You might also like
- Declaration Declaration Declaration: Signature DateDocument2 pagesDeclaration Declaration Declaration: Signature DateQuinric Bontilao SevillejoNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormRandy OpadiaNo ratings yet
- Health Declaration Form Health Declaration Form: Respondent Information Respondent InformationDocument2 pagesHealth Declaration Form Health Declaration Form: Respondent Information Respondent InformationErnilyn Espinosa LiganNo ratings yet
- HD - Reception SantierraDocument1 pageHD - Reception SantierraAnezka Danett CortinaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormNaldrin RosalesNo ratings yet
- Coronavirus Self Declaration FormDocument1 pageCoronavirus Self Declaration Formvpo almonbevsambNo ratings yet
- House of Representatives: Republic of The PhilippinesDocument2 pagesHouse of Representatives: Republic of The PhilippinesAlvin CerezoNo ratings yet
- Creening Test For 'Associates Returning To Work DateDocument1 pageCreening Test For 'Associates Returning To Work Datejohn ralph silvaNo ratings yet
- Health Declaration Form: Respondent InformationDocument2 pagesHealth Declaration Form: Respondent Informationmyzzle mendarosNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormResame ArochaNo ratings yet
- PUP Health Declaration Form ADocument1 pagePUP Health Declaration Form ARJ DAWATONNo ratings yet
- SLMC Health Declaration FormDocument1 pageSLMC Health Declaration FormNikkiNo ratings yet
- Word ForDocument2 pagesWord ForAnthony Japhz EmuelNo ratings yet
- Name: Age: Sex: Address: Contact No: Occupation: Body TemperatureDocument2 pagesName: Age: Sex: Address: Contact No: Occupation: Body TemperatureJoshua Christian TeopengcoNo ratings yet
- Health Declaration Health Declaration: YES NO YES NODocument1 pageHealth Declaration Health Declaration: YES NO YES NOMagnificat filesNo ratings yet
- SMI COVID-19 Health Survey Form - RevisedDocument2 pagesSMI COVID-19 Health Survey Form - RevisedJess Rey Q. BaranNo ratings yet
- Phoa Health Declaration Form - TVHDocument1 pagePhoa Health Declaration Form - TVHCriszel Joy Atillano AseloNo ratings yet
- House of Representatives: Republic of The Philippines Quezon City, Metro ManilaDocument3 pagesHouse of Representatives: Republic of The Philippines Quezon City, Metro ManilamereeNo ratings yet
- Don Bosco Tvet Center-Calauan, Inc.: Km. 77, Brgy, Dayap, Calauan, Laguna. 4012Document2 pagesDon Bosco Tvet Center-Calauan, Inc.: Km. 77, Brgy, Dayap, Calauan, Laguna. 4012Johnlester Delacruz KoaNo ratings yet
- Ba Go Health Declaration FormDocument1 pageBa Go Health Declaration FormPoblacion, Brien S.No ratings yet
- SPAS Customer Health Checklist Form A4Document1 pageSPAS Customer Health Checklist Form A4kablasNo ratings yet
- Bangsamoro Transition Authority: Reminders For Physical AttendeesDocument2 pagesBangsamoro Transition Authority: Reminders For Physical AttendeesShob SinsuatNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration Formedward mirandilla miranda jr.No ratings yet
- Health Declaration Health Declaration: YES NO YES NODocument1 pageHealth Declaration Health Declaration: YES NO YES NOmike tandocNo ratings yet
- Health Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiDocument2 pagesHealth Checklist Form For Visitors: Nakaranas Ka Ba NG Mga Sumusunod: Oo HindiCoin CharNo ratings yet
- Health FormDocument1 pageHealth Formnoera angel montemayorNo ratings yet
- Health Declaration Slip: (For Contact Tracing)Document2 pagesHealth Declaration Slip: (For Contact Tracing)Aylene GersanibNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormAzri AzizNo ratings yet
- ISO Health ChecklistDocument1 pageISO Health ChecklistRonnel SaludezNo ratings yet
