You might also like
- Health & Safety Check Declaration Form: TemperatureDocument1 pageHealth & Safety Check Declaration Form: TemperatureChy GomezNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormJo Anth Bernabe BuenaventuraNo ratings yet
- Health & Safety Declaration FormDocument7 pagesHealth & Safety Declaration FormMelissa DavidNo ratings yet
- Declaration - Return To Work Form (Covid 19) : EmployeeDocument2 pagesDeclaration - Return To Work Form (Covid 19) : EmployeeFahad Khalid100% (1)
- Health Declaration Form - A1 Whole Page - ADocument1 pageHealth Declaration Form - A1 Whole Page - ASharme Cagalawan AmahanNo ratings yet
- Declaration Initial IllnessDocument1 pageDeclaration Initial IllnessFahad KhalidNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageJoezerk CarpioNo ratings yet
- Health Form For Civil Service ExamDocument1 pageHealth Form For Civil Service Examralph sabaNo ratings yet
- Health Declaration: YES NODocument1 pageHealth Declaration: YES NOEliezal Dean B. CardeñoNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PagemarieleNo ratings yet
- HDF PDFDocument1 pageHDF PDFJhon Rey GonsalezNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageMiamor NatividadNo ratings yet
- Health Declaration Form A1 Whole PageDocument1 pageHealth Declaration Form A1 Whole PageFedelyn SemenianoNo ratings yet
- Screening FormDocument2 pagesScreening FormMarie I. RosalesNo ratings yet
- Health Declaration Health Declaration: YES NO YES NODocument1 pageHealth Declaration Health Declaration: YES NO YES NOMagnificat filesNo ratings yet
- DLSU Health Screening FormDocument1 pageDLSU Health Screening FormRobert Paul A MorenoNo ratings yet
- Health Declaration Health Declaration: YES NO YES NODocument1 pageHealth Declaration Health Declaration: YES NO YES NOmike tandocNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration Formedward mirandilla miranda jr.No ratings yet
- Creening Test For 'Associates Returning To Work DateDocument1 pageCreening Test For 'Associates Returning To Work Datejohn ralph silvaNo ratings yet
- SLMC Health Declaration FormDocument1 pageSLMC Health Declaration FormNikkiNo ratings yet
- Crew Health Self-Declaration and Daily Temperature Record - Global - Onsigner Version OCT2020Document2 pagesCrew Health Self-Declaration and Daily Temperature Record - Global - Onsigner Version OCT2020Knowrain ParasNo ratings yet
- House of Representatives: Republic of The Philippines Quezon City, Metro ManilaDocument3 pagesHouse of Representatives: Republic of The Philippines Quezon City, Metro ManilamereeNo ratings yet
- COVID-19 Screening Tool For Long-Term Care Homes and Retirement HomesDocument3 pagesCOVID-19 Screening Tool For Long-Term Care Homes and Retirement HomesGuillermo Rodriguez LopezNo ratings yet
- Tick/circle The Appropriate Answers For All ListedDocument1 pageTick/circle The Appropriate Answers For All ListedRiya SinglaNo ratings yet
- Health ChecklistDocument1 pageHealth ChecklistU N K O W N U N k o w nNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormVeralynNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormNaldrin RosalesNo ratings yet
- Health Declaration Form: Borang Pengisytiharan KesihatanDocument1 pageHealth Declaration Form: Borang Pengisytiharan KesihatanmarryvessaNo ratings yet
- 5.intertanko Health DeclarationDocument1 page5.intertanko Health DeclarationJohanna Catalan CantonesNo ratings yet
- House of Representatives: Republic of The PhilippinesDocument2 pagesHouse of Representatives: Republic of The PhilippinesAlvin CerezoNo ratings yet
