ratings yet
- Written Report ON Ethical Issues IN Media CoverageDocument3 pagesWritten Report ON Ethical Issues IN Media CoverageEMMANo ratings yet
- Capillary TubeDocument8 pagesCapillary Tubeziko23100% (2)
- Arjun Dhaliwal - Sustainability Paper For My Hospital 2Document7 pagesArjun Dhaliwal - Sustainability Paper For My Hospital 2api-540469046No ratings yet
- Slowotworstwo Kontekst Business 250 2Document16 pagesSlowotworstwo Kontekst Business 250 2a.strefnelNo ratings yet
- Diagnostic Studies For Osteosarcoma: CBC (WBC) ESR Serum Alkaline Phosphatase Alkaline PhosphataseDocument2 pagesDiagnostic Studies For Osteosarcoma: CBC (WBC) ESR Serum Alkaline Phosphatase Alkaline PhosphatasekyawNo ratings yet
- Solar Parks: Accelerating The Growth of Solar Power in IndiaDocument5 pagesSolar Parks: Accelerating The Growth of Solar Power in IndiaNiket DalalNo ratings yet
- LATIHAN PAS BasinkDocument15 pagesLATIHAN PAS Basinkaajiyu55No ratings yet
- Koopman - For God So Loved The World - Some Contours For Public TheologyDocument18 pagesKoopman - For God So Loved The World - Some Contours For Public TheologyKhegan DelportNo ratings yet
- Buckle - CobraDocument19 pagesBuckle - CobraPeter DavidsonNo ratings yet
- Letter of Recommendation - Josh SethiDocument1 pageLetter of Recommendation - Josh Sethiapi-346224560No ratings yet
- Document 243Document4 pagesDocument 243Abhishank BhardwajNo ratings yet
- Microeconomics 7th Edition Pindyck Test BankDocument38 pagesMicroeconomics 7th Edition Pindyck Test Bankmasonpowellkp28100% (14)
- q3 KuritaDocument3 pagesq3 KuritaMarwa ElsherifNo ratings yet
- 2 Grade Inquiry-Based Lesson South Africa vs. Slaton, TXDocument31 pages2 Grade Inquiry-Based Lesson South Africa vs. Slaton, TXSamantha MelvinNo ratings yet
- Physics Katete Grade 10Document68 pagesPhysics Katete Grade 10joshua witika100% (1)
- Community Nutrition Manual (AutoRecovered)Document77 pagesCommunity Nutrition Manual (AutoRecovered)Reen “Sudi” MuloliNo ratings yet
- Catalogo Plasma ThermadyneDocument4 pagesCatalogo Plasma ThermadynepiterNo ratings yet