- Health Declaration Health Declaration: City of Mati City of MatiDocument2 pagesHealth Declaration Health Declaration: City of Mati City of MatiJosephino Castillo25% (4)
- Health Dec New 1Document1 pageHealth Dec New 1RusselNo ratings yet
- Enhealth FormDocument1 pageEnhealth Formdexter silangNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormRoseller SasisNo ratings yet
- Health-Declaration-Checklist 2Document1 pageHealth-Declaration-Checklist 2Beverly Trangia100% (2)
- Self Declaration - Covid 19 Pre Screening: SL No Check Points AnswerDocument1 pageSelf Declaration - Covid 19 Pre Screening: SL No Check Points AnswerPampanagouda YadavNo ratings yet
- COVID-19 Self-Declaration Form - Atul ValsadDocument2 pagesCOVID-19 Self-Declaration Form - Atul Valsad8460272421No ratings yet
- Health Decleration FormDocument1 pageHealth Decleration FormGabrile GUIOGUIONo ratings yet
- Health Dec New 1Document1 pageHealth Dec New 1Mary Rose RagasaNo ratings yet
- Bfp9 Health Declaration FormDocument1 pageBfp9 Health Declaration FormGelli Jane GurdielNo ratings yet
- Health Checklist Health Checklist Temperature: TemperatureDocument2 pagesHealth Checklist Health Checklist Temperature: TemperatureJeniffer FajardoNo ratings yet
- Health Declaration Form: Client Name: Email Add: Address: Date: Mobile Number: Nail TechDocument1 pageHealth Declaration Form: Client Name: Email Add: Address: Date: Mobile Number: Nail Techcindya jorduelaNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormMarriah Izzabelle Suarez RamadaNo ratings yet
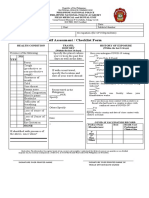
- Self Assessment / Checklist Form: YES NODocument1 pageSelf Assessment / Checklist Form: YES NOdoie kimNo ratings yet
- CHECKLIST FOR PERSONS UNDER MONITORING (For BHERT Use Only) Re 2019 nCoV ARDDocument1 pageCHECKLIST FOR PERSONS UNDER MONITORING (For BHERT Use Only) Re 2019 nCoV ARDCHICKYNo ratings yet
- Coronavirus Self-Declaration Form: Lsnurse@islux - LuDocument2 pagesCoronavirus Self-Declaration Form: Lsnurse@islux - LuSiddharth SoporiNo ratings yet
- Quarantine Form 1Document1 pageQuarantine Form 1Rachel AndesNo ratings yet
- Health Declaration Form: (Nakakaranas Ka Ba NG)Document1 pageHealth Declaration Form: (Nakakaranas Ka Ba NG)Elimer Teves Espina100% (2)
- Department of Education: Visitor'S Health Declaration FormDocument1 pageDepartment of Education: Visitor'S Health Declaration FormVian MaderaNo ratings yet
- Social Care Health Self-Declaration Form For Use During COVID-19 PandemicDocument8 pagesSocial Care Health Self-Declaration Form For Use During COVID-19 PandemicMary's CatzNo ratings yet
- Preliminary Checklist - Covid 19 - MolmiDocument2 pagesPreliminary Checklist - Covid 19 - MolmiRohit PatelNo ratings yet
- Client/Visitor Health Checklist Client/Visitor Health ChecklistDocument1 pageClient/Visitor Health Checklist Client/Visitor Health Checklistjanuary3196 :DNo ratings yet
- Health Declaration Form Health Declaration Form: Temperature: - TemperatureDocument1 pageHealth Declaration Form Health Declaration Form: Temperature: - TemperaturePrincess Ann MagbuhosNo ratings yet
- Visitors Health Check List: TemperatureDocument1 pageVisitors Health Check List: TemperatureSterben ShouchiNo ratings yet
- RFDGCDC Health and Safety Declaration FormDocument1 pageRFDGCDC Health and Safety Declaration FormChy GomezNo ratings yet
- Health & Safety Check Declaration Form: TemperatureDocument1 pageHealth & Safety Check Declaration Form: TemperatureChy GomezNo ratings yet
- School Health Declaration Survey Form A4Document1 pageSchool Health Declaration Survey Form A4Clarizze AnnNo ratings yet
