You might also like
- Geriatric Anxiety Scale v2.0 FINALDocument2 pagesGeriatric Anxiety Scale v2.0 FINALpujipurwaningsih67% (3)
- Bates-Jensen Wound Assessment Tool (BWAT)Document4 pagesBates-Jensen Wound Assessment Tool (BWAT)Jamie OngNo ratings yet
- CS1 Assignment Y2 2020 Answer Booklet 12345Document4 pagesCS1 Assignment Y2 2020 Answer Booklet 12345Deepanshu Sharma0% (1)
- Cambridge CertificateDocument2 pagesCambridge Certificateapi-322275865No ratings yet
- Developing A Utility Index For The Aberrant Behavior Checklist (ABC-C) For Fragile X SyndromeDocument10 pagesDeveloping A Utility Index For The Aberrant Behavior Checklist (ABC-C) For Fragile X SyndromeIke Kashaka TshikungNo ratings yet
- Lesson Plan For Introduction To Vector MathDocument1 pageLesson Plan For Introduction To Vector MathLeonardo MuñozNo ratings yet
- Research Article: Prognostic Factors of Functional Recovery From Left Hemispheric StrokeDocument8 pagesResearch Article: Prognostic Factors of Functional Recovery From Left Hemispheric Strokepokharelriwaj82No ratings yet
- Adobe Scan 02 Mar 2023Document18 pagesAdobe Scan 02 Mar 2023ciptakarwanaNo ratings yet
- Mckee 2012Document10 pagesMckee 2012Reda SoNo ratings yet
- Roy Adaptation Model Extremities Amputation PDFDocument7 pagesRoy Adaptation Model Extremities Amputation PDFIntan SariNo ratings yet
- 6-1Document8 pages6-1Elahe SadeqiNo ratings yet
- Rotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Document12 pagesRotator Cuff Repair vs. Nonoperative Treatment - 2021 (Tema 3)Carlos NoronaNo ratings yet
- Gum Mess On 2003Document6 pagesGum Mess On 2003fajarcolzzzNo ratings yet
- Stroke 32Document8 pagesStroke 32pokharelriwaj82No ratings yet
- Self-Efficacy in Relation To Impairments and Activities of Daily Living Disability in Elderly Patients With Stroke: A Prospective InvestigationDocument6 pagesSelf-Efficacy in Relation To Impairments and Activities of Daily Living Disability in Elderly Patients With Stroke: A Prospective InvestigationUliuliauliaNo ratings yet
- 2021 - QoL in MSisdominated by Fatigue - Disability - Sefl-EfficacyDocument7 pages2021 - QoL in MSisdominated by Fatigue - Disability - Sefl-EfficacySM199021No ratings yet
- Katzan Et AlDocument9 pagesKatzan Et Alemsutton02No ratings yet
- Acl Rehab ProtocolDocument6 pagesAcl Rehab ProtocolPricy DevNo ratings yet
- Review 2013Document11 pagesReview 2013marioNo ratings yet
- Physiotherapy Intervention in Alzheimer'sDocument12 pagesPhysiotherapy Intervention in Alzheimer'sRestu AryaNo ratings yet
- Functioning of Stroke Survivors - A Validation of The ICF Core Set For Stroke in SwedenDocument9 pagesFunctioning of Stroke Survivors - A Validation of The ICF Core Set For Stroke in SwedenMuhammadMusa47No ratings yet
- Self-Efficacy Correlates with Independence in Stroke SurvivorsDocument7 pagesSelf-Efficacy Correlates with Independence in Stroke SurvivorsSitti Rosdiana YahyaNo ratings yet
- Cirugía de HAV y Calidad de VidaDocument8 pagesCirugía de HAV y Calidad de VidaAlejandro Fernandez GibelloNo ratings yet
- Kta ArticleDocument6 pagesKta Articleapi-291380671No ratings yet
- Stroke AFRDocument9 pagesStroke AFRPrasasti 19No ratings yet
- Hospitalized Older Adult Predictors of Functional DeclineDocument10 pagesHospitalized Older Adult Predictors of Functional DeclineMauricio LorcaNo ratings yet
- ArticleDocument11 pagesArticlejesica_loNo ratings yet
- Application of Clinical Nursing Pathway Table of Pulmonary Management in Patients With Adolescent Idiopathic ScoliosisDocument6 pagesApplication of Clinical Nursing Pathway Table of Pulmonary Management in Patients With Adolescent Idiopathic Scoliosis605706503No ratings yet
