You might also like
- Orbital and Ocular TumorsDocument13 pagesOrbital and Ocular TumorsstarlytexpressNo ratings yet
- Pathology Checklist DR Preeti SharmaDocument5 pagesPathology Checklist DR Preeti SharmaAvi Khanna100% (1)
- Balantidium ColiDocument7 pagesBalantidium ColiOmar GhoneimNo ratings yet
- Most ImportantDocument3 pagesMost ImportantVenkata Ramana Murthy Vasupilli100% (1)
- Pharmacotherapy of Urinary Tract InfectionDocument75 pagesPharmacotherapy of Urinary Tract InfectionMariana CreciunNo ratings yet
- FMGE June 2019 questions and answersDocument20 pagesFMGE June 2019 questions and answersSugithaTamilarasanNo ratings yet
- My Cancrum OrisDocument22 pagesMy Cancrum OrisSoyebo Alegría OluseyeNo ratings yet
- Myelodysplastic Syndrome: DR Mika Lumbantobing, Sppd-KhomDocument20 pagesMyelodysplastic Syndrome: DR Mika Lumbantobing, Sppd-KhomsehatkabauNo ratings yet
- Parapneumonic Pleural Effusions and Empyema Thoracis: Causes, Symptoms and TreatmentDocument4 pagesParapneumonic Pleural Effusions and Empyema Thoracis: Causes, Symptoms and TreatmentLorentina Den PanjaitanNo ratings yet
- Cell Injury, Death, and Adaptation: DefinitonsDocument37 pagesCell Injury, Death, and Adaptation: Definitonsyasobaby100% (1)
- Elective Placements Application GuideDocument6 pagesElective Placements Application GuideAshish BamaniaNo ratings yet
- Autoimmune Hemolytic Anemia and ITPDocument3 pagesAutoimmune Hemolytic Anemia and ITPNivya Mary0% (1)
- Nasal Septal Disorders: Dr. Omwenga Cliffe Facilitator: Dr. KipingorDocument45 pagesNasal Septal Disorders: Dr. Omwenga Cliffe Facilitator: Dr. KipingorjustofitsNo ratings yet
- 2014 - Lecture - Pathology of The Small and Large IntestineDocument12 pages2014 - Lecture - Pathology of The Small and Large IntestinesammysandsongNo ratings yet
- Aakash Neet PG NotesDocument8 pagesAakash Neet PG NotesAravindh Balaji SNo ratings yet
- Acute Kidney Injury: Causes and DiagnosisDocument37 pagesAcute Kidney Injury: Causes and DiagnosisEndah Risky GustiyantiNo ratings yet
- SpermatoceleDocument2 pagesSpermatocelemrizkidm2301No ratings yet
- Paediatric Q & ADocument47 pagesPaediatric Q & AHafizuddin RazidNo ratings yet
- Strategy For Mci Screening TestDocument3 pagesStrategy For Mci Screening TestDr.G.Bhanu PrakashNo ratings yet
- Membranous Nephropathy: From Models To Man: Review SeriesDocument8 pagesMembranous Nephropathy: From Models To Man: Review SeriesmmsNo ratings yet
- Curriculum-Vitae Abhimanyu NehraDocument3 pagesCurriculum-Vitae Abhimanyu NehraVedita Dhull100% (1)
- Blastomycosis: Narendra Shanmugam Group 22Document17 pagesBlastomycosis: Narendra Shanmugam Group 22Naren ShanNo ratings yet
- (Practical Exam) Back Row NotesDocument16 pages(Practical Exam) Back Row NotesKeesha RiveraNo ratings yet
- Adequacy Criteria: ExceptionsDocument3 pagesAdequacy Criteria: ExceptionsPranayNo ratings yet
- DR - Polaris 4th Year Flash NoteDocument77 pagesDR - Polaris 4th Year Flash Notethat savage guyNo ratings yet
- The Most CommonsDocument80 pagesThe Most CommonsJmee8No ratings yet
- Rare Case of Peutz-Jeghers SyndromeDocument4 pagesRare Case of Peutz-Jeghers Syndromesaikrishnamedico100% (1)
- Acute appendicitis inflammatory mediator quizDocument10 pagesAcute appendicitis inflammatory mediator quizsleepingdirtyNo ratings yet
- Rapid Review AIPGMEE, 2011Document44 pagesRapid Review AIPGMEE, 2011basic80% (5)
- CellulitisDocument18 pagesCellulitisHandrian Rahman100% (1)
