You might also like
- SULPYCO Method: A New Quantum and Integrative Approach to DepressionFrom EverandSULPYCO Method: A New Quantum and Integrative Approach to DepressionNo ratings yet
- Treat AcuteDocument8 pagesTreat AcuteShane LeeNo ratings yet
- Clozapine and Haloperidol in ModeratelyDocument8 pagesClozapine and Haloperidol in Moderatelyrinaldiapt08No ratings yet
- Aripiprazole in Schizophrenia and Schizo PDFDocument18 pagesAripiprazole in Schizophrenia and Schizo PDFAlexandra PopaNo ratings yet
- Clozapine in Treatment of Schizophrenia: V. Burtea P. Ifteni A Teodorescu L. RogozeaDocument6 pagesClozapine in Treatment of Schizophrenia: V. Burtea P. Ifteni A Teodorescu L. RogozeaReza Badruun Syahrul HakimNo ratings yet
- Atypical Antipsychotic Augmentation in Major Depressive DisorderDocument13 pagesAtypical Antipsychotic Augmentation in Major Depressive DisorderrantiNo ratings yet
- 86ba PDFDocument298 pages86ba PDFKanesti KamajayaNo ratings yet
- Olanzapine Shows Superior Efficacy and Safety Profile Compared to Haloperidol in Treating SchizophreniaDocument10 pagesOlanzapine Shows Superior Efficacy and Safety Profile Compared to Haloperidol in Treating SchizophreniaWaoNo ratings yet
- Observations On The Action of Sernyl - A New Psychotropic DrugDocument8 pagesObservations On The Action of Sernyl - A New Psychotropic DrugAnna MNo ratings yet
- Serum Monitoring of Antipsychotic Drug Levels During Concomitant Administration of Sertraline and Antipsychotic MedicationDocument4 pagesSerum Monitoring of Antipsychotic Drug Levels During Concomitant Administration of Sertraline and Antipsychotic MedicationIulia CiocotisanNo ratings yet
- Comparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaDocument6 pagesComparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaLonkesNo ratings yet
- Antipsychotic Medication in Schizophrenia - A ReviewDocument11 pagesAntipsychotic Medication in Schizophrenia - A Reviewrisang akrima fikriNo ratings yet
- Clotiapine - Another Forgotten Treassure in PsychiatryDocument1 pageClotiapine - Another Forgotten Treassure in PsychiatryJuan IgnacioNo ratings yet
- Journal of Schizophrenia ResearchDocument8 pagesJournal of Schizophrenia ResearchAustin Publishing GroupNo ratings yet
- Clozapine: SchizophrenicDocument8 pagesClozapine: SchizophrenicVictoria FellowsNo ratings yet
- Lally 2015Document11 pagesLally 2015Mariana PestanaNo ratings yet
- Rajiv P. Sharma Et Al - CSF Neurotensin Concentrations and Antipsychotic Treatment in Schizophrenia and Schizoaffective DisorderDocument3 pagesRajiv P. Sharma Et Al - CSF Neurotensin Concentrations and Antipsychotic Treatment in Schizophrenia and Schizoaffective DisorderLonkesNo ratings yet
- BarbuiDocument8 pagesBarbuirinaldiapt08No ratings yet
- Stroup2019 PDFDocument2 pagesStroup2019 PDFGrayfox89No ratings yet
- Kane1988 PDFDocument8 pagesKane1988 PDFRavi KumarNo ratings yet
- Basic Clin Pharma Tox - 2020 - Baandrup - Polypharmacy in SchizophreniaDocument10 pagesBasic Clin Pharma Tox - 2020 - Baandrup - Polypharmacy in SchizophreniaSusana Pérez ReyesNo ratings yet
- Vol 54 No 2 Patel Selby YekkiralaDocument5 pagesVol 54 No 2 Patel Selby YekkiralaDrashua AshuaNo ratings yet
- Another View of Antipsychotic Drug DiscoveryDocument7 pagesAnother View of Antipsychotic Drug DiscoveryMaya EidolonNo ratings yet
- Research ProposalDocument4 pagesResearch Proposalapi-3215069410% (1)
- Body (13-112)Document100 pagesBody (13-112)gion.nandNo ratings yet
- 13 Common Errors in Psychopharmacology: EditorialDocument8 pages13 Common Errors in Psychopharmacology: Editorialgion.nandNo ratings yet