- Fall Prediction in Neurological Gait Disorders DifDocument15 pagesFall Prediction in Neurological Gait Disorders DifRudolfGerNo ratings yet
- Yjmt 30 1992090Document13 pagesYjmt 30 1992090Luis Sebastian Arango OspinaNo ratings yet
- 4-1Document9 pages4-1Elahe SadeqiNo ratings yet
- Akizuki Et Al.Document6 pagesAkizuki Et Al.Dries Van ThielenNo ratings yet
- Jurnal Demensia 5Document9 pagesJurnal Demensia 5Mutiara Anak NegeriNo ratings yet
- Poststroke Depression: Prevalence and Determinants in Brazilian Stroke PatientsDocument10 pagesPoststroke Depression: Prevalence and Determinants in Brazilian Stroke PatientsGrace KahonoNo ratings yet
- Gye Yeop Kim Et Al 2014Document6 pagesGye Yeop Kim Et Al 2014maria.castiyo2002No ratings yet
- Ggi 13069Document7 pagesGgi 13069putriNo ratings yet
- PDF 60574 4818Document13 pagesPDF 60574 4818QuiroprácticaParaTodosNo ratings yet
- Lee 2018Document7 pagesLee 2018Kings AndrewNo ratings yet
- Neuromuscular Electrical Stimulation Improves Muscle Strength Biomechanicsof Movementand Functional MobilityDocument19 pagesNeuromuscular Electrical Stimulation Improves Muscle Strength Biomechanicsof Movementand Functional MobilityAmr Mohamed GalalNo ratings yet
- Frailty and Exercise Training - How To Provide Best Care After Cardiac Surgery or Intervention For Elder Patients With Valvular Heart Disease 2018Document36 pagesFrailty and Exercise Training - How To Provide Best Care After Cardiac Surgery or Intervention For Elder Patients With Valvular Heart Disease 2018Josemi Del Castillo MolinaNo ratings yet
- Aquatic Therapy For MsDocument7 pagesAquatic Therapy For MsmadeNo ratings yet
- Journal 2Document5 pagesJournal 2nandhini raguNo ratings yet
- Rehabilitation in Patients With Rheumatoid Arhtritis 61 74Document14 pagesRehabilitation in Patients With Rheumatoid Arhtritis 61 74Yustia Ika WardhaniNo ratings yet
- Do measures of reactive balance control predict falls in people with stroke returningDocument12 pagesDo measures of reactive balance control predict falls in people with stroke returningElahe SadeqiNo ratings yet
- Abstract Leftsidest SetDocument1,047 pagesAbstract Leftsidest Setpokharelriwaj82No ratings yet
- Clinical Efficacy of Mechanical Traction As Physical Therapy For Lumbar Disc Herniation - Meta AnalysisDocument8 pagesClinical Efficacy of Mechanical Traction As Physical Therapy For Lumbar Disc Herniation - Meta AnalysissamNo ratings yet
- Alp Tekin 2016Document6 pagesAlp Tekin 2016Anisah Imansari RahayuNo ratings yet
- Main 25Document6 pagesMain 25pokharelriwaj82No ratings yet
- Rheumatoid Arthritis - Assessment of Functional Performances of The PatientsDocument14 pagesRheumatoid Arthritis - Assessment of Functional Performances of The PatientsK. Vijay AnanthNo ratings yet
- Review of Effects of Physical Activity On Strength, Balance, Mobility and ADL Performance in Elderly Subjects With DementiaDocument11 pagesReview of Effects of Physical Activity On Strength, Balance, Mobility and ADL Performance in Elderly Subjects With DementiaAlejandra VasquezNo ratings yet
- ISPR8-1352: Posters (First Part) / Annals of Physical and Rehabilitation Medicine 61S (2018) E103-E308 E219Document1 pageISPR8-1352: Posters (First Part) / Annals of Physical and Rehabilitation Medicine 61S (2018) E103-E308 E219Amal VRNo ratings yet
- 2019 Comparable Walking Gait PerformanceDocument5 pages2019 Comparable Walking Gait Performancesiyueli826No ratings yet
- 2008 - Feigin - Long Term Neuropsychological Functional Outcomes StrokeDocument8 pages2008 - Feigin - Long Term Neuropsychological Functional Outcomes StrokeLourdes CFNo ratings yet
