You might also like
- Comprehensive Guidelines For Management of COVID-19 In: ChildrenDocument11 pagesComprehensive Guidelines For Management of COVID-19 In: ChildrenAyushi GuptaNo ratings yet
- Asymptomatic Severe Moderate Mild: Comprehensive Guidelines For Management of COVID-19 PatientsDocument9 pagesAsymptomatic Severe Moderate Mild: Comprehensive Guidelines For Management of COVID-19 PatientsVaishnavi JayakumarNo ratings yet
- Guidelines For Management of COVID-19 in Children (Below 18 Years)Document10 pagesGuidelines For Management of COVID-19 in Children (Below 18 Years)Juhi NeogiNo ratings yet
- Management of ARIDocument33 pagesManagement of ARISam christenNo ratings yet
- Bronchiolitis - The Quick Guide: Assessment of Severity of DiseaseDocument2 pagesBronchiolitis - The Quick Guide: Assessment of Severity of Diseasebaiq dessyNo ratings yet
- Comprehensive Guidelines For Management of COVID-19 In: Children AdolescentsDocument12 pagesComprehensive Guidelines For Management of COVID-19 In: Children AdolescentsDheeraj kambleNo ratings yet
- Session 4-Management of Paediatric COVID19Document24 pagesSession 4-Management of Paediatric COVID19Uncertain NeuronNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- Asthma Guidelines 2016Document21 pagesAsthma Guidelines 2016Varun ArunagiriNo ratings yet
- What We Should Know About COVID-19!Document25 pagesWhat We Should Know About COVID-19!Frank ThomasNo ratings yet
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- Child With Fever in ER Non Covid 19Document6 pagesChild With Fever in ER Non Covid 19Suwandi AlghozyNo ratings yet
- Febrile Convulsion UHL Paediatric Emergency Department GuidelineDocument4 pagesFebrile Convulsion UHL Paediatric Emergency Department GuidelineAmila ShyamalNo ratings yet
- Peds 2 - Pulmonary Disorders of ChildrenDocument27 pagesPeds 2 - Pulmonary Disorders of ChildrenMinh Nguyễn Phương HồngNo ratings yet
- Febrile ConvulsionDocument8 pagesFebrile ConvulsionKo NgeNo ratings yet
- Home Care For CovidDocument18 pagesHome Care For CovidiSmayli (smyle-smayl)No ratings yet
- Common Pediatric Illnesses in The Er UrgentDocument46 pagesCommon Pediatric Illnesses in The Er UrgentDr mohamedNo ratings yet
- Directorate General of Health Services, Mohfw, Goi Comprehensive Guidelines For Management of Covid-19 Patients Asymptomatic Mild Moderate SevereDocument2 pagesDirectorate General of Health Services, Mohfw, Goi Comprehensive Guidelines For Management of Covid-19 Patients Asymptomatic Mild Moderate SevereSpecial OPD SVMCHRCNo ratings yet
- Pediatric Therapeutics 2020Document36 pagesPediatric Therapeutics 2020Dheeraj46No ratings yet
- Barnet Primary Care Guide During Covid-19: Contents PageDocument32 pagesBarnet Primary Care Guide During Covid-19: Contents PageGreta Tanushi KukaNo ratings yet
- The Mcmaster Pediatric Curriculum: at NightDocument29 pagesThe Mcmaster Pediatric Curriculum: at NightFrancia ToledanoNo ratings yet
- TreatmentProtocol 10-4-2021Document3 pagesTreatmentProtocol 10-4-2021Anishk SinghNo ratings yet
- NG Acute PoisoningDocument7 pagesNG Acute Poisoningshaker al baharNo ratings yet
- COVID Homecare Tips by 1mgDocument27 pagesCOVID Homecare Tips by 1mgprdNo ratings yet
- Laboratory Confirmed Covid 19 Patient: Department of Health & Family Welfare, Govt of West BengalDocument2 pagesLaboratory Confirmed Covid 19 Patient: Department of Health & Family Welfare, Govt of West BengalSujoyDeNo ratings yet
- Care of The Child Applying Integrated Management of Childhood Illnesses (Imci)Document22 pagesCare of The Child Applying Integrated Management of Childhood Illnesses (Imci)Jesena SalveNo ratings yet
