You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Hack and SlashDocument38 pagesHack and Slashyo100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Quantitative Aptitude Shortcuts & TricksDocument14 pagesQuantitative Aptitude Shortcuts & Tricksrock_on_rupz99No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2015 Nissan Service Maintenance GuideDocument70 pages2015 Nissan Service Maintenance GuideAhmed Almaghrby100% (2)
- The Heart and The Cave (René Guénon) PDFDocument3 pagesThe Heart and The Cave (René Guénon) PDFIsrael100% (1)
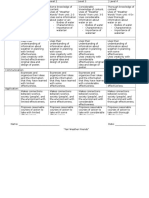
- Science Culminating Task RubricDocument2 pagesScience Culminating Task Rubricapi-311644452No ratings yet
- Study Abroad Consultant in PanchkulaDocument17 pagesStudy Abroad Consultant in Panchkulashubham mehtaNo ratings yet
- International Rice Research Notes Vol.31 No.1Document47 pagesInternational Rice Research Notes Vol.31 No.1ccquintos0% (1)
- 5-PICO Critical Appraisal of RCTDocument11 pages5-PICO Critical Appraisal of RCTRama BayuNo ratings yet
- TLE-ICT-Technical Drafting Grade 10 LMDocument175 pagesTLE-ICT-Technical Drafting Grade 10 LMHari Ng Sablay87% (113)
- Cubex 6200 Spec Sheet PDFDocument4 pagesCubex 6200 Spec Sheet PDFtharciocidreira0% (1)
- DERRIDA The Principle of Hospitality PDFDocument5 pagesDERRIDA The Principle of Hospitality PDFjeronimomiloneNo ratings yet
- COT 1 - (Science 7) - Cell To Biosphere 4as Semi-Detailed LPDocument10 pagesCOT 1 - (Science 7) - Cell To Biosphere 4as Semi-Detailed LPARLENE AGUNOD100% (1)
- Chlampah,+ejournal+dr +chan+Document7 pagesChlampah,+ejournal+dr +chan+Rama BayuNo ratings yet
- 675-Article Text-1214-1-10-20210608Document7 pages675-Article Text-1214-1-10-20210608Rama BayuNo ratings yet
- Anaesthesia - 2009 - Danelli - Ultrasound Vs Nerve Stimulation Multiple Injection Technique For Posterior Popliteal SciaticDocument5 pagesAnaesthesia - 2009 - Danelli - Ultrasound Vs Nerve Stimulation Multiple Injection Technique For Posterior Popliteal SciaticRama BayuNo ratings yet
- 4513 10918 1 PB PDFDocument13 pages4513 10918 1 PB PDFRama BayuNo ratings yet
- Depression, Anxiety, Stress, and Dysmenorrhea: A Protocol For A Systematic ReviewDocument6 pagesDepression, Anxiety, Stress, and Dysmenorrhea: A Protocol For A Systematic ReviewRama BayuNo ratings yet
- The Immediate Effects of Foam Rolling and Stretching On Iliotibial Band Stiffness: A Randomized Controlled TrialDocument11 pagesThe Immediate Effects of Foam Rolling and Stretching On Iliotibial Band Stiffness: A Randomized Controlled TrialRama BayuNo ratings yet
- HINT - High Level Inferencing Tool: An Expert System For The Interpretation of Neurophysiological StudiesDocument18 pagesHINT - High Level Inferencing Tool: An Expert System For The Interpretation of Neurophysiological StudiesRama BayuNo ratings yet
- Single Channel EMG Classification With Ensemble Empirical Mode Decomposition Based ICA For Diagnosing Neuromuscular DisordersDocument10 pagesSingle Channel EMG Classification With Ensemble Empirical Mode Decomposition Based ICA For Diagnosing Neuromuscular DisordersRama BayuNo ratings yet
