You might also like
- Complementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)From EverandComplementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)No ratings yet
- Marina Eloi, Daniela Vargas Horvath, João Carlos Ortega, Monica Simon Prado, Luis Eduardo Coelho Andrade, Et AlDocument2 pagesMarina Eloi, Daniela Vargas Horvath, João Carlos Ortega, Monica Simon Prado, Luis Eduardo Coelho Andrade, Et AlSitha WisesaNo ratings yet
- s 1368980016000409 ADocument11 pagess 1368980016000409 Atihemex618No ratings yet
- Association Between Vitamin D Levels and Allergy-Related Outcomes Vary by Race and Other FactorsDocument10 pagesAssociation Between Vitamin D Levels and Allergy-Related Outcomes Vary by Race and Other FactorsErnest Ang GrekNo ratings yet
- Higher Cord Blood 25-Hydroxyvitamin D - Fix - LGDocument44 pagesHigher Cord Blood 25-Hydroxyvitamin D - Fix - LGchkdnshNo ratings yet
- Can Vitamin D Status Be Assessed by Serum 25OHD in Children2015Document7 pagesCan Vitamin D Status Be Assessed by Serum 25OHD in Children2015Sheyla Alegre ParionaNo ratings yet
- Wang 2015Document10 pagesWang 2015Andana TrisaviNo ratings yet
- Research Article: Fall in Vitamin D Levels During Hospitalization in ChildrenDocument7 pagesResearch Article: Fall in Vitamin D Levels During Hospitalization in ChildrenAMALIA RAMADANINo ratings yet
- Longitudinal Vitamin D Status in Pregnancy and The Risk of Pre-EclampsiaDocument8 pagesLongitudinal Vitamin D Status in Pregnancy and The Risk of Pre-EclampsiaBima Bayu PutraNo ratings yet
- Vit D and Risk FactorDocument6 pagesVit D and Risk FactorRatnaNo ratings yet
- Acute Respiratory Tract Infection and Hydroxyvitamin D Concentration: A Systematic Review and Meta-AnalysisDocument15 pagesAcute Respiratory Tract Infection and Hydroxyvitamin D Concentration: A Systematic Review and Meta-AnalysisCesar AlejandroNo ratings yet
- EBM TerbaruDocument5 pagesEBM TerbaruTetty PrasetyaNo ratings yet
- Risk Factors of Vitamin D Deficiency in Children With Epilepsy Taking Anticonvulsants at Initial and During Follow-UpDocument12 pagesRisk Factors of Vitamin D Deficiency in Children With Epilepsy Taking Anticonvulsants at Initial and During Follow-UpSari MustikaNo ratings yet
- Letters To The Editor: Baseline Characteristics Steroid Group (N 5 24) Steroid 1 D3 Group (N 5 24)Document3 pagesLetters To The Editor: Baseline Characteristics Steroid Group (N 5 24) Steroid 1 D3 Group (N 5 24)Giuliana ReyesNo ratings yet
- Apem 20 198Document8 pagesApem 20 198Sari MustikaNo ratings yet
- Ajcn115105 PDFDocument8 pagesAjcn115105 PDFAnonimNo ratings yet
- Vitamin D Levels in Children Diagnosed With Acute Otitis MediaDocument5 pagesVitamin D Levels in Children Diagnosed With Acute Otitis MediamuthiafadhilahNo ratings yet
- Relationship between 25-Hydroxy Vitamin D Levels and Type of Morbus HansenDocument7 pagesRelationship between 25-Hydroxy Vitamin D Levels and Type of Morbus HansenLidia MdNo ratings yet
- Lower Vitamin D Levels Are Associated With Increased Risk of Early-Onset Neonatal Sepsis in Term InfantsDocument7 pagesLower Vitamin D Levels Are Associated With Increased Risk of Early-Onset Neonatal Sepsis in Term InfantsMohamed Abo SeifNo ratings yet
- Vitamin D Effects in Atopic Dermatitis: A B A B A D C, e BDocument7 pagesVitamin D Effects in Atopic Dermatitis: A B A B A D C, e Bmasayuki haradaNo ratings yet