- paliperidona revision 18 pagsDocument19 pagespaliperidona revision 18 pagsRodrigo SosaNo ratings yet
- Second Generation Atypical Antipsychotics Olanzapine and Aripiprazole Reduce Expression and Secretion of Inflammatory Cytokines in Human Immune CellsDocument8 pagesSecond Generation Atypical Antipsychotics Olanzapine and Aripiprazole Reduce Expression and Secretion of Inflammatory Cytokines in Human Immune CellsaulyaNo ratings yet
- CHORHostility CITROME PsychServ2001Document5 pagesCHORHostility CITROME PsychServ2001Leslie CitromeNo ratings yet
- Beyond Dopamine Receptor Antagonism, New Targets For SCZ Treatment and PreventionDocument18 pagesBeyond Dopamine Receptor Antagonism, New Targets For SCZ Treatment and Preventionjanicesusanto2000No ratings yet
- McCutcheon Et Al-2020-World PsychiatryDocument19 pagesMcCutcheon Et Al-2020-World PsychiatryRob McCutcheonNo ratings yet
- Freudenreich 2002Document8 pagesFreudenreich 2002citra kurnia pratiwiNo ratings yet
- Cari Jurnal 1Document10 pagesCari Jurnal 1Bianca CaterinalisendraNo ratings yet
- Patofisiologi Depresi Koda KimbleDocument4 pagesPatofisiologi Depresi Koda KimbleSri DewiNo ratings yet
- Aripiprazol in Delirium La Pacientii VarstniciDocument10 pagesAripiprazol in Delirium La Pacientii VarstniciRobert MovileanuNo ratings yet
- Schizophrenia: Recent Advances and Future Hopes: by Ahmad Al-Dabbas Resident in PsychiatryDocument25 pagesSchizophrenia: Recent Advances and Future Hopes: by Ahmad Al-Dabbas Resident in PsychiatryAhmad DabbasNo ratings yet
- DocumentDocument5 pagesDocumentTop MusicNo ratings yet
- The Long-Term Effects of Antipsychotic Medication on 精神病病程Document9 pagesThe Long-Term Effects of Antipsychotic Medication on 精神病病程wen zhangNo ratings yet
- Mechanism of Action of Antipsychotics: Antipsychotics: Pharmacology and Clinical Decision MakingDocument4 pagesMechanism of Action of Antipsychotics: Antipsychotics: Pharmacology and Clinical Decision MakingLuhur Anggoro SulistioNo ratings yet
- Schizophrenia Case StudyDocument3 pagesSchizophrenia Case StudyKumar Suryavanshi100% (1)
- TreatmentResistantSchizophreniaReview CITROME Neuropsych2011Document23 pagesTreatmentResistantSchizophreniaReview CITROME Neuropsych2011Leslie CitromeNo ratings yet
- Clozapine Augmented With Risperidone in The Treatment of Schizophrenia: A Randomized, Double-Blind, Placebo-Controlled TrialDocument8 pagesClozapine Augmented With Risperidone in The Treatment of Schizophrenia: A Randomized, Double-Blind, Placebo-Controlled TrialIga Faldini GazaliNo ratings yet
- Effect of Chlorpromazine and Haloperidol Combination on Lipid LevelsDocument10 pagesEffect of Chlorpromazine and Haloperidol Combination on Lipid LevelstrianaamaliaNo ratings yet
- Case Based Clinical Pearls - A Schizophrenic Case StudyDocument5 pagesCase Based Clinical Pearls - A Schizophrenic Case StudyTeofel John Alvizo PantaleonNo ratings yet
- Off-Label Use of Sodium Valproate For SchizophreniaDocument7 pagesOff-Label Use of Sodium Valproate For SchizophreniaHaya GrinvaldNo ratings yet
- Akathisia Dystonia Opisthotonos: Extrapyramidal Symptoms (EPS)Document11 pagesAkathisia Dystonia Opisthotonos: Extrapyramidal Symptoms (EPS)Ghana HendraNo ratings yet
- Treatments For Schizophrenia: A Critical Review of Pharmacology and Mechanisms of Action of Antipsychotic DrugsDocument26 pagesTreatments For Schizophrenia: A Critical Review of Pharmacology and Mechanisms of Action of Antipsychotic DrugsMaria Jose CastañedaNo ratings yet
