You might also like
- Dr. Pestana's Surgery Notes: Pocket-Sized Review for the Surgical Clerkship and Shelf ExamsFrom EverandDr. Pestana's Surgery Notes: Pocket-Sized Review for the Surgical Clerkship and Shelf ExamsRating: 5 out of 5 stars5/5 (1)
- 500 High Yield Nuggets Step 1Document25 pages500 High Yield Nuggets Step 1AmrAliTaha91% (22)
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1From EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 1Rating: 5 out of 5 stars5/5 (2)
- SURVIVOR'S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 2CK.From EverandSURVIVOR'S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 2CK.Rating: 5 out of 5 stars5/5 (1)
- Biochemistry, Usmle EndpointDocument272 pagesBiochemistry, Usmle EndpointDoctor SalameNo ratings yet
- DirtyUSMLE RocksDocument412 pagesDirtyUSMLE RocksDavid S. Chou90% (30)
- AMSJ USMLE - UWorld Notes & Associations and Clinical Presentations PDFDocument103 pagesAMSJ USMLE - UWorld Notes & Associations and Clinical Presentations PDFERA100% (3)
- USMLE Step 1 Board Exam High Yield Anatomy For MedicineDocument7 pagesUSMLE Step 1 Board Exam High Yield Anatomy For Medicinesirp328100% (2)
- USMLE PathognomicsDocument9 pagesUSMLE PathognomicsMatt McGlothlin94% (18)
- SURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3From EverandSURVIVOR’S GUIDE Quick Reviews and Test Taking Skills for USMLE STEP 3Rating: 5 out of 5 stars5/5 (1)
- Muscle ChartDocument16 pagesMuscle Chartphinee1692% (13)
- Antibiotics - Compleate ClassificationDocument2 pagesAntibiotics - Compleate ClassificationNeal Gupta83% (12)
- Usmle Step 2 CK Recalls 2021 3jz DR NotesDocument22 pagesUsmle Step 2 CK Recalls 2021 3jz DR Notesmed student100% (2)
- Step 1 Uworld PDFDocument25 pagesStep 1 Uworld PDFRegents Park Business Center100% (1)
- UWORLD Notes by Subject (Main Division) (Usmle Grassroots)Document80 pagesUWORLD Notes by Subject (Main Division) (Usmle Grassroots)Mital Bhakta83% (18)
- Pharmacology Usmle Step 1Document5 pagesPharmacology Usmle Step 1raj_1041100% (15)
- 28-DAY MED STUDY SCHEDULEDocument13 pages28-DAY MED STUDY SCHEDULEgemazy123100% (3)
- High Yield Image Plates Gross - Patholog PDFDocument151 pagesHigh Yield Image Plates Gross - Patholog PDFld100% (2)
- DR - BD S Step 1 Guide - PDF Filename UTF-8 DR - BD S Step 1 GuideDocument24 pagesDR - BD S Step 1 Guide - PDF Filename UTF-8 DR - BD S Step 1 GuideAdeelMunawarNo ratings yet
- Essential Medical Concepts and TerminologyDocument3 pagesEssential Medical Concepts and TerminologyMedStudent7650% (4)
- USMLE STEP 1 and STEP 2 Highly Tested Topics Gold CollectionDocument36 pagesUSMLE STEP 1 and STEP 2 Highly Tested Topics Gold CollectionBalto100% (1)
- Mnemonics For USMLE Step 1Document33 pagesMnemonics For USMLE Step 1Sara Sabra100% (9)
- USMLE First Aid Classic Findings - Flash CardsDocument56 pagesUSMLE First Aid Classic Findings - Flash CardsSaeed Hasan100% (1)
- Endocrine, USMLE ENDPOINTDocument73 pagesEndocrine, USMLE ENDPOINTDaNy Chiriac50% (2)
- 002367889dissecting The USMLE - BookmarkedDocument629 pages002367889dissecting The USMLE - BookmarkedPharAway100% (6)
- USMLE Step 1 Success Story - How I Scored 254Document6 pagesUSMLE Step 1 Success Story - How I Scored 254Nada AKNo ratings yet
- Step 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies 2nd Edition: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- Step 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionFrom EverandStep 3 Board-Ready USMLE Junkies: The Must-Have USMLE Step 3 Review CompanionNo ratings yet
- How to Create a Study Plan for the USMLE Step 1From EverandHow to Create a Study Plan for the USMLE Step 1Rating: 4.5 out of 5 stars4.5/5 (11)