- 4071-Published Article Text-27248-2-10-20200718Document5 pages4071-Published Article Text-27248-2-10-20200718Berry BancinNo ratings yet
- The Use of The 25 (OH) D Saliva Test As A Substitute For The 25 (OH) D Serum Test in Healthy PeopleDocument15 pagesThe Use of The 25 (OH) D Saliva Test As A Substitute For The 25 (OH) D Serum Test in Healthy PeopleRomina DatuNo ratings yet
- Low Serum 25-Hydroxyvitamin D Concentrations Are Associated With Increased Likelihood of Having Depressive Symptoms Among Japanese WorkersDocument2 pagesLow Serum 25-Hydroxyvitamin D Concentrations Are Associated With Increased Likelihood of Having Depressive Symptoms Among Japanese WorkersfricotalumewoNo ratings yet
- Translate Vit DDocument3 pagesTranslate Vit DErvin MaulanaNo ratings yet
- Vit D X Risco CardiovascularDocument7 pagesVit D X Risco CardiovascularAlberto Frazão Treinador & NutricionistaNo ratings yet
- Association of Vitamin D Level With Alopecia Areata: BackgroundDocument5 pagesAssociation of Vitamin D Level With Alopecia Areata: Backgroundrandy_suryawan_No ratings yet
- Vitamin D Pada Anak EpilepsiDocument7 pagesVitamin D Pada Anak EpilepsiMad MadNo ratings yet
- Oleh Ilham Syifaur Pembimbing Dr. Rahmad Syuhada, Sp. MDocument20 pagesOleh Ilham Syifaur Pembimbing Dr. Rahmad Syuhada, Sp. MMeta MedianaNo ratings yet
- Pdia 34 29509Document4 pagesPdia 34 29509Fi NoNo ratings yet
- Artikel 2Document7 pagesArtikel 2Claudia BuheliNo ratings yet
- Assay-Specific Differences in Lipemic InterferenceDocument5 pagesAssay-Specific Differences in Lipemic InterferenceDaniel Huachani CoripunaNo ratings yet
- Nutrients 07 03427Document22 pagesNutrients 07 03427Nurfadhilah YusufNo ratings yet
- Association of Antioxidants and Vitamin D Level With Inflammation in Children With Atopic DermatitisDocument6 pagesAssociation of Antioxidants and Vitamin D Level With Inflammation in Children With Atopic DermatitisaditiarrtuguNo ratings yet
- 379 716 1 SMDocument10 pages379 716 1 SMRahmini RangkutiNo ratings yet
- Vitamin D levels in follicular fluid and ART outcomesDocument6 pagesVitamin D levels in follicular fluid and ART outcomesMaria RoxanaNo ratings yet
- Jcrpe 1 266Document5 pagesJcrpe 1 266ASADNo ratings yet
- Journal of Reproductive Immunology: ArticleinfoDocument7 pagesJournal of Reproductive Immunology: ArticleinfoinayahsyNo ratings yet
- Vitamin D and Telomerase 6Document4 pagesVitamin D and Telomerase 6Muhammad AL Farisi SutrisnoNo ratings yet
- Nutrients: Vitamin D and Graves' Disease: A Meta-Analysis UpdateDocument15 pagesNutrients: Vitamin D and Graves' Disease: A Meta-Analysis Updatedebby claudiNo ratings yet
- Prenatal, Perinatal, and Childhood Vitamin D Exposure and Their Association With Childhood Allergic Rhinitis and Allergic SensitizationDocument10 pagesPrenatal, Perinatal, and Childhood Vitamin D Exposure and Their Association With Childhood Allergic Rhinitis and Allergic SensitizationAnasthasia hutagalungNo ratings yet
- A Study of Vitamin - D Status in Epileptic Children in Age Group of 2-15 YearsDocument5 pagesA Study of Vitamin - D Status in Epileptic Children in Age Group of 2-15 YearsRatnaNo ratings yet
- Association of Thrombotic Markers With Severity of Pediatric-Onset Systemic Lupus ErythematosusDocument3 pagesAssociation of Thrombotic Markers With Severity of Pediatric-Onset Systemic Lupus Erythematosusalfaz zamzamiNo ratings yet