- Ijmrhs Vol 4 Issue 3Document263 pagesIjmrhs Vol 4 Issue 3editorijmrhsNo ratings yet
- Farmacologia de Los Medicamentos Antipsicoticos en AmDocument9 pagesFarmacologia de Los Medicamentos Antipsicoticos en AmedgarmoncadaNo ratings yet
- The Treatment of SchizophreniaDocument9 pagesThe Treatment of Schizophreniaapi-542787928No ratings yet
- Pharmacotherapy Options for Treatment-Resistant SchizophreniaDocument6 pagesPharmacotherapy Options for Treatment-Resistant SchizophreniaSAURABH SINGHNo ratings yet
- PHARMACOLOGY OF PSYCHOSIS AND MANIADocument53 pagesPHARMACOLOGY OF PSYCHOSIS AND MANIAlavanyakakarlaNo ratings yet
- Research PaperDocument8 pagesResearch Paperapi-698797022No ratings yet
- Atypical Antipsychotics-Induced MetabolicDocument13 pagesAtypical Antipsychotics-Induced MetabolicjhuNo ratings yet
- Muscarinic Cholinergic Receptor Agonist and Peripheral Antagonist For Schizophrenia (2021)Document10 pagesMuscarinic Cholinergic Receptor Agonist and Peripheral Antagonist For Schizophrenia (2021)ShadeLRKNo ratings yet
- Kleptomania After Head Trauma: Two Case Reports and Combination Treatment StrategiesDocument5 pagesKleptomania After Head Trauma: Two Case Reports and Combination Treatment StrategiesChloe AnnNo ratings yet
- AP JayubDocument4 pagesAP JayubUsama Bin ZubairNo ratings yet
- Prolactin Response to Buspirone in Drug-Naive DepressionDocument6 pagesProlactin Response to Buspirone in Drug-Naive DepressionDoraV.MarlantiNo ratings yet
- SchizoDocument4 pagesSchizoArlene Bonife MontallanaNo ratings yet
- Add-On Pharmacotherapy For PatientsDocument2 pagesAdd-On Pharmacotherapy For PatientsmarcoNo ratings yet
- Research On Religion, Spirituality, and Mental Health 2Document9 pagesResearch On Religion, Spirituality, and Mental Health 2mijon46No ratings yet
- The Sigma-1 Receptor AsDocument17 pagesThe Sigma-1 Receptor Asmijon46No ratings yet
- Sertraline Enhances The Activity of AntimicrobialDocument8 pagesSertraline Enhances The Activity of Antimicrobialmijon46No ratings yet
- TAHONLAMA An Open Trial of Adjunctive Sertraline in TheDocument4 pagesTAHONLAMA An Open Trial of Adjunctive Sertraline in Themijon46No ratings yet
- Sertraline As An Add-On Treatment For DepressionDocument8 pagesSertraline As An Add-On Treatment For Depressionmijon46No ratings yet
- Sertraline Inhibits Nerve Growth Factor-Induced Neurite Outgrowth in PC12Document7 pagesSertraline Inhibits Nerve Growth Factor-Induced Neurite Outgrowth in PC12mijon46No ratings yet
- Effects of Sertraline and Fluoxetine On P-Glycoprotein atDocument6 pagesEffects of Sertraline and Fluoxetine On P-Glycoprotein atmijon46No ratings yet
- Population Pharmacokinetics of Sertraline in Healthy SubjectsDocument11 pagesPopulation Pharmacokinetics of Sertraline in Healthy Subjectsmijon46No ratings yet
- Effect of Polymorphisms On The Pharmacokinetics, Pharmacodynamics andDocument32 pagesEffect of Polymorphisms On The Pharmacokinetics, Pharmacodynamics andmijon46No ratings yet
- Clinical Pharmacokinetics of SertralineDocument20 pagesClinical Pharmacokinetics of Sertralinemijon46No ratings yet
- Experimental and Numerical Investigation of Rotating Bladed Disk Forced Response Using Under-Platform Friction DampersDocument11 pagesExperimental and Numerical Investigation of Rotating Bladed Disk Forced Response Using Under-Platform Friction DamperssenthilNo ratings yet
- Design Thinking Unit-1Document21 pagesDesign Thinking Unit-1Anshika BansalNo ratings yet
- Spectral Correlation of OFDM SignalsDocument6 pagesSpectral Correlation of OFDM Signalsazebshaikh3927No ratings yet
