You might also like
- Biophysical Profile PDFDocument1 pageBiophysical Profile PDFmp1757No ratings yet
- Mupirocin Drug StudyDocument1 pageMupirocin Drug StudyArthur Christopher Corpuz0% (1)
- SMI COVID-19 Health Survey Form - RevisedDocument2 pagesSMI COVID-19 Health Survey Form - RevisedJess Rey Q. BaranNo ratings yet
- Health & Safety Check Declaration Form: TemperatureDocument1 pageHealth & Safety Check Declaration Form: TemperatureChy GomezNo ratings yet
- RFDGCDC Health and Safety Declaration FormDocument1 pageRFDGCDC Health and Safety Declaration FormChy GomezNo ratings yet
- HD - Reception SantierraDocument1 pageHD - Reception SantierraAnezka Danett CortinaNo ratings yet
- TD Enterprise Health Screening Form enDocument2 pagesTD Enterprise Health Screening Form enKevin JayNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormNaldrin RosalesNo ratings yet
- Term 3 COVID 19 Student Declaration FormDocument1 pageTerm 3 COVID 19 Student Declaration FormProxyNo ratings yet
- COVID-19: Client & Employee Screening QuestionnaireDocument2 pagesCOVID-19: Client & Employee Screening QuestionnaireAlyssa MirabellaNo ratings yet
- House of Representatives: Republic of The Philippines Quezon City, Metro ManilaDocument3 pagesHouse of Representatives: Republic of The Philippines Quezon City, Metro ManilamereeNo ratings yet
- Daily Health Screening Checklist - COVID19 (For Visitors) : TemperatureDocument2 pagesDaily Health Screening Checklist - COVID19 (For Visitors) : TemperatureHelen GamboaNo ratings yet
- Bangsamoro Transition Authority: Reminders For Physical AttendeesDocument2 pagesBangsamoro Transition Authority: Reminders For Physical AttendeesShob SinsuatNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormJohnna Pauline VirayNo ratings yet
- Self Declaration - Covid 19 Pre Screening: SL No Check Points AnswerDocument1 pageSelf Declaration - Covid 19 Pre Screening: SL No Check Points AnswerPampanagouda YadavNo ratings yet
- Don Bosco Tvet Center-Calauan, Inc.: Km. 77, Brgy, Dayap, Calauan, Laguna. 4012Document2 pagesDon Bosco Tvet Center-Calauan, Inc.: Km. 77, Brgy, Dayap, Calauan, Laguna. 4012Johnlester Delacruz KoaNo ratings yet
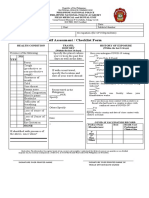
- Self Assessment / Checklist FormDocument1 pageSelf Assessment / Checklist FormAiza Rhea SantosNo ratings yet
- SPAS Customer Health Checklist Form A4Document1 pageSPAS Customer Health Checklist Form A4kablasNo ratings yet
- CHECKLIST FOR PERSONS UNDER MONITORING (For BHERT Use Only) Re 2019 nCoV ARDDocument1 pageCHECKLIST FOR PERSONS UNDER MONITORING (For BHERT Use Only) Re 2019 nCoV ARDCHICKYNo ratings yet
- Self Assessment / Checklist Form: YES NODocument1 pageSelf Assessment / Checklist Form: YES NOdoie kimNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormRoseller SasisNo ratings yet
- Quarantine Form 1Document1 pageQuarantine Form 1Rachel AndesNo ratings yet
- Fillable PDA COVID Form and Informed ConsentDocument1 pageFillable PDA COVID Form and Informed ConsentShane Marie ClitarNo ratings yet
- Board Exam Oct 2Document12 pagesBoard Exam Oct 2Aljee Sumampong BationNo ratings yet
- COVID-19 Screening Tool For Public Health and Health Links-Info SantéDocument27 pagesCOVID-19 Screening Tool For Public Health and Health Links-Info SantéTsania KusumawardaniNo ratings yet
- PX COVIDsurveyDocument1 pagePX COVIDsurveyEuniceNo ratings yet
- Health Declaration CardDocument2 pagesHealth Declaration CardJasmin AngieNo ratings yet
- COVID-19 Screening Questionnaire - Ed3Document1 pageCOVID-19 Screening Questionnaire - Ed3GilbertNo ratings yet
- Health Declaration Form1Document2 pagesHealth Declaration Form1JULCON ARAIZNo ratings yet
- Daily Health RecordDocument1 pageDaily Health RecordargelNo ratings yet
- Health Checklist: Tuguegarao Archdiocesan School System Our Lady of Piat High SchoolDocument3 pagesHealth Checklist: Tuguegarao Archdiocesan School System Our Lady of Piat High SchoolLourd Juan Artuz MustafaNo ratings yet