- Health Checklist Health Checklist Temperature: TemperatureDocument2 pagesHealth Checklist Health Checklist Temperature: TemperatureJeniffer FajardoNo ratings yet
- Health and Travel History Declaration FormDocument1 pageHealth and Travel History Declaration Formvenus kay faderogNo ratings yet
- Self Declaration - Covid 19 Pre Screening: SL No Check Points AnswerDocument1 pageSelf Declaration - Covid 19 Pre Screening: SL No Check Points AnswerPampanagouda YadavNo ratings yet
- Health and Travel History Declaration Form PDFDocument1 pageHealth and Travel History Declaration Form PDFMeriel Ocbian100% (1)
- Health and Travel History Declaration Form: Please Check OneDocument1 pageHealth and Travel History Declaration Form: Please Check Onepaolo ledesmaNo ratings yet
- Health Declaration Form: Borang Pengisytiharan KesihatanDocument1 pageHealth Declaration Form: Borang Pengisytiharan Kesihatanhasan mamatNo ratings yet
- Visitors Health Checklist Form (From DTI and DOLE)Document1 pageVisitors Health Checklist Form (From DTI and DOLE)melbaNo ratings yet
- Bangsamoro Transition Authority: Reminders For Physical AttendeesDocument2 pagesBangsamoro Transition Authority: Reminders For Physical AttendeesShob SinsuatNo ratings yet
- Covid Self Declaration Form Visitor PDFDocument3 pagesCovid Self Declaration Form Visitor PDFTipu BabuNo ratings yet
- Covid 19 QuestionnaireDocument2 pagesCovid 19 QuestionnaireChristine De Villa-RagudoNo ratings yet
- COVID-19 Health Declaration Form (Rev. 4)Document2 pagesCOVID-19 Health Declaration Form (Rev. 4)ammar razaNo ratings yet
- COVID-19 Self-Declaration Form - Atul ValsadDocument2 pagesCOVID-19 Self-Declaration Form - Atul Valsad8460272421No ratings yet
- BHHP 7-9 PDFDocument1 pageBHHP 7-9 PDFSiti MasturaNo ratings yet
- Health Declaration FormDocument4 pagesHealth Declaration FormDOMINIC HAWANGNo ratings yet
- COVID-19 Screening Tool For Long-Term Care Homes and Retirement HomesDocument3 pagesCOVID-19 Screening Tool For Long-Term Care Homes and Retirement HomesSureshNo ratings yet
- Health Declaration Form: Client Name: Email Add: Address: Date: Mobile Number: Nail TechDocument1 pageHealth Declaration Form: Client Name: Email Add: Address: Date: Mobile Number: Nail Techcindya jorduelaNo ratings yet
- Self Declaration For Covid 19 1st PageDocument1 pageSelf Declaration For Covid 19 1st PagedfjasdhgfjkasdgsNo ratings yet
- COVID QuestionnaireDocument2 pagesCOVID QuestionnaireВасил НачевNo ratings yet
- Tanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormDocument4 pagesTanauan City Integrated High School Trapiche 1, Tanauan City, Batangas Health Declaration FormKurt VillaNo ratings yet
- 2 - HEALTH DECLARATION FORM For New Hire 05292020 KTDocument1 page2 - HEALTH DECLARATION FORM For New Hire 05292020 KTpam01pamNo ratings yet
- Health Checklist: Tuguegarao Archdiocesan School System Our Lady of Piat High SchoolDocument3 pagesHealth Checklist: Tuguegarao Archdiocesan School System Our Lady of Piat High SchoolLourd Juan Artuz MustafaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAlexander IgasanNo ratings yet
- HD - Reception SantierraDocument1 pageHD - Reception SantierraAnezka Danett CortinaNo ratings yet
- Borang Pengisytiharan Kesihatan: Health Declaration FormDocument1 pageBorang Pengisytiharan Kesihatan: Health Declaration FormadibaNo ratings yet
- Parents' and Children's Health Declaration - UpdatedDocument2 pagesParents' and Children's Health Declaration - UpdatedEkin QinNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormJANET ILLESESNo ratings yet
- COVID-19: Staff Screening QuestionnaireDocument2 pagesCOVID-19: Staff Screening QuestionnaireselsilyaNo ratings yet