- Katie Doran, DO FAAP Division of Urgent Care Children's Mercy Hospital October 17, 2019Document36 pagesKatie Doran, DO FAAP Division of Urgent Care Children's Mercy Hospital October 17, 2019wisnusigitpratamaNo ratings yet
- F Seizures AssessDocument1 pageF Seizures Assessmahmudajannatul.7No ratings yet
- Consult Training 1Document9 pagesConsult Training 1Lumos MaximaNo ratings yet
- Conditions of The GITTDocument4 pagesConditions of The GITTPGDME 20192020No ratings yet
- Well Baby 2020 With NotesDocument119 pagesWell Baby 2020 With NotesSamsam Almarez BacaltosNo ratings yet
- 1.nurse Preparedness Training Against 3rd Wave of CovidDocument52 pages1.nurse Preparedness Training Against 3rd Wave of CovidyeshumasihNo ratings yet
- Respiratory Tract Infections - Med DidacticsDocument59 pagesRespiratory Tract Infections - Med Didacticsapi-649060644No ratings yet
- Mental Health and Psychosocial Resilience in The Time of PandemicDocument64 pagesMental Health and Psychosocial Resilience in The Time of Pandemicreginald_adia_1No ratings yet
- Integrated Management of Childhood Illness: Group 1Document31 pagesIntegrated Management of Childhood Illness: Group 1Alex AntipordaNo ratings yet
- COVID-19 Home - GuideDocument14 pagesCOVID-19 Home - GuidecyruskuleiNo ratings yet
- Neonatal Jaundice: Miriti M.D Master of Clinical Medicine:Accidents and Emerrgency MAY 2018Document25 pagesNeonatal Jaundice: Miriti M.D Master of Clinical Medicine:Accidents and Emerrgency MAY 2018Dennis MiritiNo ratings yet
- Smart Antibiotics Use in Children With SBI - HandoutDocument44 pagesSmart Antibiotics Use in Children With SBI - HandoutAlbertNo ratings yet
- ch2 fs1Document2 pagesch2 fs1ry beNo ratings yet
- Guidelines For DoctorsDocument4 pagesGuidelines For DoctorsNazar KaNo ratings yet
- Self Care Guide Pantai 1Document33 pagesSelf Care Guide Pantai 1puterishaliza272No ratings yet
- Neonatal SepsisDocument20 pagesNeonatal SepsisJustine Nyangaresi100% (1)
- Refluxver 23Document31 pagesRefluxver 23Osman Bin SaifNo ratings yet
- Hypoglycemia (Moderate or Severe) Diabetic Ketoacidosis (DKA)Document1 pageHypoglycemia (Moderate or Severe) Diabetic Ketoacidosis (DKA)Hanouf BakriNo ratings yet
- COVID Homecare V2 20210426Document3 pagesCOVID Homecare V2 20210426Vishal TNo ratings yet
- Course of Illness:: ClassificationDocument2 pagesCourse of Illness:: ClassificationKrista P. AguinaldoNo ratings yet
- HFMD Protocol For KK & District Hosp 01082018Document16 pagesHFMD Protocol For KK & District Hosp 01082018Yui HirasawaNo ratings yet
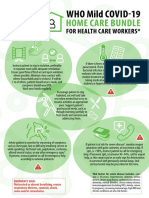
- WHO COVID-19-Home-Care-BundleDocument2 pagesWHO COVID-19-Home-Care-BundleOCSAF - P2LT PUNSALAN MCNo ratings yet
- Pneumonia AdultDocument1 pagePneumonia AdultRoi LevinzonNo ratings yet
- Asthma OSCE Jamie TanDocument5 pagesAsthma OSCE Jamie TanAini Afifah HuzaimyNo ratings yet
- A. Background of The StudyDocument43 pagesA. Background of The StudyJohn Robert CruzNo ratings yet
- Note On Asthma in AdultDocument5 pagesNote On Asthma in Adultshivam1969No ratings yet
- Hiv Co-Morbidities, Ois and NcdsDocument49 pagesHiv Co-Morbidities, Ois and NcdszawadiNo ratings yet
- Pedi Pearls 2 - Scrubed PDFDocument46 pagesPedi Pearls 2 - Scrubed PDFthomasfx10100% (1)
- Acute Respiratory InfectionDocument68 pagesAcute Respiratory InfectionArun GeorgeNo ratings yet
- 3B2 Preceptorial Nov 18 SFSeizuresDocument79 pages3B2 Preceptorial Nov 18 SFSeizuresAbigail PaasaNo ratings yet
- Vaccine BrandsDocument4 pagesVaccine BrandskarnaNo ratings yet