- DAMS CRS - Obstetrics & Gynaecology (DAMS Comprehensive Review Series) - DAMSDocument36 pagesDAMS CRS - Obstetrics & Gynaecology (DAMS Comprehensive Review Series) - DAMSAbhisek ChatterjeeNo ratings yet
- Medical waste mnemonicDocument3 pagesMedical waste mnemonicRahul All100% (1)
- Laser Treatment For GlaucomaDocument52 pagesLaser Treatment For GlaucomadrquanNo ratings yet
- Pathology of Parathyrid Gland FinalDocument63 pagesPathology of Parathyrid Gland FinalGurpreet Kaur SagooNo ratings yet
- Lipoma ExcisionDocument4 pagesLipoma ExcisionNikolaus TalloNo ratings yet
- Anti - EpilepticsDocument27 pagesAnti - EpilepticsVijayabala JeevaganNo ratings yet
- HX Taking of PeadiatricsDocument5 pagesHX Taking of PeadiatricsCahaya Al-Hazeenillah100% (1)
- Introduction To Pathology Infectious DiseasesDocument37 pagesIntroduction To Pathology Infectious DiseasesNirav PatelNo ratings yet
- Diseases of The Parathyroid GlandDocument60 pagesDiseases of The Parathyroid GlandRuDy RaviNo ratings yet
- Surgery 92Document92 pagesSurgery 92Sai Pardhu33% (3)
- 500 SBA Gen SystemicDocument27 pages500 SBA Gen Systemicdr_shafiqNo ratings yet
- 300 Fcps Mcq's SolvedDocument16 pages300 Fcps Mcq's SolvedFarazNo ratings yet
- Mbbs BooksDocument7 pagesMbbs Booksbakhem7hbk2002190% (1)
- MenorrhagiaDocument4 pagesMenorrhagiaFlloyd_Martin__1259No ratings yet
- UHS PBL - Febrile Child: Case Scenario 1Document4 pagesUHS PBL - Febrile Child: Case Scenario 1Natosha MendozaNo ratings yet
- Visual Mnemonics For BoardsDocument39 pagesVisual Mnemonics For BoardsyepherenowNo ratings yet
- Retinopathy stagingDocument4 pagesRetinopathy stagingNikithaNo ratings yet
- Collodion Baby: Presented byDocument10 pagesCollodion Baby: Presented byNoor AhamedNo ratings yet
- Ophthalmology Pictures For MRCP Part-2 WrittenDocument96 pagesOphthalmology Pictures For MRCP Part-2 WrittenLeilaNo ratings yet
- Check Unit 555 November Immunology V3 PDFDocument25 pagesCheck Unit 555 November Immunology V3 PDFdragon66No ratings yet
- IM - Facts From Case Files CRCDocument80 pagesIM - Facts From Case Files CRCridin007No ratings yet
- Orthopedics Images Based QuestionsDocument29 pagesOrthopedics Images Based QuestionsKannan KannanNo ratings yet
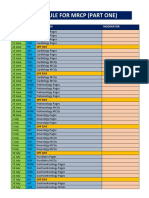
- Schedule For MRCP (Part One) PDFDocument3 pagesSchedule For MRCP (Part One) PDFImran ChaudhryNo ratings yet
- Red Eye Poster HiresDocument1 pageRed Eye Poster HiresAndrew CheongNo ratings yet
- Community OphthalmologyDocument23 pagesCommunity OphthalmologyOphthalmology DiscussionNo ratings yet
- Bleeding Disorder (Paediatrics)Document95 pagesBleeding Disorder (Paediatrics)Nurul Afiqah Mohd YusoffNo ratings yet
- 14 - UveitisDocument4 pages14 - UveitisSpislgal PhilipNo ratings yet
- 2010 Schwartz's Principles of SurgeryDocument4 pages2010 Schwartz's Principles of SurgeryPJHG50% (2)
- Inflammatory Disorders of The Eyelids: BlepharitisDocument3 pagesInflammatory Disorders of The Eyelids: BlepharitisNadia Indah AlvitaNo ratings yet
- Diskusi Topik BlepharitisDocument10 pagesDiskusi Topik BlepharitisDwi Permana PutraNo ratings yet
- 02 Impact of COVID-19 Outbreak On The Emergency of Acute AppendicitisDocument5 pages02 Impact of COVID-19 Outbreak On The Emergency of Acute AppendicitishiNo ratings yet