- Jurnal GerontikDocument8 pagesJurnal GerontikLIZBETH FEMMIL SAPUTRINo ratings yet
- Intervention:: American Occupational Therapy Association Evidence-Based Literature Review Project/Evidence Table.5-06Document5 pagesIntervention:: American Occupational Therapy Association Evidence-Based Literature Review Project/Evidence Table.5-06nkdewittNo ratings yet
- The Swedish Occupational Fatigue Inventory in People With Multiple SclerosisDocument7 pagesThe Swedish Occupational Fatigue Inventory in People With Multiple SclerosisikrambahariNo ratings yet
- Bab 2Document2 pagesBab 2SANDA NABILAH FATINNo ratings yet
- Rodríguez-Hernández Et Al. - 2021 - Effects of Specific Virtual Reality-Based TherapyDocument15 pagesRodríguez-Hernández Et Al. - 2021 - Effects of Specific Virtual Reality-Based TherapyMARIA TERAPEUTANo ratings yet
- Impact of Physical Activity On Disability Risk inDocument7 pagesImpact of Physical Activity On Disability Risk inLyrian LohNo ratings yet
- Stroke RehabilitationDocument10 pagesStroke RehabilitationPethuel Pomaloy100% (1)
- STROKE REHABILITATION EVIDENCEDocument36 pagesSTROKE REHABILITATION EVIDENCEMarikit2012No ratings yet
- Activities of Daily Living and Quality of Life in Persons With Muscular DystrophyDocument6 pagesActivities of Daily Living and Quality of Life in Persons With Muscular DystrophyHenry wijaya oeijNo ratings yet
- Review Article Extracorporeal Shock Wave Therapy For The Treatment of Osteoarthritis: A Systematic Review and Meta-AnalysisDocument15 pagesReview Article Extracorporeal Shock Wave Therapy For The Treatment of Osteoarthritis: A Systematic Review and Meta-Analysissymbiosis.ikfrNo ratings yet
- Interventions for Autism: Evidence for Educational and Clinical PracticeFrom EverandInterventions for Autism: Evidence for Educational and Clinical PracticeNo ratings yet
- Psychophysiological assessment of human cognition and its enhancement by a non-invasive methodFrom EverandPsychophysiological assessment of human cognition and its enhancement by a non-invasive methodNo ratings yet
- Self-directed Learning Skills in Honduras Compared to the United StatesDocument19 pagesSelf-directed Learning Skills in Honduras Compared to the United StatesZilbran BerontaxNo ratings yet
- Role of Bacterial Infections in Pancreatic Cancer: ReviewDocument5 pagesRole of Bacterial Infections in Pancreatic Cancer: ReviewZilbran BerontaxNo ratings yet
- Understanding Doctoral Nursing Students' Experiences of Blended LearningDocument8 pagesUnderstanding Doctoral Nursing Students' Experiences of Blended LearningZilbran BerontaxNo ratings yet
- Self-Directed Learning Methods On Nursing Education: A Literature ReviewDocument8 pagesSelf-Directed Learning Methods On Nursing Education: A Literature ReviewZilbran BerontaxNo ratings yet
- Speech and Language Therapy For Aphasia Following Subacute StrokeDocument6 pagesSpeech and Language Therapy For Aphasia Following Subacute StrokeZilbran BerontaxNo ratings yet
- Transtition To Blended LearningDocument17 pagesTranstition To Blended LearningZilbran BerontaxNo ratings yet
- The Effects of Blended Learning On Knowledge, Skills, and Satisfaction Innursing Students A Meta-AnalysisDocument7 pagesThe Effects of Blended Learning On Knowledge, Skills, and Satisfaction Innursing Students A Meta-AnalysisZilbran BerontaxNo ratings yet
- The Self-Directed Learning Readiness Level of The Undergraduate Students of Midwife and Nurse in Terms of Sustainability in Nursing and Midwifery EducationDocument14 pagesThe Self-Directed Learning Readiness Level of The Undergraduate Students of Midwife and Nurse in Terms of Sustainability in Nursing and Midwifery EducationZilbran BerontaxNo ratings yet