- Health Survey OfficeDocument2 pagesHealth Survey OfficeLara Denise BreizNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration FormVeralynNo ratings yet
- Coronavirus on My Mind: The Journey of an ER Doc Into the Madness of COVID-19From EverandCoronavirus on My Mind: The Journey of an ER Doc Into the Madness of COVID-19No ratings yet
- Your Best Is yet to Come!: Believe-Educate-Stand-Tall Information on the Covid-19 Vaccination, Inhalation, or PillFrom EverandYour Best Is yet to Come!: Believe-Educate-Stand-Tall Information on the Covid-19 Vaccination, Inhalation, or PillNo ratings yet
- G11 - Science - Lesson PlanDocument7 pagesG11 - Science - Lesson PlanRamir BecoyNo ratings yet
- FINAL RPMS T1 3 SY 2022 2023 Pink - CaliguidDocument37 pagesFINAL RPMS T1 3 SY 2022 2023 Pink - CaliguidRamir BecoyNo ratings yet
- 1classificationandscientificnames-140712125133-phpapp01Document12 pages1classificationandscientificnames-140712125133-phpapp01Ramir BecoyNo ratings yet
- CUF_VALUES_MARINELLE M. MENDOZA_DLL (2)Document3 pagesCUF_VALUES_MARINELLE M. MENDOZA_DLL (2)Ramir BecoyNo ratings yet
- Accomplishment ReportDocument16 pagesAccomplishment ReportRamir Becoy100% (1)
- Answer SheetDocument1 pageAnswer SheetRamir BecoyNo ratings yet
- FINAL RPMS T1 3 SY 2022 2023 BecoyDocument37 pagesFINAL RPMS T1 3 SY 2022 2023 BecoyRamir Becoy100% (1)
- Quiz ScienceG7 Living&Non-LivingThingsDocument12 pagesQuiz ScienceG7 Living&Non-LivingThingsRamir BecoyNo ratings yet
- FINAL RPMS T1 3 SY 2022 2023 IgotDocument37 pagesFINAL RPMS T1 3 SY 2022 2023 IgotRamir Becoy100% (3)
- SF2 Lact 1Document9 pagesSF2 Lact 1Ramir BecoyNo ratings yet
- Action Plan For RemedialDocument3 pagesAction Plan For RemedialRamir BecoyNo ratings yet
- CS Form 86 Health Exam RecordDocument1 pageCS Form 86 Health Exam RecordRamir BecoyNo ratings yet
- Strategic Intervention Material For GradDocument16 pagesStrategic Intervention Material For GradRamir BecoyNo ratings yet
- English 9 - Second&Third ConditionalsDocument2 pagesEnglish 9 - Second&Third ConditionalsRamir BecoyNo ratings yet
- 7th Grade Chap 1 Scientific Method PPT PDFDocument15 pages7th Grade Chap 1 Scientific Method PPT PDFRamir BecoyNo ratings yet
- Q2 - M3 - What Are TheseDocument4 pagesQ2 - M3 - What Are TheseRamir BecoyNo ratings yet
- Q2 - M3 - Living ThingsDocument2 pagesQ2 - M3 - Living ThingsRamir BecoyNo ratings yet
- Summative Test - Understanding TyphoonDocument18 pagesSummative Test - Understanding TyphoonRamir BecoyNo ratings yet
- Act. 3 What Makes Up An OrganismDocument12 pagesAct. 3 What Makes Up An OrganismRamir BecoyNo ratings yet
- Science Quiz Fault Earthquake SeismicDocument34 pagesScience Quiz Fault Earthquake SeismicRamir BecoyNo ratings yet
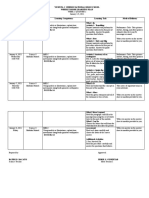
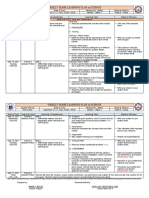
- Weekly Home Learning Plan in ScienceDocument14 pagesWeekly Home Learning Plan in ScienceRamir BecoyNo ratings yet
- Science - 7: Unified Summative Assessment (Quarter 2 - Week 1 and 2)Document3 pagesScience - 7: Unified Summative Assessment (Quarter 2 - Week 1 and 2)Ramir BecoyNo ratings yet
- Act. 2 Parts & Funsctions of MicroscopeDocument9 pagesAct. 2 Parts & Funsctions of MicroscopeRamir BecoyNo ratings yet
- Summative Test-Sci8-Particle of MatterDocument21 pagesSummative Test-Sci8-Particle of MatterRamir Becoy100% (1)
- CGAP - Steps in Decision MakingDocument26 pagesCGAP - Steps in Decision MakingRamir BecoyNo ratings yet
- 1-WHLP Sci8 Q1 W1Document2 pages1-WHLP Sci8 Q1 W1Ramir BecoyNo ratings yet
- Weekly Home Learning Plan in ScienceDocument4 pagesWeekly Home Learning Plan in ScienceRamir BecoyNo ratings yet
- Science G7 Q1Document4 pagesScience G7 Q1Ramir BecoyNo ratings yet