- Preliminary Checklist - Covid 19 - MolmiDocument2 pagesPreliminary Checklist - Covid 19 - MolmiRohit PatelNo ratings yet
- Declaration Declaration Declaration: Signature DateDocument2 pagesDeclaration Declaration Declaration: Signature DateQuinric Bontilao SevillejoNo ratings yet
- Ba Go Health Declaration FormDocument1 pageBa Go Health Declaration FormPoblacion, Brien S.No ratings yet
- Visitors Health Checklist Form (From DTI and DOLE)Document1 pageVisitors Health Checklist Form (From DTI and DOLE)melbaNo ratings yet
- Covid-19 Impact Hrqol Questionnaire FinalDocument3 pagesCovid-19 Impact Hrqol Questionnaire FinalJosh LozadaNo ratings yet
- Declaration Declaration Declaration: Signature DateDocument2 pagesDeclaration Declaration Declaration: Signature DateRamir BecoyNo ratings yet
- Health Checklist Health Checklist Temperature: TemperatureDocument2 pagesHealth Checklist Health Checklist Temperature: TemperatureJeniffer FajardoNo ratings yet
- COVID-19 Self-Declaration Form - Atul ValsadDocument2 pagesCOVID-19 Self-Declaration Form - Atul Valsad8460272421No ratings yet
- Self Assesment Form MARS3 02092020Document1 pageSelf Assesment Form MARS3 02092020Randi NababanNo ratings yet
- Health Declaration Form - 1606903543Document1 pageHealth Declaration Form - 1606903543Patrick GregorioNo ratings yet
- Health & Safety Declaration FormDocument7 pagesHealth & Safety Declaration FormMelissa DavidNo ratings yet
- CDC COVID QuestionnaireDocument2 pagesCDC COVID QuestionnaireKenneth A. Prado M.No ratings yet
- House of Representatives: Republic of The PhilippinesDocument2 pagesHouse of Representatives: Republic of The PhilippinesAlvin CerezoNo ratings yet
- Tanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormDocument4 pagesTanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormKurt VillaNo ratings yet
- COVID-19 Questionnaire Rev.7 (2020-11-13)Document1 pageCOVID-19 Questionnaire Rev.7 (2020-11-13)Satendra kumarNo ratings yet
- Health Declaration Slip: (For Contact Tracing)Document2 pagesHealth Declaration Slip: (For Contact Tracing)Aylene GersanibNo ratings yet
- Health Declaration Health Declaration: YES NO YES NODocument1 pageHealth Declaration Health Declaration: YES NO YES NOMagnificat filesNo ratings yet
- Img 20200716 0001Document1 pageImg 20200716 0001mark sylNo ratings yet
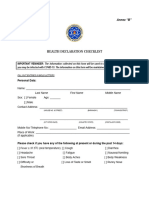
- Health Declaration Checklist Health Declaration Checklist: Last Name First Name Middle Name Middle NameDocument3 pagesHealth Declaration Checklist Health Declaration Checklist: Last Name First Name Middle Name Middle NameJason PaquibulanNo ratings yet
- SLMC Health Declaration FormDocument1 pageSLMC Health Declaration FormNikkiNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAzri AzizNo ratings yet
- Self Declaration For Covid 19 1st PageDocument1 pageSelf Declaration For Covid 19 1st PagedfjasdhgfjkasdgsNo ratings yet
- Checklist For Persons Under Monitoring (PUM) : Eastern VisayasDocument1 pageChecklist For Persons Under Monitoring (PUM) : Eastern VisayasSophie Rose V R-zNo ratings yet
- Consent Form Covid 19Document1 pageConsent Form Covid 19Mahesh with UshaNo ratings yet
- 2020-68 Annex B - Health Declaration Form110320Document3 pages2020-68 Annex B - Health Declaration Form110320Jay MonrealNo ratings yet
- Health Declaration ChecklistDocument3 pagesHealth Declaration ChecklistChe CacatianNo ratings yet
- 2020-68 Annex B - Health Declaration Form110320Document3 pages2020-68 Annex B - Health Declaration Form110320tdci.franceskorineganzaNo ratings yet
- Health Assessment Form For Student 02Document2 pagesHealth Assessment Form For Student 02ERICA MAY LABOGNo ratings yet
- Covid Self Declaration Form Visitor PDFDocument3 pagesCovid Self Declaration Form Visitor PDFTipu BabuNo ratings yet