- 2023 - 002075129500001316312023 - Error CJALDocument7 pages2023 - 002075129500001316312023 - Error CJALFabian Quiroz VergelNo ratings yet
- Chapter 1 (Full) Introduction To MicroEconomicsDocument42 pagesChapter 1 (Full) Introduction To MicroEconomicsEida Hidayah100% (3)
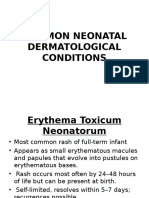
- Common Neonatal Dermatological ConditionsDocument27 pagesCommon Neonatal Dermatological ConditionsArslan SiddiquiNo ratings yet
- American Ceramic: SocietyDocument8 pagesAmerican Ceramic: SocietyPhi TiêuNo ratings yet
- Grade 10 Sasmo: secθ + tanθ = q, secθ q. q q q qDocument3 pagesGrade 10 Sasmo: secθ + tanθ = q, secθ q. q q q qAje GhazaNo ratings yet
- Chapter 05Document65 pagesChapter 05Tony DiPierryNo ratings yet
- Jamanisal 2015 4 1 5 PDFDocument7 pagesJamanisal 2015 4 1 5 PDFDuge AnggrainiNo ratings yet
- Vegetarian and Vegan Diets in Type 2 Diabetes ManagementDocument3 pagesVegetarian and Vegan Diets in Type 2 Diabetes Managementapi-259343531No ratings yet
- Emcee King & QueenDocument8 pagesEmcee King & QueenMaryHazelClaveBeniga100% (10)
- Chapter 5 - Strategic Human Resource ManagementDocument19 pagesChapter 5 - Strategic Human Resource ManagementmaiaaaaNo ratings yet
- 3 Affect Regulation, Mentalization, and The Development of The Self (Peter Fonagy, Gyorgy Gergely, Elliot L. Jurist Etc.) - 211-259Document49 pages3 Affect Regulation, Mentalization, and The Development of The Self (Peter Fonagy, Gyorgy Gergely, Elliot L. Jurist Etc.) - 211-259Sergio Andres Rico AvendanoNo ratings yet
- Volleyball BOTTOM LINE ESSAY TEMPLATEDocument2 pagesVolleyball BOTTOM LINE ESSAY TEMPLATEViness Pearl Kristina R. AcostoNo ratings yet
- Fitness To Work Offshore GuidelineDocument28 pagesFitness To Work Offshore GuidelineMohd Zaha Hisham100% (2)
- Core 13 UcspDocument3 pagesCore 13 UcspJanice DomingoNo ratings yet
- Find The Thévenin Equivalent With Respect To The 7k Ohm ResistorDocument27 pagesFind The Thévenin Equivalent With Respect To The 7k Ohm ResistorVipan SharmaNo ratings yet
- Tañada v. Angara Case DigestDocument12 pagesTañada v. Angara Case DigestKatrina PerezNo ratings yet
- Sacred SpaceDocument440 pagesSacred SpaceAbdiel Cervantes HernandezNo ratings yet
- GTU Affiliated L.D. College of Engineering Report on Online Hotel Management SystemDocument16 pagesGTU Affiliated L.D. College of Engineering Report on Online Hotel Management Systemyashvant thakkarNo ratings yet
- REduce BAil 22Document2 pagesREduce BAil 22Pboy SolanNo ratings yet
- Punjab govt grants EOL to doctors for postgraduate trainingDocument2 pagesPunjab govt grants EOL to doctors for postgraduate trainingMasroor HassanNo ratings yet
- Legal Counselling defined in broad and narrow sensesDocument5 pagesLegal Counselling defined in broad and narrow sensesRegie Rey AgustinNo ratings yet
- Amity School of Communication: BA (J&MC), Semester-1 Basics of Print Media Neha BhagatDocument10 pagesAmity School of Communication: BA (J&MC), Semester-1 Basics of Print Media Neha BhagatYash TiwariNo ratings yet
- ModernismDocument8 pagesModernismMariangela RizzoNo ratings yet
- English K 2 Multi Age Year A Unit 1Document46 pagesEnglish K 2 Multi Age Year A Unit 1celine celineNo ratings yet
- PROGRAMMING 11 - Q1 - W2 - Mod2 PDFDocument13 pagesPROGRAMMING 11 - Q1 - W2 - Mod2 PDFDianne Brucal - MatibagNo ratings yet
- How To Think Like A Professional TraderDocument7 pagesHow To Think Like A Professional TraderL100% (8)
- Labor Bar ExamDocument10 pagesLabor Bar Examcloudstorm-1No ratings yet