You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- M05 Writing Case Study 1 - BrandyDocument6 pagesM05 Writing Case Study 1 - BrandyMad MaximusNo ratings yet
- Cardio WorkbookDocument5 pagesCardio WorkbookZhy Caluza100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Final-Exam Neurosurgery - 2-VersionDocument6 pagesFinal-Exam Neurosurgery - 2-VersionMAMA LALANo ratings yet
- DM Case Study Question and AnswerDocument3 pagesDM Case Study Question and AnswerscribdfrydNo ratings yet
- Prof Prac Correl Reviewer PDFDocument22 pagesProf Prac Correl Reviewer PDFMara Benzon-Barrientos100% (1)
- SPP NotesDocument3 pagesSPP NotesMara Benzon-BarrientosNo ratings yet
- Prac Correlx PDFDocument14 pagesPrac Correlx PDFMara Benzon-BarrientosNo ratings yet
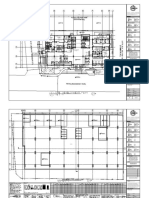
- 2019-0215-Hmi DD A1000-Floor PlansDocument16 pages2019-0215-Hmi DD A1000-Floor PlansMara Benzon-BarrientosNo ratings yet
- Current Sanitation Practices in The Philippines (Final)Document7 pagesCurrent Sanitation Practices in The Philippines (Final)Mara Benzon-BarrientosNo ratings yet
- Non Alcoholic Liver Disease PhilippinesDocument5 pagesNon Alcoholic Liver Disease PhilippinesMara Benzon-BarrientosNo ratings yet
- 2016 - Philippine Health StatisticsDocument223 pages2016 - Philippine Health StatisticsMara Benzon-BarrientosNo ratings yet
- 3 Heart Diseases: and How Knowing The Differences Can Help Save A LifeDocument15 pages3 Heart Diseases: and How Knowing The Differences Can Help Save A LifeMara Benzon-BarrientosNo ratings yet
- Per Capita Budget For Meal Provision of Patients2 PDFDocument30 pagesPer Capita Budget For Meal Provision of Patients2 PDFMara Benzon-BarrientosNo ratings yet
- Sample Gen HospDocument94 pagesSample Gen HospMara Benzon-BarrientosNo ratings yet
- Thesis Title DefenseDocument10 pagesThesis Title DefenseMara Benzon-BarrientosNo ratings yet
- HSP PDFDocument1 pageHSP PDFMara Benzon-BarrientosNo ratings yet
- NCM 117 Midterm ReviewerDocument17 pagesNCM 117 Midterm ReviewerPia Rose RoqueNo ratings yet
- ACLS HandoutsDocument4 pagesACLS HandoutshasanNo ratings yet
- Botulism As A Bioterrorism AgentDocument24 pagesBotulism As A Bioterrorism AgentFabián FernándezNo ratings yet
- Streptococcus: PneumoniaeDocument12 pagesStreptococcus: PneumoniaeZeth MoturiNo ratings yet
- Food HygieneDocument31 pagesFood Hygienehemihema100% (1)
- Science Lesson PlanDocument5 pagesScience Lesson Planapi-242843832No ratings yet
- Inflammatory Cytokine Response in Patients With Septic Shock Secondary To Generalized PeritonitisDocument9 pagesInflammatory Cytokine Response in Patients With Septic Shock Secondary To Generalized PeritonitisFerdian PriantoNo ratings yet
- Cva Case StudyDocument31 pagesCva Case StudyZoe AnnaNo ratings yet
- Postpartum QuestionsDocument2 pagesPostpartum QuestionsRayMendez100% (4)
- Cefoxitin Drug StudyDocument1 pageCefoxitin Drug StudyArthur Christopher CorpuzNo ratings yet
- Blood Culture TestDocument15 pagesBlood Culture TestNimra IqbalNo ratings yet
- AntipsychoticsDocument22 pagesAntipsychoticsDaniyal AhmedNo ratings yet
- Ischemic Stroke in Young AdultDocument26 pagesIschemic Stroke in Young AdultBill Jones TanawalNo ratings yet
- Which of The Two Is More Liver Specific and Increases More During Liver DiseaseDocument8 pagesWhich of The Two Is More Liver Specific and Increases More During Liver DiseaseMariel AbatayoNo ratings yet
- Oxaliplatin Monograph 1dec2016Document9 pagesOxaliplatin Monograph 1dec2016Nadial UzmahNo ratings yet
- Rheumatoid ArthritisDocument4 pagesRheumatoid ArthritisFreeNursingNotes100% (1)
- Amantadine HCLDocument4 pagesAmantadine HCLMae Ann Bueno CastillonNo ratings yet
- Emergency NursingDocument5 pagesEmergency NursingRoAn DulayNo ratings yet
- PAROS (Case 3)Document2 pagesPAROS (Case 3)Carl Michael RazoNo ratings yet
- PONSTAN® Capsules: What Is in This LeafletDocument4 pagesPONSTAN® Capsules: What Is in This LeafletLee Hye RiNo ratings yet
- Fibroadenoma Mammae of The BreastDocument15 pagesFibroadenoma Mammae of The Breastirvanie100% (1)
- Health Vocabulary ListDocument7 pagesHealth Vocabulary ListClaudia MacarieNo ratings yet
- Notes On Cancer (Class XII)Document2 pagesNotes On Cancer (Class XII)Aryan JaiswalNo ratings yet
- DRUG STUDY (Lung Cancer)Document10 pagesDRUG STUDY (Lung Cancer)Jobelle AcenaNo ratings yet
- What Is Diaper RashDocument6 pagesWhat Is Diaper RashshirlyneappledeleonNo ratings yet
- Fever Is Not A Contraindication For A - 2015 - Australasian Emergency Nursing JDocument1 pageFever Is Not A Contraindication For A - 2015 - Australasian Emergency Nursing JIván del Crísto Guerra CamargoNo ratings yet