You might also like
- 1001 Common Words in OET Exam Mini-DictionaryDocument38 pages1001 Common Words in OET Exam Mini-DictionaryProsanjit Majumder94% (18)
- Matchstick MenDocument9 pagesMatchstick Menmichael_arnesonNo ratings yet
- PoikilocytosisDocument3 pagesPoikilocytosisJasonNo ratings yet
- Rapini DermatopatologíaDocument474 pagesRapini DermatopatologíadrNo ratings yet
- Project NewDocument33 pagesProject Newceeyem83% (12)
- RBC DisordersDocument8 pagesRBC DisordersDavid JohnNo ratings yet
- Anemia Differential Diagnosis : Microcytic Normocytic MacrocyticDocument1 pageAnemia Differential Diagnosis : Microcytic Normocytic Macrocyticمحمد عقيلي100% (1)
- Systematic Approach in Anemia Evaluation and Review of Peripheral SmearsDocument72 pagesSystematic Approach in Anemia Evaluation and Review of Peripheral SmearsSukma Eka PratiwiNo ratings yet
- Anemia SDocument8 pagesAnemia SCarlo SantosNo ratings yet
- RED CELL MORPHOLOGY Tabulation SummaryDocument6 pagesRED CELL MORPHOLOGY Tabulation SummaryStephen YorNo ratings yet
- Basic HematologyDocument69 pagesBasic HematologyDimas Bayu FirdausNo ratings yet
- Overview of AnaemiaDocument2 pagesOverview of AnaemiaGerardLumNo ratings yet
- Reticulocyte Count: Esr: RBC Count: Reticulocyte Count: Low For Reticulocyte Count: Platelet Count: Packed Reticulocyte CountDocument3 pagesReticulocyte Count: Esr: RBC Count: Reticulocyte Count: Low For Reticulocyte Count: Platelet Count: Packed Reticulocyte CountVarshaa BharathiNo ratings yet
- Blood FilmDocument2 pagesBlood FilmGerardLum100% (1)
- RBC ANOMALIES AND INCLUSIONS With Their Associated DiseasesDocument2 pagesRBC ANOMALIES AND INCLUSIONS With Their Associated DiseasesCamella Beatrice Lujan ValleNo ratings yet
- Hematology 101: Interpreting Lab Results - Patterns and PitfallsDocument55 pagesHematology 101: Interpreting Lab Results - Patterns and PitfallsAmorrita Puspita Ratu100% (1)
- Anemia TutoringDocument28 pagesAnemia TutoringngNo ratings yet
- Poikilocytosis Review TableDocument5 pagesPoikilocytosis Review Tablekat100% (1)
- TrW-Guwv 0g VwhuPGl65PBCquGkt3j5Document65 pagesTrW-Guwv 0g VwhuPGl65PBCquGkt3j5Shikhar MishraNo ratings yet
- Approach To Anemia: - Reticulocyte Count Is Most Important TestDocument15 pagesApproach To Anemia: - Reticulocyte Count Is Most Important TestJanella SuerteNo ratings yet
- Degenevie - HematologyDocument71 pagesDegenevie - Hematologykkq7fhkwvkNo ratings yet
- Cara Mendiagnose AnemiaDocument1 pageCara Mendiagnose AnemiaMuchlissatus Lisa MedicalbookNo ratings yet
- Amboss Hemolytic AnemiaDocument16 pagesAmboss Hemolytic AnemiaAhmed Ali100% (2)
- Clinical Haematology-Lecture SlidesDocument55 pagesClinical Haematology-Lecture SlidesShiv Sookun100% (1)
- Red and White Blood Cell DisordersDocument11 pagesRed and White Blood Cell DisordersVittorio Di PaoloNo ratings yet
- Microcytic anaemia types and causesDocument7 pagesMicrocytic anaemia types and causesJason AnthonyNo ratings yet
- Clinical Pathology CBC GuideDocument38 pagesClinical Pathology CBC Guideyeshitla amsaluNo ratings yet