- SSC COVID19GuidelinesRecTable FirstUpdateDocument5 pagesSSC COVID19GuidelinesRecTable FirstUpdatesatya.drNo ratings yet
- Meity To PlatformsDocument2 pagesMeity To PlatformsVaibhav TiwariNo ratings yet
- Covidshield DelhiDocument1 pageCovidshield DelhiVaibhav TiwariNo ratings yet
- Delhi CovaxinDocument1 pageDelhi CovaxinVaibhav TiwariNo ratings yet
- MHAorderdt 27012021Document7 pagesMHAorderdt 27012021Vaibhav TiwariNo ratings yet
- Rheumatology 2012 MrcppassDocument131 pagesRheumatology 2012 Mrcppasslittle luluNo ratings yet
- 2-d Echo With Doppler: Prepared by Kurfessa, AbdisaDocument7 pages2-d Echo With Doppler: Prepared by Kurfessa, AbdisaAb Staholic BoiiNo ratings yet
- Dual Antiplatelet Therapy Clopidogrel With Low-Dose Cilostazol Intensifies Platelet Inhibition in Patients With Ischemic StrokeDocument5 pagesDual Antiplatelet Therapy Clopidogrel With Low-Dose Cilostazol Intensifies Platelet Inhibition in Patients With Ischemic StrokeDhanang Prawira NugrahaNo ratings yet
- What Shoull You Do in Sudden Cardiac ArrestDocument31 pagesWhat Shoull You Do in Sudden Cardiac ArrestAlban RamadhanNo ratings yet
- Thoracic SurgeryDocument178 pagesThoracic SurgeryArthur Pendragon100% (1)
- CVS ExaminationDocument85 pagesCVS ExaminationPrasenjit DasNo ratings yet
- WSDDocument13 pagesWSDhinatakunhinata75No ratings yet
- The Child With Hematologic DisordersDocument149 pagesThe Child With Hematologic DisordersNics FranciscoNo ratings yet
- Cerebellar StrokeDocument12 pagesCerebellar StrokewhitecloudsNo ratings yet
- A Drug Study On: Furosemide TabletDocument7 pagesA Drug Study On: Furosemide TabletRaijenne VersolaNo ratings yet
- NAHCO3Document2 pagesNAHCO3Krizha Angela NicolasNo ratings yet
- Ch. 4 TissuesDocument55 pagesCh. 4 TissuesBora YaNo ratings yet
- Dr. Warsinggih, SP.B-KBD (SLIDE ERAS in Digestive Surgery)Document34 pagesDr. Warsinggih, SP.B-KBD (SLIDE ERAS in Digestive Surgery)dewiswahyuNo ratings yet
- Common MurmurDocument2 pagesCommon MurmurKyWoNo ratings yet
- Thorax Anatomy..Document21 pagesThorax Anatomy..Dungani AllanNo ratings yet
- Unit 4 (7) Origin and Conduction of Cardiac ImpulsesDocument31 pagesUnit 4 (7) Origin and Conduction of Cardiac ImpulsesDINAMANI 0inamNo ratings yet
- 4 Valvular Heart Disease#36f7Document40 pages4 Valvular Heart Disease#36f7Natasha LiberisNo ratings yet
- Classifications of Heart MurmursDocument2 pagesClassifications of Heart MurmursVS100% (2)
- Mock 2Document40 pagesMock 2Syali Sasidharan100% (2)
- Lab Exercise Digestive System Bautista Maria LuisaDocument9 pagesLab Exercise Digestive System Bautista Maria LuisaEricka ElloNo ratings yet
- Compre PE and ROSDocument7 pagesCompre PE and ROSBatch V Med 2 SY 21-22No ratings yet
- 9 Wireframe DocumentDocument7 pages9 Wireframe Documentharshaddanawale.nbnssoe.compNo ratings yet
- Interpretation Chest X RayDocument127 pagesInterpretation Chest X RayVimal NishadNo ratings yet
- Summary of ECG AbnormalitiesDocument8 pagesSummary of ECG AbnormalitiesChristine Nancy NgNo ratings yet
- Science Reviewer - Respiratory and Circulatory SystemDocument2 pagesScience Reviewer - Respiratory and Circulatory SystemMaribeth Villanueva100% (2)
- Seminar - Heart FailuerDocument19 pagesSeminar - Heart Failuermustafalotfy01No ratings yet
- Diabetic Ketoacidosis in ChildrenDocument6 pagesDiabetic Ketoacidosis in ChildrenviharadewiNo ratings yet
- Night Sweats: A Systematic Review of The LiteratureDocument16 pagesNight Sweats: A Systematic Review of The Literaturedevin mahendikaNo ratings yet
- Uworld - PEDIATRICSDocument50 pagesUworld - PEDIATRICSNikxy100% (1)
- The Cardiac Cycle NotesDocument5 pagesThe Cardiac Cycle NotesAsad Khan Khalil100% (1)