- Blended Learning (Research Article)Document12 pagesBlended Learning (Research Article)Andrés Espinoza100% (1)
- The Impact of Blended Teaching On Knowledge, Satisfaction, and Self-Directed Learning in Nursing Undergraduates: A Randomized, Controlled TrialDocument7 pagesThe Impact of Blended Teaching On Knowledge, Satisfaction, and Self-Directed Learning in Nursing Undergraduates: A Randomized, Controlled TrialJefry ArieNo ratings yet
- Bencana 1Document14 pagesBencana 1Andhi SNo ratings yet
- Validation of Self-Directed LearningDocument11 pagesValidation of Self-Directed LearningZilbran BerontaxNo ratings yet
- Effectiveness of A Self-Directed LearningDocument8 pagesEffectiveness of A Self-Directed LearningZilbran BerontaxNo ratings yet
- Simulation Videos Presented in A Blended Learning Platform ToDocument27 pagesSimulation Videos Presented in A Blended Learning Platform ToZilbran BerontaxNo ratings yet
- The Impact of The Learning Contract On Self-Directed LearningDocument5 pagesThe Impact of The Learning Contract On Self-Directed LearningZilbran BerontaxNo ratings yet
- Self-Directed Learning A Tool For Lifelong LearningDocument15 pagesSelf-Directed Learning A Tool For Lifelong LearningZilbran BerontaxNo ratings yet
- Effect of Self-Directed Learning On Nursing Students' Readiness, Perception and Performance in SudanDocument10 pagesEffect of Self-Directed Learning On Nursing Students' Readiness, Perception and Performance in SudanZilbran BerontaxNo ratings yet
- LR SDL - 7. OutDocument7 pagesLR SDL - 7. OutAnggita Nandya ArdiatiNo ratings yet
- Effect of Self-Directed Learning On Nursing Students' Readiness, Perception and Performance in SudanDocument10 pagesEffect of Self-Directed Learning On Nursing Students' Readiness, Perception and Performance in SudanZilbran BerontaxNo ratings yet
- Effect of Blended Learning On Newly Nursing Student's Outcomes Regarding New Trends in Nursing Subject at Ain Shams UniversityDocument9 pagesEffect of Blended Learning On Newly Nursing Student's Outcomes Regarding New Trends in Nursing Subject at Ain Shams UniversityZilbran BerontaxNo ratings yet
- Scientific Information System: Network of Scientific Journals From Latin America, The Caribbean, Spain and PortugalDocument12 pagesScientific Information System: Network of Scientific Journals From Latin America, The Caribbean, Spain and PortugalZilbran BerontaxNo ratings yet
- Measure Nursing Student Self-Directed Learning AbilitiesDocument8 pagesMeasure Nursing Student Self-Directed Learning AbilitiesZilbran BerontaxNo ratings yet
- Concurrent Validity of Self-Rating Scale ofDocument11 pagesConcurrent Validity of Self-Rating Scale ofZilbran BerontaxNo ratings yet
- Exploratory Study of The Relationship Between Self-Directed Learning and Academic Performance in A Web - Based Learning EnvironmentDocument11 pagesExploratory Study of The Relationship Between Self-Directed Learning and Academic Performance in A Web - Based Learning EnvironmentZilbran BerontaxNo ratings yet
- Effect of Blended Learning On Newly Nursing Student's Outcomes Regarding New Trends in Nursing Subject at Ain Shams UniversityDocument9 pagesEffect of Blended Learning On Newly Nursing Student's Outcomes Regarding New Trends in Nursing Subject at Ain Shams UniversityZilbran BerontaxNo ratings yet
- Blended Versus Lecture LearningDocument5 pagesBlended Versus Lecture LearningZilbran BerontaxNo ratings yet
- Blended Learning The New Normal and Emerging Technologies PDFDocument16 pagesBlended Learning The New Normal and Emerging Technologies PDFBagas Annas UtomoNo ratings yet