- Zako HematologyDocument35 pagesZako Hematologydoctormehmeteren8292No ratings yet
- An Approach To Anemia: Brad Lewis Director Hematology San Francisco General HospitalDocument47 pagesAn Approach To Anemia: Brad Lewis Director Hematology San Francisco General HospitalyapponNo ratings yet
- Anemia Workup - Approach Considerations, Investigation For Pathogenesis, Evaluation For Blood LossDocument14 pagesAnemia Workup - Approach Considerations, Investigation For Pathogenesis, Evaluation For Blood LossRahul SahadevanNo ratings yet
- 9 Hema Extrinsic RBC DefectsDocument2 pages9 Hema Extrinsic RBC DefectsGwen Kirsten AtayanNo ratings yet
- Anemia - AMBOSSDocument2 pagesAnemia - AMBOSStgayuNo ratings yet
- Anemia OutlineDocument3 pagesAnemia Outlinekaylakmills_10135868No ratings yet
- AnaemiaDocument7 pagesAnaemiaYousef El3alameyNo ratings yet
- Update On (Approach To) AnemiaDocument44 pagesUpdate On (Approach To) AnemiaIsaac MwangiNo ratings yet
- Anemia BloodDocument29 pagesAnemia BloodDalia EzzeddineNo ratings yet
- Hematology: Presented by Alyazeed Hussein, BSCDocument96 pagesHematology: Presented by Alyazeed Hussein, BSCMONFOLANo ratings yet
- Week 4 - HandoutDocument4 pagesWeek 4 - Handoutjess waldenNo ratings yet
- Patho HematologyDocument39 pagesPatho HematologyCastleKGNo ratings yet
- Anemia in Children: Causes, Types and TreatmentDocument61 pagesAnemia in Children: Causes, Types and TreatmentSamuel ManurungNo ratings yet
- Anemia - AmbossDocument10 pagesAnemia - AmbossGuga XachidzeNo ratings yet
- RBC anomalies-ANEMIADocument19 pagesRBC anomalies-ANEMIAJeremiahNo ratings yet
- Hema 2 Prelims MergedDocument26 pagesHema 2 Prelims MergedMYLENE POSTREMONo ratings yet
- Hematology 2 PrelimsDocument17 pagesHematology 2 PrelimsMYLENE POSTREMONo ratings yet
- Diagnosis Laboratorium ThalassemiaDocument36 pagesDiagnosis Laboratorium ThalassemiairanifianzaNo ratings yet
- RBC Morphology and InclusionsDocument3 pagesRBC Morphology and InclusionsDeomicah SolanoNo ratings yet
- AnemiaDocument2 pagesAnemiaRed DiggerNo ratings yet
- Physiology Lab V2Document14 pagesPhysiology Lab V2Mohammed EljackNo ratings yet
- Super Simplified Pathology Hematology - Dr. Priyanka SachdevDocument500 pagesSuper Simplified Pathology Hematology - Dr. Priyanka SachdevMohd SaquibNo ratings yet
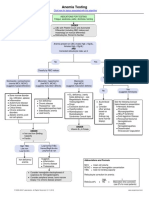
- Anemia Testing Algorithm PDFDocument1 pageAnemia Testing Algorithm PDFBilly AuNo ratings yet
- Anemia Testing Algorithm PDFDocument1 pageAnemia Testing Algorithm PDFkatNo ratings yet
- Anemia Flow ChartDocument1 pageAnemia Flow ChartCynthiaNo ratings yet
- AnaemiaDocument83 pagesAnaemiadoc19019696No ratings yet
- 20.guidelines AnaemiaDocument5 pages20.guidelines AnaemiaRed DevilNo ratings yet
- Intravascular Extravascular: Fe Storage Tibc SerumDocument2 pagesIntravascular Extravascular: Fe Storage Tibc Serumazhar hussinNo ratings yet
- Clinical Approach: Anemia in ChildhoodDocument30 pagesClinical Approach: Anemia in ChildhoodYuffaa AinayyaaNo ratings yet