- Pharmacologic: Systemic Administration AssessmentDocument3 pagesPharmacologic: Systemic Administration Assessmentitsmeaya100% (1)
- Principles of Seizure ManagementDocument119 pagesPrinciples of Seizure ManagementRenan Toledo SandaloNo ratings yet
- Troublesome Throat Awareness (tTA) As A Contemporary Alternative To 'Globus Pharyngeus (DOODY 2017)Document3 pagesTroublesome Throat Awareness (tTA) As A Contemporary Alternative To 'Globus Pharyngeus (DOODY 2017)DANDYNo ratings yet
- 407-Article Text-1424-3-10-20210802 PDFDocument8 pages407-Article Text-1424-3-10-20210802 PDFWahyuni. ambarwatiNo ratings yet
- Articles: BackgroundDocument10 pagesArticles: BackgroundivanlchNo ratings yet
- 23-08-2021 Handwritten NotesDocument13 pages23-08-2021 Handwritten NotesAbhishekh GuptaNo ratings yet
- Malaria Infection in Children Below 10 Years Attending Doka Rural HospitalDocument9 pagesMalaria Infection in Children Below 10 Years Attending Doka Rural HospitalKIU PUBLICATION AND EXTENSIONNo ratings yet
- Herbal Medicine For EveryoneDocument63 pagesHerbal Medicine For EveryoneMaratus Solehah100% (2)
- Ypgh 113 1695081Document12 pagesYpgh 113 1695081Pawan MishraNo ratings yet
- Diff Betw Cohort N Case ControlDocument1 pageDiff Betw Cohort N Case ControlFirzuan WanNo ratings yet
- The Domain BacteriaDocument51 pagesThe Domain BacterialeyluuuuuhNo ratings yet
- Complete Notes For Class 12 (Yoga and Lifestyle)Document20 pagesComplete Notes For Class 12 (Yoga and Lifestyle)Om Kumar Singh67% (3)
- LEEP 1000 Workstation Operating Manual 220vDocument24 pagesLEEP 1000 Workstation Operating Manual 220vpatrickNo ratings yet
- CHN LEC 1 Week 5-6Document39 pagesCHN LEC 1 Week 5-6Carl Josef C. GarciaNo ratings yet
- Failed My Nursing DissertationDocument4 pagesFailed My Nursing DissertationPaySomeoneToDoMyPaperCanada100% (1)
- 03-05.PreTesting and Troubleshooting A Washing MachineDocument2 pages03-05.PreTesting and Troubleshooting A Washing MachineRissy Kh Xhie100% (1)
- QN BNK Og PeadDocument39 pagesQN BNK Og PeadZemen addiss100% (3)
- Fish and Shell Fish Immunology: Full Length ArticleDocument9 pagesFish and Shell Fish Immunology: Full Length ArticleKirana Rahmada SafitriNo ratings yet
- Understanding The SelfDocument26 pagesUnderstanding The SelfPaula100% (1)
- USMLE STEP 1 CHECKLIST @lifeinwhitecoatDocument23 pagesUSMLE STEP 1 CHECKLIST @lifeinwhitecoatGlorivy E. Mora Gonzalez100% (3)
- Prenatal and Postnatal Care A Woman Centered Approach 2nd EditionDocument61 pagesPrenatal and Postnatal Care A Woman Centered Approach 2nd Editionmarion.wade943No ratings yet
- Effectiveness of Tens Versus Intermittent CervicalDocument6 pagesEffectiveness of Tens Versus Intermittent CervicalshindyNo ratings yet
- Ministry of Health AND Family Welfare: Major Schemes and ProgrammesDocument166 pagesMinistry of Health AND Family Welfare: Major Schemes and ProgrammesVarun ToshniwalNo ratings yet
- Find Out The Lack of Healthcare Concerns of Mass Populations and The Local Government During The Epidemic in Rural Area: A Study On Basail Upazila, Tangail, BangladeshDocument6 pagesFind Out The Lack of Healthcare Concerns of Mass Populations and The Local Government During The Epidemic in Rural Area: A Study On Basail Upazila, Tangail, BangladeshMuhammad Al AminNo ratings yet
- PRF PeriodontiaDocument8 pagesPRF PeriodontiaDANIELA MARTINS LEITENo ratings yet
- Abebizuhan ZigaleDocument45 pagesAbebizuhan Zigaleabiraham zigaleNo ratings yet
- .Trashed 1703825822 AIIMS NORCET Memory Based Paper Delhi 15 Sept 2019 EnglishDocument161 pages.Trashed 1703825822 AIIMS NORCET Memory Based Paper Delhi 15 Sept 2019 EnglishNanda NandaNo ratings yet
- Enhanced Recovery After Surgery: It's Time To Change Practice!Document12 pagesEnhanced Recovery After Surgery: It's Time To Change Practice!Anditha Namira RSNo ratings yet