- Blended Learning in High School Chemistry ToDocument11 pagesBlended Learning in High School Chemistry ToZilbran BerontaxNo ratings yet
- Down Syndrome and AutismDocument8 pagesDown Syndrome and AutismChristine Joy GonzalesNo ratings yet
- IIC Annual Report 2021-22Document30 pagesIIC Annual Report 2021-22Aeronautical ACSCENo ratings yet
- Detailed Lesson Plan in Science ViDocument6 pagesDetailed Lesson Plan in Science ViJustin Ace MallorcaNo ratings yet
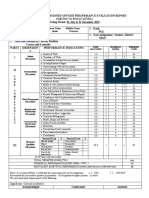
- Ratee's Name Last Name, Given Name Middle Name Galvez Jessie PanaresDocument2 pagesRatee's Name Last Name, Given Name Middle Name Galvez Jessie PanaresMeredith GalvezNo ratings yet
- Dualtech Training Center Presentation RVSADocument17 pagesDualtech Training Center Presentation RVSADennis SalongaNo ratings yet
- Heads Up 2023Document6 pagesHeads Up 2023api-39965614No ratings yet
- Dream Tending - What It IsDocument3 pagesDream Tending - What It IsNick JudsonNo ratings yet
- DepEd Order On Time Allotment Per Learning Areas - TeacherPHDocument1 pageDepEd Order On Time Allotment Per Learning Areas - TeacherPHsjnhs SPANo ratings yet
- Download ebook Intermediate Macroeconomics Pdf full chapter pdfDocument67 pagesDownload ebook Intermediate Macroeconomics Pdf full chapter pdfjulia.castro488100% (27)
- Report Assessment 1 CSC264 - Muhammad Hafiz Imran Bin AhmadDocument9 pagesReport Assessment 1 CSC264 - Muhammad Hafiz Imran Bin AhmadMUHD HAFIZ IMRAN BIN AHMADNo ratings yet
- Ead-519 Dress Code Case AnalysisDocument4 pagesEad-519 Dress Code Case Analysisapi-642173798No ratings yet
- NAPLAN Yr 9 Numeracy Test-3 CalcAllowedDocument11 pagesNAPLAN Yr 9 Numeracy Test-3 CalcAllowedLeezaNo ratings yet
- Bns Accomplishment ReportDocument4 pagesBns Accomplishment ReportRaquel ParcareyNo ratings yet
- Black History Month LessonDocument11 pagesBlack History Month LessonJ JohnsonNo ratings yet
- Introduction to Symposium on Public Service Motivation ResearchDocument3 pagesIntroduction to Symposium on Public Service Motivation ResearchHumberto RiveraNo ratings yet
- Applications OF Artificial Intelligence FOR Organic ChemistryDocument203 pagesApplications OF Artificial Intelligence FOR Organic ChemistryMichael RoseNo ratings yet
- Managing For Quality and Performance Excellence, 9E, © 2014 Cengage PublishingDocument46 pagesManaging For Quality and Performance Excellence, 9E, © 2014 Cengage PublishingWilsonNo ratings yet
- Week 9-Gagarin, Jophnel Noa B.Document3 pagesWeek 9-Gagarin, Jophnel Noa B.JOPHNEL NOA GAGARINNo ratings yet
- Bahasa Inggris (Iklan Pekerjaan)Document5 pagesBahasa Inggris (Iklan Pekerjaan)AndreNo ratings yet
- PEpC 1Document44 pagesPEpC 1Claudio Makarovsky100% (1)
- IntroductionDocument6 pagesIntroductionNigel KowNo ratings yet
- Create New Java Red5 Application - TsavoDocument38 pagesCreate New Java Red5 Application - TsavoFabrizio TorelliNo ratings yet
- CV AnalysisDocument6 pagesCV Analysisbaniyash1204No ratings yet
- UAE4 School List4Document82 pagesUAE4 School List4Javeed MohiuddinNo ratings yet
- IATF Internal Auditor 2019Document1 pageIATF Internal Auditor 2019Prakash kumarTripathiNo ratings yet
- Intro to Philosophy of Human Person Chapter 1Document90 pagesIntro to Philosophy of Human Person Chapter 1Adrian Nicole DionisioNo ratings yet
- Accreditation of CME Programme As Approved by Governing Body of U P Medical Council, Lucknow On 11 April 2012Document9 pagesAccreditation of CME Programme As Approved by Governing Body of U P Medical Council, Lucknow On 11 April 2012GauravChopraNo ratings yet