- Hematology: AnemiaDocument46 pagesHematology: AnemiaCyrus100% (1)
- Undergraduates—Medicine: Diagnosing Megaloblastic AnemiasDocument30 pagesUndergraduates—Medicine: Diagnosing Megaloblastic AnemiasAishwarya JeeNo ratings yet
- Fast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaFrom EverandFast Facts: Leucemia: Desde la mutación genética inicial hasta el apoyo para la supervivenciaNo ratings yet
- Basic Needs and Comfort MeasuresDocument73 pagesBasic Needs and Comfort MeasuresProsanjit MajumderNo ratings yet
- Pain ManagementDocument20 pagesPain ManagementProsanjit MajumderNo ratings yet
- Ielts & Toefl: Vocabulary Master ClassDocument18 pagesIelts & Toefl: Vocabulary Master ClassProsanjit MajumderNo ratings yet
- IELTS & TOEFL Vocabulary Master Class: 900+ Words to Boost Your ScoreDocument39 pagesIELTS & TOEFL Vocabulary Master Class: 900+ Words to Boost Your ScoreProsanjit Majumder0% (1)
- FWZ© Weáwß: Gv÷Vi Ae Cvewjk NJDocument3 pagesFWZ© Weáwß: Gv÷Vi Ae Cvewjk NJProsanjit MajumderNo ratings yet
- HR Specialist's ResumeDocument1 pageHR Specialist's ResumeProsanjit MajumderNo ratings yet
- FWZ© Weáwß: Gv÷Vi Ae Cvewjk NJDocument3 pagesFWZ© Weáwß: Gv÷Vi Ae Cvewjk NJProsanjit MajumderNo ratings yet
- Basic Science: Introduction To Science of BIOLOGYDocument5 pagesBasic Science: Introduction To Science of BIOLOGYProsanjit MajumderNo ratings yet
- Blood Supply of Whole BodyDocument60 pagesBlood Supply of Whole BodyProsanjit Majumder100% (1)
- Candidate Guide To MRCS Examination July2018 PDFDocument51 pagesCandidate Guide To MRCS Examination July2018 PDFBakri MustafaNo ratings yet
- Introduction To Pediatric NursingDocument4 pagesIntroduction To Pediatric NursingProsanjit MajumderNo ratings yet
- Speaking Sub-Test Overview PDFDocument10 pagesSpeaking Sub-Test Overview PDFProsanjit MajumderNo ratings yet
- 100 Cases in General Practice 1st PDFDocument224 pages100 Cases in General Practice 1st PDFfunandlearningNo ratings yet
- Cell Biology Lecture Notes ExplainedDocument108 pagesCell Biology Lecture Notes ExplainedpandaprasadNo ratings yet
- Roleplay Tasks PDFDocument5 pagesRoleplay Tasks PDFProsanjit MajumderNo ratings yet
- Roleplay Tasks PDFDocument5 pagesRoleplay Tasks PDFProsanjit MajumderNo ratings yet
- ABC of ICU by Mansdocs PDFDocument62 pagesABC of ICU by Mansdocs PDFProsanjit MajumderNo ratings yet
- Writing Assessment Criteria & FormatDocument15 pagesWriting Assessment Criteria & FormatProsanjit Majumder100% (1)
- Study Tips and Skill BuildingDocument6 pagesStudy Tips and Skill BuildingProsanjit MajumderNo ratings yet
- Writing Difficult Words-1Document11 pagesWriting Difficult Words-1Prosanjit Majumder100% (1)
- Medical Health Manager Job ApplicationDocument1 pageMedical Health Manager Job ApplicationProsanjit MajumderNo ratings yet
- English Grammar SecretsDocument66 pagesEnglish Grammar SecretsMbatutes94% (33)
- Pedi NotesDocument49 pagesPedi NotesProsanjit MajumderNo ratings yet