- TOS - ArPan G8Document2 pagesTOS - ArPan G8Ramir BecoyNo ratings yet
- Unified Summative TOS G7Document3 pagesUnified Summative TOS G7Ramir BecoyNo ratings yet
- Product Management GemsDocument14 pagesProduct Management GemsVijendra GopaNo ratings yet
- Application For MigrationDocument8 pagesApplication For Migrationmoments444No ratings yet
- Cassava Starch Granule Structure-Function Properties - Influence of Time and Conditions at Harvest On Four Cultivars of Cassava StarchDocument10 pagesCassava Starch Granule Structure-Function Properties - Influence of Time and Conditions at Harvest On Four Cultivars of Cassava Starchwahyuthp43No ratings yet
- Business en Pre Above S+T ReadingDocument3 pagesBusiness en Pre Above S+T Readingsvetlana939No ratings yet
- Impact of Carding Segments On Quality of Card Sliver: Practical HintsDocument1 pageImpact of Carding Segments On Quality of Card Sliver: Practical HintsAqeel AhmedNo ratings yet
- Salumber ProjectDocument103 pagesSalumber ProjectVandhana RajasekaranNo ratings yet
- The 8051 Microcontroller & Embedded Systems: Muhammad Ali Mazidi, Janice Mazidi & Rolin MckinlayDocument15 pagesThe 8051 Microcontroller & Embedded Systems: Muhammad Ali Mazidi, Janice Mazidi & Rolin MckinlayAkshwin KisoreNo ratings yet
- 1 Conflict in NG - Report - 28FEB2018Document46 pages1 Conflict in NG - Report - 28FEB2018KrishnaNo ratings yet
- APCJ Directory 2019Document34 pagesAPCJ Directory 2019Anonymous Pu3OF7100% (3)
- Response LTR 13 330 VielmettiDocument2 pagesResponse LTR 13 330 VielmettiAnn Arbor Government DocumentsNo ratings yet
- Contoh Kuda-Kuda Untuk Pak Henry Truss D&EKK1L KDocument1 pageContoh Kuda-Kuda Untuk Pak Henry Truss D&EKK1L KDhany ArsoNo ratings yet
- Resume 202309040934Document5 pagesResume 202309040934dubai eyeNo ratings yet
- Marketing Research ProjectDocument37 pagesMarketing Research ProjectVijay100% (15)
- Blanko Permohonan VettingDocument1 pageBlanko Permohonan VettingTommyNo ratings yet
- Daily Price Monitoring: Retail Prices of Selected Agri-Fishery Commodities in Selected Markets in Metro ManilaDocument3 pagesDaily Price Monitoring: Retail Prices of Selected Agri-Fishery Commodities in Selected Markets in Metro ManilaRio CorralNo ratings yet
- Diagrama Electronico EGED 285Document2 pagesDiagrama Electronico EGED 285Carlos Juarez Chunga100% (1)
- PX4211 2Document3 pagesPX4211 2kalpanaNo ratings yet
- Outline - Essay and Argumentative EssayDocument2 pagesOutline - Essay and Argumentative EssayGabbo GómezNo ratings yet
- Challenges Faced by DMRCDocument2 pagesChallenges Faced by DMRCSourabh Kr67% (3)
- ACC 101 - 3rd QuizDocument3 pagesACC 101 - 3rd QuizAdyangNo ratings yet
- Hw5 MaterialsDocument2 pagesHw5 MaterialsmehdiNo ratings yet
- X25Document10 pagesX25RajNo ratings yet
- 9MFY18 MylanDocument94 pages9MFY18 MylanRahul GautamNo ratings yet
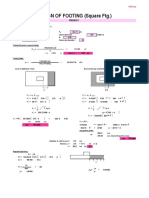
- Design of Footing (Square FTG.) : M Say, L 3.75Document2 pagesDesign of Footing (Square FTG.) : M Say, L 3.75victoriaNo ratings yet
- 99990353-Wsi4-2 C1D2-7940022562 7950022563 7940022564Document2 pages99990353-Wsi4-2 C1D2-7940022562 7950022563 7940022564alltheloveintheworldNo ratings yet
- MAYA1010 EnglishDocument30 pagesMAYA1010 EnglishjailsondelimaNo ratings yet
- Datascope System 98Document16 pagesDatascope System 98Guillermo ZalazarNo ratings yet
- Normas FieldbusDocument3 pagesNormas FieldbusAlielson PazNo ratings yet
- Katalog Bonnier BooksDocument45 pagesKatalog Bonnier BooksghitahirataNo ratings yet
- (Developer Shed Network) Server Side - PHP - Database Abstraction With PHPDocument29 pages(Developer Shed Network) Server Side - PHP - Database Abstraction With PHPSeher KurtayNo ratings yet