- Health Declaration Form - 1606903543Document1 pageHealth Declaration Form - 1606903543Patrick GregorioNo ratings yet
- Who Knew Life Could Be This Good: Your Personality Is the Secret to a Happier and Healthier Life.From EverandWho Knew Life Could Be This Good: Your Personality Is the Secret to a Happier and Healthier Life.No ratings yet
- Staff HouseDocument6 pagesStaff HouseChy GomezNo ratings yet
- Schedule of LoadsDocument1 pageSchedule of LoadsChy GomezNo ratings yet
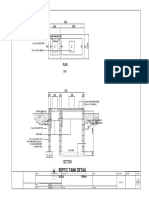
- Septic Tank Detail: Scale 1:20mmDocument1 pageSeptic Tank Detail: Scale 1:20mmChy GomezNo ratings yet
- Electrical Specifications:: Riser DiagramDocument1 pageElectrical Specifications:: Riser DiagramChy GomezNo ratings yet
- Typical Slab 2 Detail: Scale 1:40mmDocument1 pageTypical Slab 2 Detail: Scale 1:40mmChy GomezNo ratings yet
- Fascia Frame Detail: Proposed Single Storey Residential BuildingDocument1 pageFascia Frame Detail: Proposed Single Storey Residential BuildingChy GomezNo ratings yet
- Title PAGE FPWDocument1 pageTitle PAGE FPWChy GomezNo ratings yet
- Proposed Single Storey Residential Building: Ar. Rodel S. Falcasantos, MpaDocument1 pageProposed Single Storey Residential Building: Ar. Rodel S. Falcasantos, MpaChy GomezNo ratings yet
- Catch Basin DetailDocument1 pageCatch Basin DetailChy GomezNo ratings yet
- Schedules of Windows and DoorsDocument1 pageSchedules of Windows and DoorsChy GomezNo ratings yet
- Isometric View PlumbingDocument1 pageIsometric View PlumbingChy GomezNo ratings yet
- Sample CAD For ARCH Floor PlanDocument1 pageSample CAD For ARCH Floor PlanChy GomezNo ratings yet
- Isometric View WaterlineDocument1 pageIsometric View WaterlineChy GomezNo ratings yet
- Stair Plan Detail: Second FloorDocument1 pageStair Plan Detail: Second FloorChy GomezNo ratings yet
- Sample CAD For ARCH Floor Plan 1Document1 pageSample CAD For ARCH Floor Plan 1Chy GomezNo ratings yet
- Sample CAD For ARCH Floor Plan With RoofdeckDocument1 pageSample CAD For ARCH Floor Plan With RoofdeckChy GomezNo ratings yet
- Sample of Architectural PlanDocument1 pageSample of Architectural PlanChy GomezNo ratings yet
- Sample Cad Location PlanDocument1 pageSample Cad Location PlanChy GomezNo ratings yet
- Isometric View: Name NameDocument1 pageIsometric View: Name NameChy GomezNo ratings yet
- Sample CAD For Architetural DrawingsDocument1 pageSample CAD For Architetural DrawingsChy GomezNo ratings yet
- Sample CAD For ARCH Floor Plan With RoofdeckDocument1 pageSample CAD For ARCH Floor Plan With RoofdeckChy GomezNo ratings yet
- Sample Cad Location PlanDocument1 pageSample Cad Location PlanChy GomezNo ratings yet
- Sample of ELEVATION PLANDocument1 pageSample of ELEVATION PLANChy GomezNo ratings yet
- Mixed Used Passenger Terminal Buildin1 Final-1Document9 pagesMixed Used Passenger Terminal Buildin1 Final-1Chy GomezNo ratings yet
- The Cross-Price Elasticity of Demand: Econ 101Document4 pagesThe Cross-Price Elasticity of Demand: Econ 101Chy GomezNo ratings yet
- newEIA 1Document9 pagesnewEIA 1Chy GomezNo ratings yet
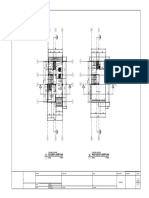
- Ground Floor ResidentialDocument1 pageGround Floor ResidentialChy GomezNo ratings yet
- 2nd Floor ResidentialDocument1 page2nd Floor ResidentialChy GomezNo ratings yet
- About Me: Iris Chyiane Mae L. PaculanangDocument1 pageAbout Me: Iris Chyiane Mae L. PaculanangChy GomezNo ratings yet
- The Cross-Price Elasticity of Demand: Econ 101Document4 pagesThe Cross-Price Elasticity of Demand: Econ 101Chy GomezNo ratings yet
- Group 4 Case Presentation DiarrheaDocument46 pagesGroup 4 Case Presentation DiarrheaEphraim John QuichoNo ratings yet