- Nicu 1Document7 pagesNicu 1PPDS ANAK FK USUNo ratings yet
- Psoriasis y Vitamina DDocument11 pagesPsoriasis y Vitamina DGaviota75No ratings yet
- Infant Vit D PakistanDocument4 pagesInfant Vit D PakistanAleem MuhammadNo ratings yet
- Vitamin D in Human Reproduction - Some Answers and Many More QuestionsDocument2 pagesVitamin D in Human Reproduction - Some Answers and Many More QuestionsjuanNo ratings yet
- Antibiotik THT FixDocument3 pagesAntibiotik THT FixIda LailaNo ratings yet
- Valproic Acid Therapy Decreases Serum 25-Hydroxyvitamin D Level in Female Infants and Toddlers With Epilepsy - A Pilot Longitudinal StudyDocument7 pagesValproic Acid Therapy Decreases Serum 25-Hydroxyvitamin D Level in Female Infants and Toddlers With Epilepsy - A Pilot Longitudinal StudyAnna FlorentinaNo ratings yet
- Vitamin D Insufficiency Linked To Asthma Severity: Medscape Medical NewsDocument6 pagesVitamin D Insufficiency Linked To Asthma Severity: Medscape Medical NewsMichal MajewskiNo ratings yet
- Fendo 13 920340Document10 pagesFendo 13 920340iam_ca2No ratings yet
- Congenital Cardiology SolutionsDocument1 pageCongenital Cardiology SolutionsSherZalattha KuchikiElfNo ratings yet
- The Impact of Vitamin D On The Innate Immune Response To Uropathogenic Escherichia Coli During PregnancyDocument7 pagesThe Impact of Vitamin D On The Innate Immune Response To Uropathogenic Escherichia Coli During PregnancyfinaNo ratings yet
- Selenio e Ovario PolicisticoDocument6 pagesSelenio e Ovario PolicisticoprofnutrialecuriNo ratings yet
- Inhaled Nitric Oxide For Respiratory Failure in Preterm InfantsDocument3 pagesInhaled Nitric Oxide For Respiratory Failure in Preterm InfantsAlvin Brilian BudionoNo ratings yet
- Prenatal Vitamin D Reduces Risk of AshtmaDocument15 pagesPrenatal Vitamin D Reduces Risk of AshtmaKerlyn GuerraNo ratings yet
- Enteral Vitamin A For Reducing Severity of Bronchopulmonary Dysplasia: A Randomized TrialDocument12 pagesEnteral Vitamin A For Reducing Severity of Bronchopulmonary Dysplasia: A Randomized Triallaurencia aliminNo ratings yet
- Vitamin D Sufficiency Through Sunshine in Infants?: Editorial Editorial Editorial Editorial EditorialDocument2 pagesVitamin D Sufficiency Through Sunshine in Infants?: Editorial Editorial Editorial Editorial EditorialMuhammad RamadhanNo ratings yet
- L-Arginine and Vitamin D Adjunctive Therapies in Pulmonary Tuberculosis: A Randomised, Double-Blind, Placebo-Controlled TrialDocument12 pagesL-Arginine and Vitamin D Adjunctive Therapies in Pulmonary Tuberculosis: A Randomised, Double-Blind, Placebo-Controlled TrialDivaa OktavianitaNo ratings yet
- Relationship between vitamin D deficiency, inflammation and preeclampsiaDocument7 pagesRelationship between vitamin D deficiency, inflammation and preeclampsiaronny29No ratings yet
- Sleep Disordered Breathing in Bronchopulmonary DysplasiaDocument9 pagesSleep Disordered Breathing in Bronchopulmonary DysplasiaJHONATAN MATA ARANDANo ratings yet
- Lung Ultrasound For The Cardiologist PDFDocument14 pagesLung Ultrasound For The Cardiologist PDFraul zea calcinaNo ratings yet
- Bab 3Document18 pagesBab 3Calvin Tanuwijaya Stick BolaNo ratings yet
- Bab 1 PendahuluanDocument2 pagesBab 1 PendahuluanCalvin Tanuwijaya Stick BolaNo ratings yet
- Bab 2Document4 pagesBab 2Calvin Tanuwijaya Stick BolaNo ratings yet
- Bab 4Document3 pagesBab 4Calvin Tanuwijaya Stick BolaNo ratings yet