- Paracetamol Drug StudyDocument5 pagesParacetamol Drug StudyMatty Jolbitado50% (2)
- Problem TreeDocument1 pageProblem Treeyel5buscatoNo ratings yet
- ChlorphromazineDocument2 pagesChlorphromazineanreilegardeNo ratings yet
- 22 Phil 227 Bagtas Vs PaguioDocument4 pages22 Phil 227 Bagtas Vs PaguioGina Portuguese GawonNo ratings yet
- Sign Symptoms Ketoacidosis DiabeticDocument4 pagesSign Symptoms Ketoacidosis DiabeticMatthew NathanielNo ratings yet
- Geria ReviewerDocument2 pagesGeria ReviewerbillyktoubattsNo ratings yet
- Preoperative Assess Prep in AnesthesiaDocument26 pagesPreoperative Assess Prep in AnesthesiaShimmering MoonNo ratings yet
- ALBINISMDocument3 pagesALBINISMLawrence CezarNo ratings yet
- Rajinikanth: "Rajini" Redirects Here. For Other Uses, SeeDocument15 pagesRajinikanth: "Rajini" Redirects Here. For Other Uses, SeeArun SekarNo ratings yet
- Factors That Affect Physical DevelopmentDocument4 pagesFactors That Affect Physical DevelopmentmomuNo ratings yet
- Herbarium of IndiaDocument7 pagesHerbarium of IndiaStephanie MooreNo ratings yet
- Final Assessment Report Allium Sativum L Bulbus - enDocument90 pagesFinal Assessment Report Allium Sativum L Bulbus - enWidiyastuti DarwisNo ratings yet
- What Is Polio?: SymptomsDocument2 pagesWhat Is Polio?: SymptomsJP LandagoraNo ratings yet
- Acute Bronchitis Case StudyDocument6 pagesAcute Bronchitis Case Studyulka0750% (2)
- NBME Form 1 Step 2 ReviewDocument77 pagesNBME Form 1 Step 2 Reviewalex karevNo ratings yet
- Pneumokokus Dan Penyakit Pneumokokus - Ari PrayitnoDocument36 pagesPneumokokus Dan Penyakit Pneumokokus - Ari PrayitnoIndri MmrNo ratings yet
- High Prevalence of Obstructive Sleep Apnea Among People With Type 2 Diabetes Mellitus in A Tertiary Care CenterDocument5 pagesHigh Prevalence of Obstructive Sleep Apnea Among People With Type 2 Diabetes Mellitus in A Tertiary Care CenterPcrNo ratings yet
- Best ENT Surgeon in Hyderabad - ENT HospitalDocument14 pagesBest ENT Surgeon in Hyderabad - ENT HospitalMagnasVNo ratings yet
- Rare blistering skin condition linked to gluten intoleranceDocument2 pagesRare blistering skin condition linked to gluten intoleranceCharticha PatrisindryNo ratings yet
- Ginger ArticleDocument17 pagesGinger ArticleDr-Aftab Ahmed KhanNo ratings yet
- Zuku Visual Flashnotes Distemper ExtendedDocument4 pagesZuku Visual Flashnotes Distemper ExtendedShubham HarishNo ratings yet
- SIP On Essential OilsDocument17 pagesSIP On Essential OilsJessa Marie SuarezNo ratings yet
- The Wonder of Herbs To Treat-AlopeciaDocument7 pagesThe Wonder of Herbs To Treat-AlopeciaLuca JohnNo ratings yet
- Practice Bulletin ACOG Antibiotic Prophylaxis For LabourDocument12 pagesPractice Bulletin ACOG Antibiotic Prophylaxis For LabourLorenzo TzuNo ratings yet
- Reversibledementias: Milta O. LittleDocument26 pagesReversibledementias: Milta O. LittleLUCAS IGNACIO SANCHEZNo ratings yet
- Pharm Quiz 1Document59 pagesPharm Quiz 1Anonymous vXOM1Wxt100% (1)
- Audit Worksheet PDFDocument1 pageAudit Worksheet PDFAgnelNo ratings yet