- A Special Case of Lower Back Pain in A 3-Year-Old Girl: Davide Tassinari, Sara Forti, Michele Torella, Giovanni TaniDocument7 pagesA Special Case of Lower Back Pain in A 3-Year-Old Girl: Davide Tassinari, Sara Forti, Michele Torella, Giovanni TanihiNo ratings yet
- Asian Spine Risk FactorsDocument8 pagesAsian Spine Risk FactorsSahithya MNo ratings yet
- Treating Stye, Chalazion and TrichiasisDocument4 pagesTreating Stye, Chalazion and TrichiasishiNo ratings yet
- Aquatic Exercise and Pain Neurophysiology Education Versus Aquatic Exercise Alone For Patients With LBP Chronics1Document10 pagesAquatic Exercise and Pain Neurophysiology Education Versus Aquatic Exercise Alone For Patients With LBP Chronics1hiNo ratings yet
- 03 Increasing Incidence of Complicated Appendicitis During COVID-19Document5 pages03 Increasing Incidence of Complicated Appendicitis During COVID-19hiNo ratings yet
- 04 Managing Acute Appendicitis During The COVID-19 Pandemic in Jiaxing, ChinaDocument12 pages04 Managing Acute Appendicitis During The COVID-19 Pandemic in Jiaxing, ChinahiNo ratings yet
- 01 Impact of The COVID-19 Pandemic On Appendicitis TreatmentDocument7 pages01 Impact of The COVID-19 Pandemic On Appendicitis TreatmenthiNo ratings yet
- Apendisitis HarisonDocument5 pagesApendisitis HarisonhiNo ratings yet
- New Doc 2019-02-21 15.31.31 - 20190221161639602Document44 pagesNew Doc 2019-02-21 15.31.31 - 20190221161639602hiNo ratings yet
- Akbayrak2019 (CR)Document4 pagesAkbayrak2019 (CR)hiNo ratings yet
- Assessment of LymphadenopathyDocument69 pagesAssessment of LymphadenopathyhiNo ratings yet
- Dieulafoy's LesionDocument2 pagesDieulafoy's LesionhiNo ratings yet
- Bleedng GIT HarrisonDocument4 pagesBleedng GIT HarrisonhiNo ratings yet
- New Doc 2020-03-30 13.39.44 - 20200330140201Document5 pagesNew Doc 2020-03-30 13.39.44 - 20200330140201hiNo ratings yet
- COVID-19 Infection in Pregnant Women: Review of Maternal and Fetal OutcomesDocument8 pagesCOVID-19 Infection in Pregnant Women: Review of Maternal and Fetal Outcomesumbu anandaNo ratings yet
- Scanned With CamscannerDocument5 pagesScanned With CamscannerhiNo ratings yet
- Non-Invasive Brain Stimulation For Gambling Disorder A Systematic ReviewDocument11 pagesNon-Invasive Brain Stimulation For Gambling Disorder A Systematic ReviewhiNo ratings yet
- Stimulasi Otak Non-Invasif Untuk Gangguan Judi - Tinjauan SistematisDocument21 pagesStimulasi Otak Non-Invasif Untuk Gangguan Judi - Tinjauan SistematishiNo ratings yet
- Repetitive Transcranial Magnetic Stimulation in Gambling Disorder - Full Text View - ClinicalTrials - GovDocument1 pageRepetitive Transcranial Magnetic Stimulation in Gambling Disorder - Full Text View - ClinicalTrials - GovhiNo ratings yet
- Transport of Critically Ill: Himanshu Khurana, Yatin MehtaDocument9 pagesTransport of Critically Ill: Himanshu Khurana, Yatin MehtahiNo ratings yet
- Bab 8 EngDocument25 pagesBab 8 EnghiNo ratings yet
- Atrioventricular Nodal Reentrant Tachycardia: AvnrtDocument13 pagesAtrioventricular Nodal Reentrant Tachycardia: AvnrthiNo ratings yet
- Screenshot 2021-01-12 at 16.57.57Document36 pagesScreenshot 2021-01-12 at 16.57.57hiNo ratings yet
- Two Case Reports of Acute Upper Gastrointestinal BleedingDocument9 pagesTwo Case Reports of Acute Upper Gastrointestinal BleedinghiNo ratings yet
- Edit - RESPIRATORY DIVINGDocument30 pagesEdit - RESPIRATORY DIVINGhiNo ratings yet
- Neocortical DynamicDocument16 pagesNeocortical DynamichiNo ratings yet
- Julia SlidesManiaDocument17 pagesJulia SlidesManiahiNo ratings yet