- Opportunities For Early Intervention Based On Theory, Basic Neuroscience, and Clinical ScienceDocument13 pagesOpportunities For Early Intervention Based On Theory, Basic Neuroscience, and Clinical ScienceRama BayuNo ratings yet
- Kelompok 3 Epidemologi (Diagnostik)Document4 pagesKelompok 3 Epidemologi (Diagnostik)Rama BayuNo ratings yet
- Dr. Siswo Poerwanto MPH, MSCDocument25 pagesDr. Siswo Poerwanto MPH, MSCRama BayuNo ratings yet
- Terapi Latihan 2019 ADocument1 pageTerapi Latihan 2019 ARama BayuNo ratings yet
- CCS PDFDocument12 pagesCCS PDFRama BayuNo ratings yet
- Null Hypothesis Ho: P PoDocument3 pagesNull Hypothesis Ho: P PoRama BayuNo ratings yet
- Junal ScreeningDocument9 pagesJunal ScreeningRama BayuNo ratings yet
- EssayDocument2 pagesEssaySantoshKumarPatraNo ratings yet
- Seloka: Jurnal Pendidikan Bahasa Dan Sastra Indonesia: Susilo Rini & WagiranDocument7 pagesSeloka: Jurnal Pendidikan Bahasa Dan Sastra Indonesia: Susilo Rini & Wagiranareni yulitawatiNo ratings yet
- 123ignition Mercedes 200 230 T C W123 M115 Online-ShopDocument1 page123ignition Mercedes 200 230 T C W123 M115 Online-ShophundalNo ratings yet
- mathematicsproficiencyattitudeandperformanceofgrade9studentsinprivatehighschoolsinBukidnonPhilippines PDFDocument15 pagesmathematicsproficiencyattitudeandperformanceofgrade9studentsinprivatehighschoolsinBukidnonPhilippines PDFNacivah BasherNo ratings yet
- Selected Objective Question On Introduction To Computers With Answer Set 5Document27 pagesSelected Objective Question On Introduction To Computers With Answer Set 5Ankit JainNo ratings yet
- Introducing The True Ekklesia of Jesus ChristDocument5 pagesIntroducing The True Ekklesia of Jesus ChristRamil Moreno SumangilNo ratings yet
- Price List 2020-21Document3 pagesPrice List 2020-21Nikhil SalujaNo ratings yet
- Descriptive Statistics I Theory Questions (1997-2016)Document9 pagesDescriptive Statistics I Theory Questions (1997-2016)Satyaki GhosalNo ratings yet
- FDARDocument2 pagesFDARMikaella JumandosNo ratings yet
- How Could Auto Manufacturer Use Transportation To Increase The Efficiency of Supply Chain?Document25 pagesHow Could Auto Manufacturer Use Transportation To Increase The Efficiency of Supply Chain?guddianushaNo ratings yet
- Pioneer QX 747 BrochureDocument6 pagesPioneer QX 747 BrochureArmando JimenezNo ratings yet
- Knowage Baby Steps PDFDocument230 pagesKnowage Baby Steps PDFworkflow m3cNo ratings yet
- Automatic Workload Management With RACDocument32 pagesAutomatic Workload Management With RACKe JuNo ratings yet
- ProgramDetails PDF 134Document2 pagesProgramDetails PDF 134samyakgaikwad12No ratings yet
- Star Delta Transformation: Dr.V.Joshi ManoharDocument14 pagesStar Delta Transformation: Dr.V.Joshi ManoharhariNo ratings yet
- Criminal Law - Aggravating CircumstancesDocument9 pagesCriminal Law - Aggravating Circumstancesabo8008No ratings yet
- JLG Skytrak Telehandler 6042 Operation Service Parts ManualsDocument22 pagesJLG Skytrak Telehandler 6042 Operation Service Parts Manualschristyross211089ntz100% (133)
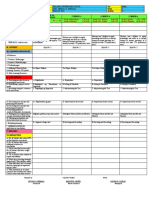
- DLL Q3 Week 4 Day5 WWDocument3 pagesDLL Q3 Week 4 Day5 WWCecilia Guevarra DumlaoNo ratings yet
- Hsep-05 - Communication, Participation & ConsultationDocument6 pagesHsep-05 - Communication, Participation & ConsultationScha AffinNo ratings yet