- Order of Duties of Ophthalmic Assitants Under NPCB&VIDocument3 pagesOrder of Duties of Ophthalmic Assitants Under NPCB&VISathishNo ratings yet
- Oxygen Toxicity - Signs and SymptomsDocument4 pagesOxygen Toxicity - Signs and SymptomsYoga SemadhiNo ratings yet
- Conginital Heart DiseaseDocument19 pagesConginital Heart DiseaseSanthosh.S.UNo ratings yet
- Prevention of Surgical Site Infections: Pola Brenner, Patricio NercellesDocument10 pagesPrevention of Surgical Site Infections: Pola Brenner, Patricio NercellesAmeng GosimNo ratings yet
- Chronic Kidney Disease (CKD) and DiabetesDocument35 pagesChronic Kidney Disease (CKD) and Diabetesm29hereNo ratings yet
- 1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingDocument14 pages1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingKamx Mohammed100% (1)
- CopdDocument60 pagesCopdRizqy Shofianingrum100% (1)
- APA Guidelines On The Prevention of Postoperative Vomiting in ChildrenDocument35 pagesAPA Guidelines On The Prevention of Postoperative Vomiting in ChildrenMaria Lucia RossiNo ratings yet
- Osteomielitis Akut Edit MeiDocument9 pagesOsteomielitis Akut Edit MeiRaja DarmawanNo ratings yet
- Laporan RPUDocument9 pagesLaporan RPUddeeppeeNo ratings yet
- Name: Maulana Aditya Pratama Number: 18029Document8 pagesName: Maulana Aditya Pratama Number: 18029Widiya BudiNo ratings yet
- Diane Kazer Loving On Our LymphDocument22 pagesDiane Kazer Loving On Our LymphKátia BárbaraNo ratings yet
- Part B - Health Facility Briefing & Design 55Document15 pagesPart B - Health Facility Briefing & Design 55Mudita PiseNo ratings yet
- Bmi Lab Viva QuestionDocument7 pagesBmi Lab Viva QuestionnijafancyNo ratings yet
- 823 2334 1 PBDocument7 pages823 2334 1 PBMeryNo ratings yet
- Presented By:dr - Anita Chaudhari Roll No: 2Document22 pagesPresented By:dr - Anita Chaudhari Roll No: 2younismushtaq100% (1)
- Nursing Hyperthyroidism Study GuideDocument4 pagesNursing Hyperthyroidism Study GuideLin SookdeeNo ratings yet
- Basic PhotographyDocument3 pagesBasic Photographyapi-461238862No ratings yet
- NCM 104 IG Lec - DOC CARLDocument23 pagesNCM 104 IG Lec - DOC CARLLanz LlnsNo ratings yet
- World Sight Day-Activity Report - 2022-PICO PakistanDocument5 pagesWorld Sight Day-Activity Report - 2022-PICO Pakistanjibran khanNo ratings yet
- CS - UTI, Acute Bronchitis, Acute GastritisDocument39 pagesCS - UTI, Acute Bronchitis, Acute GastritisGrace BernadetteNo ratings yet
- Kim Resume PDFDocument1 pageKim Resume PDFapi-548816548No ratings yet
- Medication - Chart ADHD PDFDocument2 pagesMedication - Chart ADHD PDFaayceeNo ratings yet
- Medicaid Family TherapyDocument685 pagesMedicaid Family TherapyfejjinsNo ratings yet
- Your Guide To Post Surgery Care - Major - CleanDocument28 pagesYour Guide To Post Surgery Care - Major - CleanZar Chi LinNo ratings yet
- Crocus Sativus L. (Saffron) in The Treatment of Premenstrual Syndrome: A Double-Blind, Randomised and Placebo-Controlled TrialDocument5 pagesCrocus Sativus L. (Saffron) in The Treatment of Premenstrual Syndrome: A Double-Blind, Randomised and Placebo-Controlled TrialhanaNo ratings yet
- Essential Hypertension (Also Called Primary Hypertension or Idiopathic Hypertension) IsDocument6 pagesEssential Hypertension (Also Called Primary Hypertension or Idiopathic Hypertension) Isbeenish ashfaqNo ratings yet
- Retained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateDocument19 pagesRetained Placenta After Vaginal Birth and Length of The Third Stage of Labor - UpToDateHartanto Lie100% (1)
- 2021 All Product Catalog - 20210601 - LowDocument87 pages2021 All Product Catalog - 20210601 - LowSridevi AnggrainiNo ratings yet