- Agrochemical Product Expiry DatesDocument64 pagesAgrochemical Product Expiry Datesjayesmine barlongayNo ratings yet
- Gap Junction: Tibial Nerve FunctionDocument9 pagesGap Junction: Tibial Nerve FunctionRevant AgarwalNo ratings yet
- Step 1 HintsDocument4 pagesStep 1 HintsKelvin Aquino GallozaNo ratings yet
- Step 1 DrugsDocument19 pagesStep 1 Drugssplinter59490% (20)
- Jefferson - Aoa USMLE Step 1Document12 pagesJefferson - Aoa USMLE Step 1Mc Ase100% (1)
- High Yield Microbiology ImagesDocument73 pagesHigh Yield Microbiology ImagesSana Savana Aman RNo ratings yet
- USMLE Step 1 Radiology Buzzwords - USMLE ForumsDocument5 pagesUSMLE Step 1 Radiology Buzzwords - USMLE Forumsfrabzi100% (2)
- NBME 15 QuizletDocument12 pagesNBME 15 Quizletrmelendez00192% (12)
- Penicillins Pen&G Pen&V: T.%pallidum% (Syphilis)Document1 pagePenicillins Pen&G Pen&V: T.%pallidum% (Syphilis)gregoryvo100% (5)
- Usmle CluesDocument86 pagesUsmle CluesAlejandro Bocanegra Osuna100% (8)
- USMLE Step 1 NotesDocument7 pagesUSMLE Step 1 Notesmojda100% (1)
- List of Forgettables - What You Need To Review Few Days Before The Exam - USMLE ForumsDocument1 pageList of Forgettables - What You Need To Review Few Days Before The Exam - USMLE ForumsJahanzeb AhmedNo ratings yet
- Usmle Classic CluesDocument10 pagesUsmle Classic CluesfrabziNo ratings yet
- Step 1 USMLE NotesDocument15 pagesStep 1 USMLE Notes13un391543100% (1)
- NBME ChecklistDocument3 pagesNBME ChecklistDinesh Kumar ReddyNo ratings yet
- Step 1 271 Feb 10, 2021Document5 pagesStep 1 271 Feb 10, 2021Bireera AhmedNo ratings yet
- Usmle Hy Images: By: MeduploaderDocument62 pagesUsmle Hy Images: By: Meduploaderdamodarpatil100% (18)
- NBME 5 Review: Multiple Myeloma Block 1Document21 pagesNBME 5 Review: Multiple Myeloma Block 1Vivian Tamara Suárez89% (9)
- How I Scored A 270 On USMLE Step 1Document7 pagesHow I Scored A 270 On USMLE Step 1sankgupta100% (1)
- 265 Experience - Abdelrahman Abusaif PDFDocument6 pages265 Experience - Abdelrahman Abusaif PDFAz Tebba100% (4)
- High Yield Notes From UW Q BlocksDocument159 pagesHigh Yield Notes From UW Q BlocksKunal Sharma100% (5)
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
- Guide for Residency and Fellowship in the USA as an International Medical GraduateFrom EverandGuide for Residency and Fellowship in the USA as an International Medical GraduateNo ratings yet
- U.S. MEDICAL LICENSING EXAM (USMLE) STEP III – Patient Management: Passbooks Study GuideFrom EverandU.S. MEDICAL LICENSING EXAM (USMLE) STEP III – Patient Management: Passbooks Study GuideNo ratings yet
- Patan Academy of Health SciencesDocument1 pagePatan Academy of Health Sciencesomy yadavNo ratings yet
- Memory and Medical MnemonicsDocument33 pagesMemory and Medical Mnemonicsrandiey john abelleraNo ratings yet
- Memory and Medical MnemonicsDocument33 pagesMemory and Medical Mnemonicsrandiey john abelleraNo ratings yet
- Biochemistry One Liner PDFDocument13 pagesBiochemistry One Liner PDFMinaz PatelNo ratings yet
- Drug List by Therapeutic Category: Cardiovascular DrugsDocument7 pagesDrug List by Therapeutic Category: Cardiovascular DrugsAloah122346No ratings yet
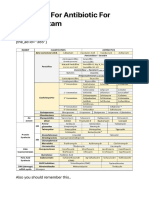
- Summary For Antibiotic For USMLE Exam - USMLE MATERIALS - Updated USMLE Study DataDocument5 pagesSummary For Antibiotic For USMLE Exam - USMLE MATERIALS - Updated USMLE Study Dataomy yadavNo ratings yet
- Hypoglycemia Hypoglycemia: @biochemistryconceptsDocument22 pagesHypoglycemia Hypoglycemia: @biochemistryconceptsomy yadavNo ratings yet
- The Actions of Sympathetic and Parasympathetic Divisions On OrgansDocument1 pageThe Actions of Sympathetic and Parasympathetic Divisions On Organsomy yadavNo ratings yet