- High School Weekly Planner: - MinimalistDocument48 pagesHigh School Weekly Planner: - Minimalistjetlee estacion100% (1)
- A Plasmid Is A Small DNA Molecule Within A Cell That Is Physically Separated From A Chromosomal DNA and Can Replicate IndependentlyDocument5 pagesA Plasmid Is A Small DNA Molecule Within A Cell That Is Physically Separated From A Chromosomal DNA and Can Replicate Independentlyyaqoob008No ratings yet
- 1.urogen Well D-One Eng. Rev. 6Document9 pages1.urogen Well D-One Eng. Rev. 6nmakrygNo ratings yet
- OBGYN 1st Round 2021 AnsweredDocument14 pagesOBGYN 1st Round 2021 AnsweredMuhammed Mostafa100% (4)
- Pernicious Oral Habits-1 PDFDocument35 pagesPernicious Oral Habits-1 PDFWen Shu GohNo ratings yet
- Cardiovascular Exam GuideDocument4 pagesCardiovascular Exam GuidearchanaNo ratings yet
- Yoga For PregnancyDocument9 pagesYoga For Pregnancyspes123100% (1)
- Immunological DisordersDocument78 pagesImmunological DisordersAshwathy ThomasNo ratings yet
- Care For The Patient With Limited Mobility: Problems Caused by Prolonged ImmobilityDocument18 pagesCare For The Patient With Limited Mobility: Problems Caused by Prolonged ImmobilityFerdaooz Azhar Al-MootNo ratings yet
- Why SufferingDocument7 pagesWhy SufferingRandall Dean WestNo ratings yet
- Oral and Maxillofacial PathologyDocument79 pagesOral and Maxillofacial PathologyMai AnhNo ratings yet
- Self Care Handout-1Document3 pagesSelf Care Handout-1Wandarh RhNo ratings yet
- Red Flags ArticleDocument4 pagesRed Flags ArticleINNOCENT KHULIWANo ratings yet
- Tetanus Symptoms, Causes, Treatment and PreventionDocument4 pagesTetanus Symptoms, Causes, Treatment and PreventionSneha SnehaNo ratings yet
- Blood SamplingDocument11 pagesBlood Samplingwiodi nazhofatunnisa umami swNo ratings yet
- Pulmonary Rehabilitation (S)Document79 pagesPulmonary Rehabilitation (S)liz100% (3)
- NCM 109 (ECG and Cardiac Monitoring)Document7 pagesNCM 109 (ECG and Cardiac Monitoring)Kyla BungayNo ratings yet
- Umbilical Cord CareDocument3 pagesUmbilical Cord CareHui Li TehNo ratings yet
- Granuloma TuberculosisDocument9 pagesGranuloma TuberculosisÁlvaro Alexandro Morales JiménezNo ratings yet
- Sexual Orientation and Gender IdentityDocument24 pagesSexual Orientation and Gender IdentityBreajAdarbe100% (1)
- Caie As Level Geography 9696 Core Human Geography v1Document13 pagesCaie As Level Geography 9696 Core Human Geography v1BrizzyNo ratings yet
- Chest Pneumonia Detection From X-Ray Images Using Resnet101 ModelDocument19 pagesChest Pneumonia Detection From X-Ray Images Using Resnet101 ModelMahesh TekiNo ratings yet
- Workshop1 1Document2 pagesWorkshop1 1Aple Mae Cudiamat Letranca-CastroNo ratings yet
- GallstonesDocument17 pagesGallstonesع ب و دNo ratings yet
- Assignment 3Document5 pagesAssignment 3Samantha PargadNo ratings yet
- Electro PDFDocument14 pagesElectro PDFFulg de NeaNo ratings yet
- Growel Dairy Farming ManualDocument52 pagesGrowel Dairy Farming ManualGrowel Agrovet Private Limited.No ratings yet
- Final Molecular BiologyDocument8 pagesFinal Molecular Biologyrachyb7100% (1)
- Health and Privacy PDFDocument40 pagesHealth and Privacy PDFMonika NegiNo ratings yet
- WHO - Adherence ReportDocument211 pagesWHO - Adherence Reportscratch9100% (1)
- Frcophth 400 Sbas and CrqsDocument262 pagesFrcophth 400 Sbas and CrqsZaheer Ullah Soleh100% (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)