- VM in BpocDocument19 pagesVM in BpocAndreea Livia DumitrescuNo ratings yet
- An Open-Label Pilot Study of Adrenocorticotrophic Hormone in The Treatment of IgA Nephropathy at High Risk of Progression Zand2019Document8 pagesAn Open-Label Pilot Study of Adrenocorticotrophic Hormone in The Treatment of IgA Nephropathy at High Risk of Progression Zand2019Calvin Tanuwijaya Stick BolaNo ratings yet
- Bab 4Document3 pagesBab 4Calvin Tanuwijaya Stick BolaNo ratings yet
- Bab 3Document18 pagesBab 3Calvin Tanuwijaya Stick BolaNo ratings yet
- Bab 1 PendahuluanDocument2 pagesBab 1 PendahuluanCalvin Tanuwijaya Stick BolaNo ratings yet
- Bab 3Document18 pagesBab 3Calvin Tanuwijaya Stick BolaNo ratings yet
- 9288 30346 1 PBDocument17 pages9288 30346 1 PBZulhartoni ToniNo ratings yet
- Bab 4Document3 pagesBab 4Calvin Tanuwijaya Stick BolaNo ratings yet
- Pie DiagramDocument1 pagePie DiagramCalvin Tanuwijaya Stick BolaNo ratings yet
- Chart Title: More Frequent Use of Multimedia After COVID-19 PandemicDocument1 pageChart Title: More Frequent Use of Multimedia After COVID-19 PandemicCalvin Tanuwijaya Stick BolaNo ratings yet
- Graph AllDocument1 pageGraph AllCalvin Tanuwijaya Stick BolaNo ratings yet
- Trautmann2020 Article IPNAClinicalPracticeRecommendaDocument33 pagesTrautmann2020 Article IPNAClinicalPracticeRecommendaAna-Mihaela BalanuțaNo ratings yet
- Role of Inflammation in The Pathogenesis and Treatment of Fibromyalgia (2019) PDFDocument11 pagesRole of Inflammation in The Pathogenesis and Treatment of Fibromyalgia (2019) PDFBecados PsiquiatriaNo ratings yet
- Transfer Patient Covid PDFDocument29 pagesTransfer Patient Covid PDFCalvin Tanuwijaya Stick BolaNo ratings yet
- Anestesi Pada Penyakit GinjalDocument16 pagesAnestesi Pada Penyakit GinjalCalvin Tanuwijaya Stick BolaNo ratings yet
- Autonomic Neuroscience: Basic and Clinical: Jose-Alberto Palma, Lucy Norcli Ffe-Kaufmann, Horacio KaufmannDocument11 pagesAutonomic Neuroscience: Basic and Clinical: Jose-Alberto Palma, Lucy Norcli Ffe-Kaufmann, Horacio KaufmannCalvin Tanuwijaya Stick BolaNo ratings yet
- Autonomic Neuroscience: Basic and Clinical: Jose-Alberto Palma, Lucy Norcli Ffe-Kaufmann, Horacio KaufmannDocument11 pagesAutonomic Neuroscience: Basic and Clinical: Jose-Alberto Palma, Lucy Norcli Ffe-Kaufmann, Horacio KaufmannCalvin Tanuwijaya Stick BolaNo ratings yet
- Pengantar Toksikologi Dan ToxindromeDocument29 pagesPengantar Toksikologi Dan ToxindromeCalvin Tanuwijaya Stick BolaNo ratings yet
- Physical Education: Module 7: Designing Your Own Exercise ProgramDocument6 pagesPhysical Education: Module 7: Designing Your Own Exercise ProgramColleen CastueraNo ratings yet
- The Use of Isotretinoin in AcneDocument8 pagesThe Use of Isotretinoin in AcneMelisa Silvia SembiringNo ratings yet
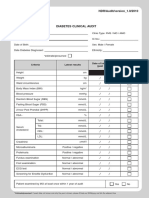
- Borang Diabetes Clinical AuditDocument2 pagesBorang Diabetes Clinical AuditHafizzah Mohd FirdausNo ratings yet
- Laboratory ManagementDocument6 pagesLaboratory ManagementJamille CarayuganNo ratings yet
- DownloadDocument6 pagesDownloadDoraNo ratings yet
- Paleco Safety PlanDocument17 pagesPaleco Safety PlanBobomo PoNo ratings yet
- JW English PDFDocument84 pagesJW English PDFIrma NosadseNo ratings yet
- 2022 Tribal HHAP Application - 22Document7 pages2022 Tribal HHAP Application - 22LakeCoNewsNo ratings yet
- Osce Notes For Psychiatry GXDocument52 pagesOsce Notes For Psychiatry GXtarshaNo ratings yet