- Gi and HepatoDocument14 pagesGi and Hepatoomy yadavNo ratings yet
- Insecticides / Pesticides Registered Under Section 9 (3) of The Insecticides Act, 1968 For Use in The CountryDocument7 pagesInsecticides / Pesticides Registered Under Section 9 (3) of The Insecticides Act, 1968 For Use in The Countrybabji dudekulaNo ratings yet
- Pesticides 2015 - Full BookDocument297 pagesPesticides 2015 - Full BookTushar Savaliya100% (1)
- Insecticide Mode of Action Classification GuideDocument6 pagesInsecticide Mode of Action Classification GuideJose Natividad Flores MayoriNo ratings yet
- Antifungal PDFDocument3 pagesAntifungal PDFFaten SarhanNo ratings yet
- EUCAST System For Antimicrobial Abbreviations: Method For Selection of A Unique Three-Letter CodeDocument2 pagesEUCAST System For Antimicrobial Abbreviations: Method For Selection of A Unique Three-Letter CodeMarcelo UGNo ratings yet
- Antibiotics Spreadsheet 2004-1215Document1 pageAntibiotics Spreadsheet 2004-1215palak32No ratings yet
- Summary For Antibiotic For USMLE Exam - USMLE MATERIALS - Updated USMLE Study DataDocument5 pagesSummary For Antibiotic For USMLE Exam - USMLE MATERIALS - Updated USMLE Study Dataomy yadavNo ratings yet
- AsoDocument3 pagesAsoKedokteran ShopNo ratings yet
- Registered Pesticide 1 Oct 2007 - 1 Sept 2012Document312 pagesRegistered Pesticide 1 Oct 2007 - 1 Sept 2012marzuki2870% (1)
- List of AntibioticsDocument9 pagesList of Antibioticsdesi_mNo ratings yet
- 429 RC MinutesDocument286 pages429 RC MinutesManoj MistariNo ratings yet
- PSA Labeled Sanitizers For ProduceDocument71 pagesPSA Labeled Sanitizers For ProduceGabriel JZedd Pisfil SuclupeNo ratings yet
- Antibiotics SummaryDocument4 pagesAntibiotics SummaryKamaI AzizNo ratings yet
- Inventario de Productos QuimicosDocument8 pagesInventario de Productos QuimicosGerardo Adrián Terceros ZorrillaNo ratings yet
- Pt. Nufarm Indonesia Sales Budget 2010/2011 - Territory: Riau - PLTDocument24 pagesPt. Nufarm Indonesia Sales Budget 2010/2011 - Territory: Riau - PLTRIZKINo ratings yet
- 2021 Tennessee Weed Control GuideDocument111 pages2021 Tennessee Weed Control GuideAllanNo ratings yet
- How Do Antibiotics Work - AntibioticsDocument1 pageHow Do Antibiotics Work - AntibioticsBrigitte Fani FlorenciaNo ratings yet
- Insecticide GroupsDocument2 pagesInsecticide GroupsJuan Luis Herrera YañezNo ratings yet
- Pesticide PollutionDocument6 pagesPesticide PollutionBinodBasnetNo ratings yet
- Production List of NTGC: Zhejiang Medicines and Health Products Imp & Exp. Co., LTDDocument2 pagesProduction List of NTGC: Zhejiang Medicines and Health Products Imp & Exp. Co., LTDMarius Ponzhi VillafuenteNo ratings yet
- Price List E-Katalog 20Document1 pagePrice List E-Katalog 20Kuncoro Ambra ZNo ratings yet
- Anti-Bakteri Formularium GuideDocument14 pagesAnti-Bakteri Formularium GuideNilam atika sariNo ratings yet
- Kemampuan Sabun Antiseptik Cair Yang Mengandung Triclosan Yang Terdaftar Di BPOM Dalam Menghambat Pertumbuhan Bakteri Escherichia ColiDocument8 pagesKemampuan Sabun Antiseptik Cair Yang Mengandung Triclosan Yang Terdaftar Di BPOM Dalam Menghambat Pertumbuhan Bakteri Escherichia ColiNurazizah Asmani10No ratings yet
- Suncrop Pesticide Price ListDocument3 pagesSuncrop Pesticide Price Listraaa guy69% (16)
- Suppliers MasterfileDocument150 pagesSuppliers Masterfilejayesmine barlongay100% (1)
- 5 1 Quantamatrix 1 MKT Bdra1en A - DrastDocument2 pages5 1 Quantamatrix 1 MKT Bdra1en A - DrastBilgi KurumsalNo ratings yet
- Ecolab Supplier Part Numbers and DescriptionsDocument14 pagesEcolab Supplier Part Numbers and DescriptionsMOGES ABERANo ratings yet
- PH Water On Stability PesticidesDocument6 pagesPH Water On Stability PesticidesMontoya AlidNo ratings yet