- (PPT) DPC 1.4.1 Periodic Health Examination - Dr. ZuluetaDocument28 pages(PPT) DPC 1.4.1 Periodic Health Examination - Dr. ZuluetaJennifer Pisco LiracNo ratings yet
- Topics For Possible ResearchDocument2 pagesTopics For Possible ResearchJinny Mae Jacenth GardoseNo ratings yet
- PHSA Brigada Sining Proposal To LBDocument10 pagesPHSA Brigada Sining Proposal To LBlaurenceNo ratings yet
- Learning Feedback Diary (LFD) : General ObjectiveDocument3 pagesLearning Feedback Diary (LFD) : General ObjectiveAlhadzra AlihNo ratings yet
- Step 3 Form 3 CorrectedDocument41 pagesStep 3 Form 3 CorrectedSBG BPT100% (2)
- Medical School Pediatric Department Chairs, Inc.: Notes From The Association ofDocument4 pagesMedical School Pediatric Department Chairs, Inc.: Notes From The Association ofChristian NaranjoNo ratings yet
- Flexible Thermoplastic Denture Base Materials For Aesthetical Removable Partial Denture FrameworkDocument3 pagesFlexible Thermoplastic Denture Base Materials For Aesthetical Removable Partial Denture FrameworkPreuNo ratings yet
- Z-TRACK-METHOD ChecklistDocument5 pagesZ-TRACK-METHOD ChecklistDaniela Villanueva RosalNo ratings yet
- Sushrut Dental Clinic: Dr. Bhagyashree Ramesh Khedkar BDS (Reg No. A-45644)Document1 pageSushrut Dental Clinic: Dr. Bhagyashree Ramesh Khedkar BDS (Reg No. A-45644)Ganesh ganiNo ratings yet
- Spanking Children is Detrimental and Should be OutlawedDocument3 pagesSpanking Children is Detrimental and Should be OutlawedJames MungaiNo ratings yet
- View Point 2 File 10 Teacher Leticia Franco Unit 9 1. Complete The Conversation With Whatever, Whichever, WhoeverDocument8 pagesView Point 2 File 10 Teacher Leticia Franco Unit 9 1. Complete The Conversation With Whatever, Whichever, WhoeverMaisa BassiniNo ratings yet
- Pearson's Correlation Coefficient: BMJ (Online) July 2012Document3 pagesPearson's Correlation Coefficient: BMJ (Online) July 2012Randy Rafael Asencio AlvaradoNo ratings yet
- HRM 370Document6 pagesHRM 370Md. Kamil UddinNo ratings yet
- Martina Caic PHD Dissertation EmbargoChpt3Document180 pagesMartina Caic PHD Dissertation EmbargoChpt3Josh GonzalesNo ratings yet
- Zimmer Nexgen Lps Flex Mobile and Lps Mobile Bearing Knee Surgical Technique PDFDocument68 pagesZimmer Nexgen Lps Flex Mobile and Lps Mobile Bearing Knee Surgical Technique PDFMogildea CristianNo ratings yet
- Welcome Guests & Take Food Orders Session PlanDocument4 pagesWelcome Guests & Take Food Orders Session Planabegail capistranoNo ratings yet
- Australian Beverages OH&S AuditDocument41 pagesAustralian Beverages OH&S AuditPauline VukiNo ratings yet
- METHOD OF STATEMENT Electrical Resistivity Survey (Wenner Four Pin Method)Document9 pagesMETHOD OF STATEMENT Electrical Resistivity Survey (Wenner Four Pin Method)anwar ariffinNo ratings yet
- Geriatric Pearls: Tools For Taking A History and Physical With The Older AdultDocument51 pagesGeriatric Pearls: Tools For Taking A History and Physical With The Older AdultMajid KhanNo ratings yet
- Module 3 Organizational Structure, Job Description and Job EvaluationDocument21 pagesModule 3 Organizational Structure, Job Description and Job EvaluationJasper Mina GerminoNo ratings yet
- Continuous Assessment Termination. UploadDocument6 pagesContinuous Assessment Termination. Uploadstephen BannahNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)